Glomerular nephritis
Reading File
Finding Sources
Searching PubMed
"glomerulonephritis"[MeSH Terms] AND "diagnosis" AND "treatment"
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
I now have rich, comprehensive content from multiple authoritative textbooks. Let me compose the full response:
Glomerulonephritis (GN)
Glomerulonephritis refers to a group of inflammatory conditions that damage the glomerular capillary loops, leading to impaired filtration, hematuria, proteinuria, and progressive renal failure. It can be primary (limited to the kidney) or secondary (part of a systemic disease).
Glomerular Anatomy - The Target of Disease
The glomerulus has three filtration layers that GN disrupts:
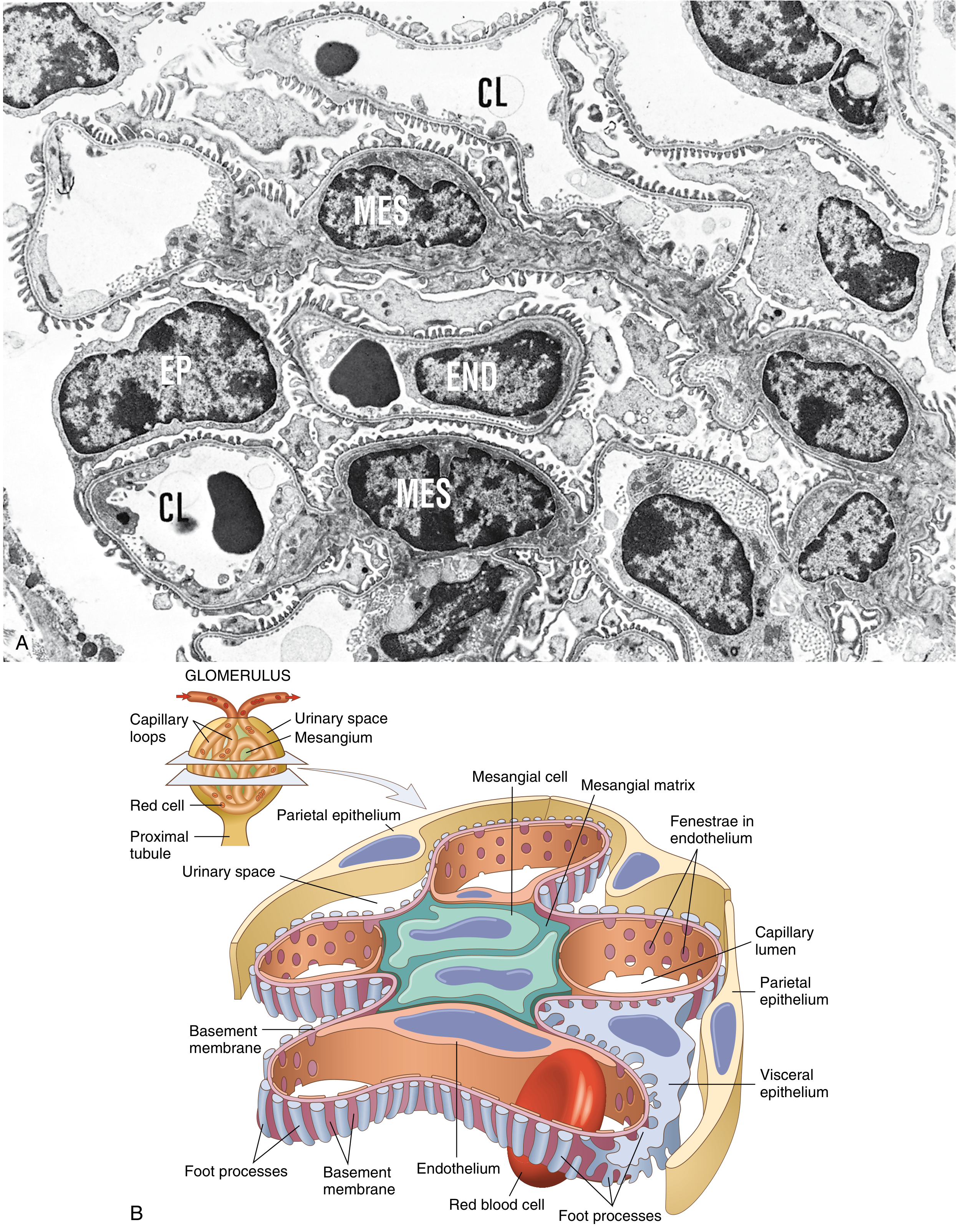
Glomerular structure: (A) electron micrograph and (B) detailed schematic. - Robbins, Cotran & Kumar Pathologic Basis of Disease
Pathogenesis
Most GN is immunologically mediated. The major mechanisms are:
1. In Situ Immune Complex Formation
Antibodies react with intrinsic glomerular antigens (e.g., anti-GBM antibodies in Goodpasture disease targeting the α3 chain of type IV collagen NC1 domain). This produces linear immunofluorescence (IF) staining.
2. Circulating Immune Complex Deposition
Circulating antigen-antibody complexes are trapped in the glomerulus. Produces granular IF staining. Examples: post-streptococcal GN, lupus nephritis, hepatitis B/C.
3. Pauci-Immune / ANCA-Mediated
Neutrophils activated by anti-neutrophil cytoplasmic antibodies (ANCA) damage glomeruli without significant immune deposits on IF.
4. Cell-Mediated Immunity
Sensitized T cells contribute to injury and progression in crescentic GN.
5. Alternative Complement Pathway Activation
Dysregulation of the complement alternative pathway leads to C3 glomerulopathy (dense deposit disease, C3 GN).
The location of immune complex deposition determines the histologic pattern:
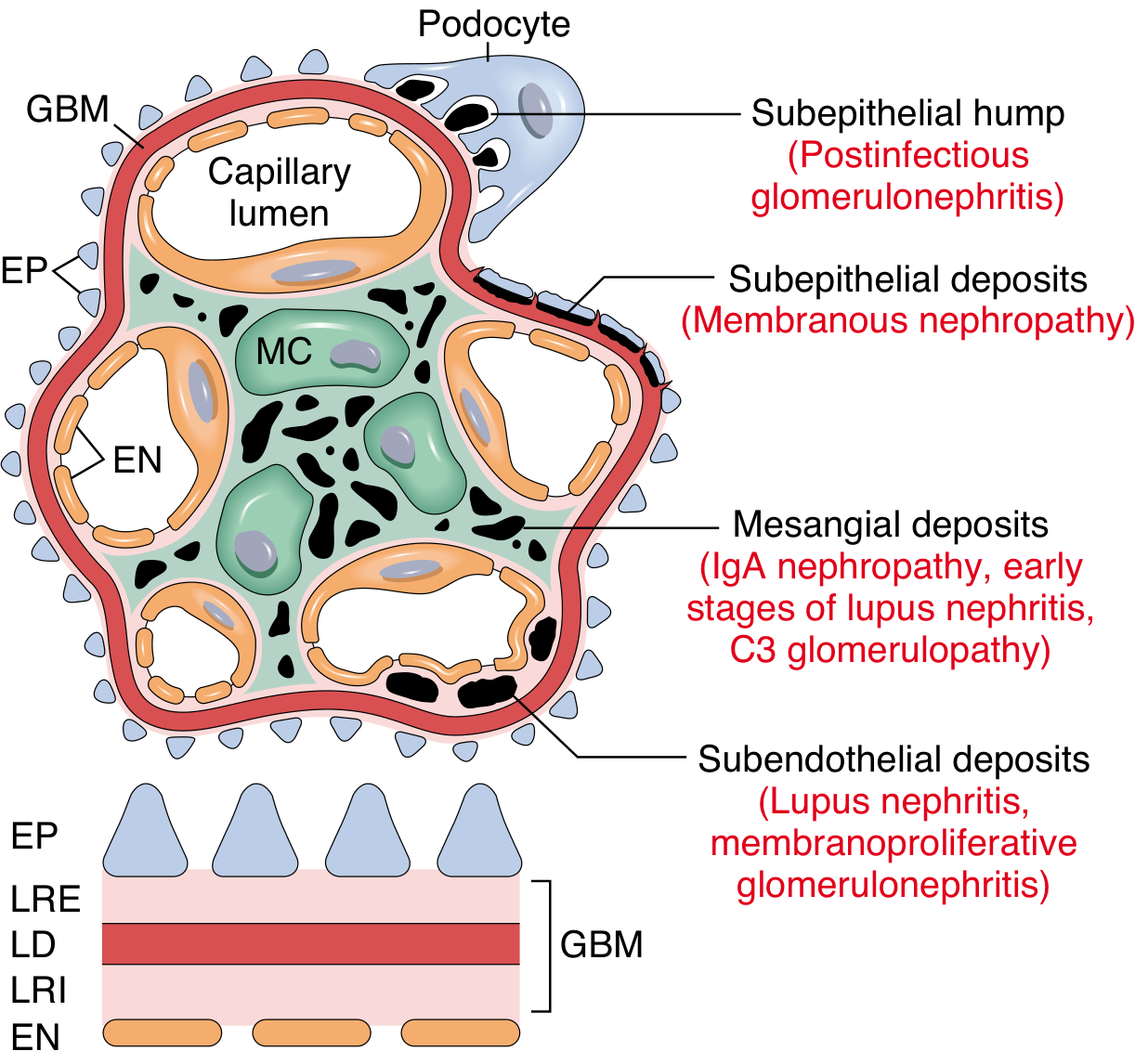
Immune deposit localization and the corresponding disease - Robbins, Cotran & Kumar, p. 834
Mediators of injury include oxidants, proteases, cytokines, complement activation, and growth factors such as TGF-β, which drives eventual glomerulosclerosis. - Goldman-Cecil Medicine, p. 1255
Clinical Presentation: The Nephritic Syndrome
GN classically produces the nephritic syndrome:
| Feature | Description |
|---|---|
| Hematuria | Dark/smoky/cola-colored urine; RBC casts on urinalysis |
| Oliguria | Reduced urine output |
| Hypertension | From volume expansion |
| Azotemia | Elevated BUN/creatinine |
| Proteinuria | Variable - subnephrotic to nephrotic range |
| Active sediment | RBC casts, leukocytes, granular casts |
On light microscopy, GN is characterized by glomerular hypercellularity from: (1) infiltrating neutrophils and monocytes, (2) proliferation of resident mesangial/endothelial cells, or (3) extracapillary crescent formation.
Classification: Major Types of GN
Nephritic Pattern (Proliferative)
1. Acute Postinfectious (Post-streptococcal) GN
- Trigger: Group A beta-hemolytic Streptococcus (throat or skin infection); 1-3 weeks after pharyngitis, 3-6 weeks after impetigo
- Pathogenesis: Immune complex deposition; subepithelial "humps" on EM
- IF: Granular IgG + C3 in GBM and mesangium ("starry sky")
- Labs: Low C3 (complement consumed), ASO titer elevated, hematuria
- Prognosis: >95% of children recover; adults have a worse prognosis
- Treatment: Supportive; penicillin for active infection; antihypertensives, diuretics
2. Rapidly Progressive (Crescentic) GN (RPGN)
This is the most aggressive form, progressing to renal failure within weeks to months. The kidney biopsy hallmark is crescent formation in Bowman's space.
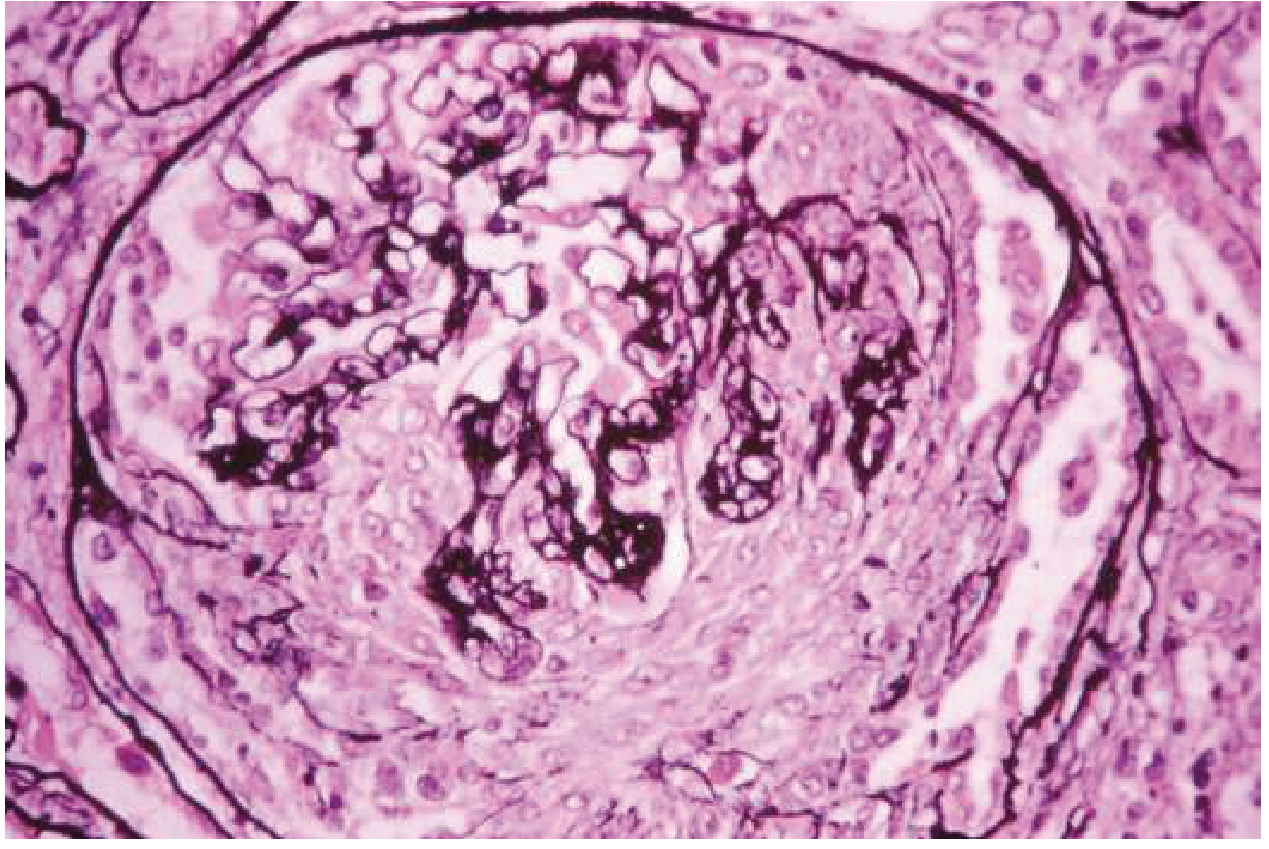
Crescentic GN: proliferating parietal epithelial cells compressing the glomerular tuft. - Goldman-Cecil Medicine, p. 1258
Three subtypes (from Goldman-Cecil Medicine, p. 1258):
| Type | Mechanism | IF Pattern | Example |
|---|---|---|---|
| Type I | Anti-GBM antibody | Linear IgG + C3 | Goodpasture disease |
| Type II | Immune complex | Granular IgG | Lupus, IgA vasculitis, post-infection |
| Type III | Pauci-immune (ANCA) | Little or no deposits | GPA, MPA, EGPA |
Treatment of ANCA-associated RPGN:
- Induction: Pulse methylprednisolone (10-15 mg/kg/day IV x 3 days) then prednisone 1 mg/kg/day + cyclophosphamide (IV 15 mg/kg q2-3 weeks or oral 1.5-2 mg/kg/day) OR rituximab (375 mg/m² weekly x 4 doses)
- Avacopan (C5a receptor inhibitor, 30 mg BD for 52 weeks) as adjunctive therapy in severe disease to reduce steroid exposure
- Plasmapheresis: Consider if creatinine >5.7 mg/dL, dialysis-dependent, or diffuse alveolar hemorrhage
- Maintenance: Azathioprine 1.5 mg/kg/day or rituximab 500 mg at months 6, 12, 18 for 18 months to 4 years
3. IgA Nephropathy (Berger Disease)
- Most common primary GN worldwide
- Pathogenesis: Mesangial deposition of poorly galactosylated IgA1 + IgG anti-IgA1 antibodies; complement activation
- Presentation: Recurrent macroscopic hematuria (often concurrent with upper respiratory infections - "synpharyngitic"), or persistent microscopic hematuria ± proteinuria
- IF: IgA dominant or co-dominant in mesangium
- EM: Mesangial electron-dense deposits
- Treatment: ACE inhibitors/ARBs for proteinuria; corticosteroids in selected patients; newer therapies include targeted-release budesonide (TRF-budesonide), sparsentan, and SGLT2 inhibitors
4. Membranoproliferative GN (MPGN)
- Presentation: Mixed nephritic/nephrotic picture
- LM: Mesangial proliferation, GBM thickening and "splitting" (tram-track appearance)
- Type I: Immune complex-mediated (HBV, HCV, SLE) - subendothelial deposits; IF: IgG + C3 + C1q + C4
- Dense Deposit Disease (Type II): Alternative complement pathway dysregulation; C3 only on IF; dense osmiophilic intramembranous deposits on EM
Summary Table: Primary Glomerulonephritides
| Disease | Presentation | Pathogenesis | LM | IF | EM |
|---|---|---|---|---|---|
| Post-infectious GN | Nephritic | Immune complex | Diffuse endocapillary infiltration | Granular IgG + C3 | Subepithelial humps |
| Crescentic (RPGN) | Nephritic + rapid progression | Anti-GBM / immune complex / ANCA | Crescents + necrosis | Linear / Granular / Negative | Varies |
| Membranous nephropathy | Nephrotic | In situ PLA2R antigen | Diffuse capillary wall thickening | Granular IgG + C3 diffuse | Subepithelial deposits |
| Minimal change disease | Nephrotic | Anti-nephrin antibodies | Normal; lipid in tubules | Negative (or fine IgG) | Foot process effacement only |
| FSGS | Nephrotic / proteinuria | Podocyte injury (various) | Focal segmental sclerosis + hyalinosis | IgM + C3 | Foot process effacement |
| MPGN type I | Nephritic/nephrotic | Immune complex | Mesangial proliferation + GBM splitting | IgG + C3 + C1q + C4 | Subendothelial deposits |
| Dense deposit disease | Hematuria | Complement dysregulation | Membranoproliferative | C3 only (no C1q/C4) | Dense deposits |
| IgA nephropathy | Recurrent hematuria | Unknown (IgA1 accumulation) | Focal mesangial proliferation | IgA dominant in mesangium | Mesangial deposits |
Summary adapted from Robbins, Cotran & Kumar Pathologic Basis of Disease, Table 20.5, p. 840
Secondary GN (Associated With Systemic Diseases)
| Systemic Disease | Renal Pattern |
|---|---|
| Systemic lupus erythematosus | Lupus nephritis (WHO Class I-VI); subendothelial + mesangial deposits; "wire loop" |
| IgA vasculitis (Henoch-Schönlein) | IgA mesangial deposits; similar to IgA nephropathy |
| Goodpasture syndrome | Anti-GBM antibody; linear IF; pulmonary-renal syndrome |
| ANCA vasculitis (GPA, MPA) | Pauci-immune crescentic GN |
| Hepatitis B/C | MPGN (HBV/HCV), membranous (HBV), cryoglobulinemic GN (HCV) |
| Diabetic nephropathy | Diffuse/nodular glomerulosclerosis (Kimmelstiel-Wilson nodules) |
| HIV | Collapsing FSGS (HIVAN) |
Complement Levels as a Diagnostic Clue
| Low C3, Low C4 | Low C3, Normal C4 | Normal Complement |
|---|---|---|
| SLE | Post-infectious GN | IgA nephropathy |
| Cryoglobulinemic GN | MPGN (alternative pathway) | ANCA-GN |
| Dense deposit disease | Anti-GBM disease | |
| FSGS, membranous |
General Management Principles
- Treat the underlying cause where possible (antibiotics for infection, antivirals for HBV/HCV)
- Supportive measures: Salt/water restriction, antihypertensives (ACE-I/ARBs preferred for their antiproteinuric effect), loop diuretics
- Immunosuppression: Indicated for immune-mediated GN - options include corticosteroids, cyclophosphamide, rituximab, mycophenolate mofetil, azathioprine, calcineurin inhibitors (for nephrotic types like membranous/FSGS)
- Monitoring: Serial creatinine, urinalysis, proteinuria quantification, ANCA/anti-GBM titers where relevant
- Renal biopsy: Essential for definitive diagnosis and guiding treatment in most cases of GN
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease, Ch. 20, pp. 815-842
- Goldman-Cecil Medicine, Ch. 107, pp. 1255-1260
- Comprehensive Clinical Nephrology, 7th Edition
- Brenner and Rector's The Kidney, 2-Volume Set
Recent evidence note: A 2025 meta-analysis (PMID: 40721561) confirms the efficacy and safety of targeted-release budesonide (TRF-budesonide) for IgA nephropathy. A 2024 systematic review (PMID: 39423662) highlights the evolving role of innate immunity and the gut-kidney axis in IgA nephropathy pathogenesis.
Nephrotic syndrome full long answer under all heading definition classification pathogenesis clinical features investigation management also give flow charts and algorithm master road map of this
Finding Sources
Searching PubMed
"nephrotic syndrome"[MeSH Terms] AND "treatment"[MeSH Terms]
Reading File
Reading File
Searching PubMed
"nephrotic syndrome" AND management
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
This is a complete, exam-level long-answer guide. Here is a summary of everything covered:
What Was Covered
1. Definition
The classic tetrad: proteinuria >3.5 g/day, hypoalbuminemia <3.5 g/dL, edema, and hyperlipidemia - with the precise diagnostic thresholds for adults and children.
2. Classification
- Etiological: Primary vs. Secondary (with full secondary cause table)
- Histopathological: MCD, FSGS, Membranous Nephropathy, MPGN, IgA - with age frequency breakdown
- Steroid Response: SSNS, SRNS, FRNS, SDNS (clinical classification)
3. Pathogenesis (7 mechanisms)
All the downstream consequences of podocyte injury - proteinuria, hypoalbuminemia, underfill vs. overfill edema, hyperlipidemia/lipiduria, hypercoagulability, susceptibility to infection, and loss of binding proteins (vitamin D, transferrin, thyroid hormone)
4. Individual Diseases
MCD, FSGS (with Columbia variants), and Membranous Nephropathy - with LM/IF/EM findings and histology images
5. Clinical Features
Full symptom/sign table, Muehrcke's lines, xanthelasma, and a complete complications tree
6. Investigations
Tiered (confirm diagnosis → etiology → complications → biopsy), with clinical significance of each test
7. Management
- General: diet, edema (underfill vs. overfill algorithm), anti-proteinuric strategy, lipid control, anticoagulation, infection prevention
- Disease-specific: MCD protocol, FSGS protocol, Membranous Nephropathy risk-based algorithm (with image)
- Special populations
8. Flowcharts & Algorithms
- Pathogenesis flow
- Edema management algorithm
- MCD treatment algorithm with relapse pathways
- Membranous Nephropathy risk-stratified algorithm (textbook image)
- Master Roadmap flowchart from presentation to final management
You as a genius student write a laq on this topic what all points professor wants write systematically and refer standard books of medicine and paediatric
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
I now have all the material I need from 6+ standard textbooks. Let me compose the LAQ exactly as a top student would write it in an exam.
NEPHROTIC SYNDROME
Long Answer Question (LAQ) - Examination Standard
INTRODUCTION
Nephrotic syndrome (NS) is one of the most clinically important glomerular syndromes in both internal medicine and paediatrics. It is not a diagnosis in itself but a clinical constellation arising from a derangement of the glomerular filtration barrier, resulting in massive urinary protein loss. Understanding it requires integrating renal physiology, pathology, clinical medicine, and pharmacology - which is why it is a favourite topic in university examinations.
1. DEFINITION
Nephrotic syndrome is defined as the clinical tetrad of:
| Component | Adult Threshold | Paediatric Threshold |
|---|---|---|
| Massive proteinuria | > 3.5 g/24 hours | > 40 mg/m²/hr or urine protein:creatinine ratio > 2.0 mg/mg |
| Hypoalbuminemia | Serum albumin < 3.0-3.5 g/dL | Serum albumin < 2.5 g/dL |
| Generalised edema | Periorbital, facial, dependent | Periorbital especially in children |
| Hyperlipidemia + Lipiduria | ↑ cholesterol, ↑ TG, ↑ LDL | Oval fat bodies in urine |
"Nephrotic syndrome is defined as more than 3.5 g of proteinuria in 24 hours, with serum albumin level less than 3.5 g/dL accompanied by hyperlipidemia and clinically apparent edema." — NKF Primer on Kidney Diseases, 8th Edition, p. 189
"The manifestations of the syndrome include massive proteinuria with the daily loss of 3.5 g or more, hypoalbuminemia with plasma albumin levels less than 3 g/dL, generalized edema, and hyperlipidemia and lipiduria." — Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 843
2. INCIDENCE AND EPIDEMIOLOGY
- Annual incidence in children: 2-7 per 100,000; prevalence 16 per 100,000
- Male:Female ratio in children = 2:1 (this equalises in adults)
- Peak age in children: 2-6 years (preschool age); median age of onset 2.5 years
- In children under 10 years, Minimal Change Disease (MCD) accounts for 70-90% of cases
- In adults, Focal Segmental Glomerulosclerosis (FSGS) and Membranous Nephropathy (MN) are most common
- Diabetic nephropathy is the most common cause of NS globally (secondary cause)
- (Brenner & Rector's The Kidney; Campbell Walsh Wein Urology, 3-Volume Set)
3. AETIOLOGY AND CLASSIFICATION
A. PRIMARY (Idiopathic) Nephrotic Syndrome
Disease confined to the kidney with no identifiable systemic cause
| Histological Type | Adults (%) | Children (%) | Key Feature |
|---|---|---|---|
| Minimal Change Disease (MCD) | 15-25% | 70-90% | Foot process effacement only on EM |
| Focal Segmental Glomerulosclerosis (FSGS) | 25-35% | 10-15% | Focal segmental sclerosis + hyalinosis |
| Membranous Nephropathy (MN) | 25-30% | Rare | Subepithelial deposits; spikes on silver stain |
| Membranoproliferative GN (MPGN) | 5-10% | 5% | GBM splitting; "tram-track" |
| IgA Nephropathy | 5-10% | Variable | Mesangial IgA deposits |
B. SECONDARY Nephrotic Syndrome
NS as a manifestation of a systemic disease or identifiable cause
| Category | Specific Causes |
|---|---|
| Metabolic | Diabetes mellitus (most common secondary), amyloidosis |
| Autoimmune/Connective tissue | SLE (lupus nephritis Class V), mixed connective tissue disease |
| Infections | Hepatitis B → MN; Hepatitis C → MPGN; HIV → Collapsing FSGS; Malaria; Syphilis; Filariasis |
| Drugs/Toxins | NSAIDs, gold, penicillamine, heroin, captopril, pamidronate, mercury |
| Malignancy | Hodgkin lymphoma → MCD; Solid tumours (lung, colon) → MN |
| Hereditary/Genetic | Congenital NS (Finnish type: NPHS1/nephrin mutation); Alport syndrome; Denys-Drash syndrome (WT1 mutation) |
| Others | Pre-eclampsia, renal vein thrombosis, bee sting allergy |
(Brenner & Rector's The Kidney, Box 31.1, p. 1339; Robbins, Cotran & Kumar)
C. CLINICAL CLASSIFICATION (Used in Paediatrics)
| Type | Definition |
|---|---|
| Steroid-Sensitive NS (SSNS) | Complete remission of proteinuria within 8 weeks of steroid therapy |
| Steroid-Resistant NS (SRNS) | No remission after 8 weeks of full-dose prednisolone |
| Frequently-Relapsing NS (FRNS) | ≥ 2 relapses in 6 months OR ≥ 4 relapses in any 12-month period |
| Steroid-Dependent NS (SDNS) | Two consecutive relapses during steroid taper OR need for continuous steroids to maintain remission |
(Campbell Walsh Wein Urology, 3-Volume Set, p. 460-461)
4. PATHOGENESIS
The unifying mechanism is disruption of the glomerular filtration barrier - specifically the podocyte slit diaphragm - leading to loss of both the size and charge selectivity of the glomerulus.
Step-by-Step Pathogenic Cascade
PRIMARY INSULT
(immune, toxic, genetic, metabolic)
↓
PODOCYTE INJURY
(foot process effacement, slit diaphragm disruption,
nephrin/podocin dysfunction, anti-nephrin antibodies)
↓
LOSS OF GLOMERULAR FILTRATION BARRIER
↓
MASSIVE PROTEINURIA (>3.5 g/day)
↙ ↘ ↘ ↘
HYPO- EDEMA HYPER- HYPER-
ALBUMIN- LIPIDEMIA COAG-
EMIA ULABILITY
A. Mechanism of Proteinuria
- The normal GBM acts as both a size barrier (filters proteins > 68 kDa) and a charge barrier (negatively charged proteoglycans repel anionic albumin)
- In NS, podocyte foot process effacement disrupts the filtration slit - proteins cross freely
- Selective proteinuria: mainly albumin (low MW) = MCD; indicative of good steroid response
- Non-selective proteinuria: albumin + globulins = FSGS, MN; indicates worse prognosis
B. Mechanism of Hypoalbuminemia
- Urinary albumin losses exceed hepatic synthetic capacity
- Increased renal catabolism of filtered albumin
- Reduced nutritional intake (anorexia from bowel edema)
C. Mechanism of Oedema
Two distinct mechanisms operate:
| "Underfill" (Classical) | "Overfill" (Intrinsic) | |
|---|---|---|
| Primary event | ↓ plasma oncotic pressure → fluid shift to interstitium | Primary renal Na/H₂O retention |
| Plasma volume | Contracted | Expanded |
| RAAS | Activated (↑ renin, ↑ aldosterone) | Suppressed |
| Sympathetic NS | Activated | Suppressed |
| ANP | Decreased | Increased |
| Typical disease | MCD | FSGS, membranous, diabetic |
| Response to diuretics | Risk of hypovolemia/AKI | Generally safe |
Additional factors: secondary hyperaldosteronism, sympathetic activation, reduced ANP secretion, enhanced ENaC activity in the collecting duct.
(Brenner & Rector's The Kidney, p. 2277)
D. Mechanism of Hyperlipidemia and Lipiduria
- ↓ oncotic pressure → stimulates hepatic lipoprotein synthesis (VLDL, LDL ↑)
- ↓ lipoprotein lipase activity → impaired peripheral lipid clearance
- ↓ HDL (small molecule, easily filtered)
- Lipiduria: lipoproteins leak into urine → absorbed by tubular cells → shed as oval fat bodies ("Maltese cross" birefringence on polarised light microscopy)
- Long-term hyperlipidemia accelerates cardiovascular disease
E. Mechanism of Hypercoagulability
Urinary losses of natural anticoagulants drive a prothrombotic state:
| Lost in Urine | Gained / Increased |
|---|---|
| Antithrombin III | ↑ Fibrinogen |
| Protein C, Protein S | ↑ Factors II, V, VII, VIII, X, XIII |
| Plasminogen | ↑ Platelet aggregation |
| Factor IX, XI | ↑ Blood viscosity (hemoconcentration) |
Risk of renal vein thrombosis, DVT, and pulmonary embolism - highest in membranous nephropathy. Risk is greatest when albumin < 2.0 g/dL and proteinuria > 10 g/day. (Brenner & Rector's The Kidney, Box 31.3; NKF Primer, 8th Ed., p. 190)
F. Susceptibility to Infection
- Loss of IgG → hypogammaglobulinemia
- Loss of complement factor B and properdin → impaired opsonization
- Loss of properdin → reduced alternative complement pathway activity
- T-cell dysfunction (particularly in MCD)
- Common organisms: Streptococcus pneumoniae (spontaneous bacterial peritonitis), Staphylococcus aureus, gram-negative organisms
G. Other Protein Losses and Their Consequences
| Protein Lost | Clinical Consequence |
|---|---|
| Transferrin | Iron-deficiency anaemia (microcytic) |
| Vitamin D-binding protein | Vitamin D deficiency → ↓ Ca²⁺ → Secondary hyperparathyroidism |
| Thyroxine-binding globulin (TBG) | Low total T4 (free T4 and TSH normal - euthyroid) |
| Ceruloplasmin | Copper and zinc deficiency |
| IgG | Hypogammaglobulinemia, recurrent infections |
| Erythropoietin | Anaemia (additional to transferrin loss) |
(Brenner & Rector's The Kidney, Box 31.2, p. 1402)
5. PATHOLOGY OF INDIVIDUAL DISEASES
A. Minimal Change Disease (MCD)
Pathogenesis: Abnormal T-cell regulation → elaboration of a circulating podocyte permeability factor (possibly hemopexin isoform) → disruption of podocyte slit diaphragm → foot process effacement. Association with Hodgkin's lymphoma supports T-cell mediation.
(Brenner & Rector's The Kidney, p. 1342)
| Microscopy | Finding |
|---|---|
| Light microscopy | Normal glomeruli; lipid droplets in tubular cells ("lipoid nephrosis") |
| Immunofluorescence | Negative (or subtle fine IgG/IgM) |
| Electron microscopy | Diffuse foot process effacement (100%); microvillous transformation; NO deposits |
- MCD is a diagnosis of exclusion - all other causes must be ruled out
- The effacement diminishes as proteinuria resolves with treatment
B. Focal Segmental Glomerulosclerosis (FSGS)
| Microscopy | Finding |
|---|---|
| LM | Focal (some glomeruli affected) + segmental (only part of tuft) sclerosis and hyalinosis |
| IF | IgM + C3 in sclerotic areas (non-specific trapping) |
| EM | Foot process effacement + epithelial cell denudation + subendothelial hyaline deposits |
Columbia Classification Variants:
- NOS (Not Otherwise Specified) - most common
- Perihilar variant - adaptive/secondary
- Cellular variant - active lesion
- Tip variant - better prognosis, steroid-responsive
- Collapsing variant - worst prognosis; HIV-associated (HIVAN), COVID-19-associated
C. Membranous Nephropathy (MN)
| Microscopy | Finding |
|---|---|
| LM | Diffuse capillary wall thickening; Jones silver stain: "spikes" projecting from GBM between subepithelial deposits |
| IF | Granular IgG + C3 along peripheral capillary wall ("beads on a string") |
| EM | Subepithelial deposits between GBM and podocyte; staged I-IV by Ehrenreich and Churg |
- Anti-PLA2R antibodies positive in 70-80% of primary MN - diagnostic and prognostic
- Rule of thirds: 1/3 spontaneous remission, 1/3 persistent proteinuria, 1/3 progress to ESKD
6. CLINICAL FEATURES
Symptoms
| Symptom | Mechanism |
|---|---|
| Facial/periorbital puffiness (first noticed on waking) | Low oncotic pressure; loose connective tissue of periorbital region |
| Frothy urine (persistent foam) | Proteinuria |
| Decreased urine output / oliguria | Reduced effective circulating volume (underfill) |
| Progressive weight gain | Fluid retention |
| Abdominal distension | Ascites; bowel wall edema → anorexia, nausea, diarrhoea |
| Breathlessness | Pleural effusion; ascites limiting diaphragm excursion |
| Fatigue, weakness | Hypoalbuminemia, anaemia, muscle wasting |
Signs
| Sign | Details |
|---|---|
| Periorbital edema | Puffy eyelids, worst in mornings; often the first sign in children |
| Pitting edema | Dependent - ankles, legs; sacrum in bedridden patients |
| Ascites | Shifting dullness, fluid thrill in severe cases |
| Pleural effusion | Dullness at lung bases, reduced breath sounds bilaterally |
| Genital edema | Scrotal/labial edema in severe NS |
| Pallor | Iron-deficiency anaemia (transferrin loss) |
| Muehrcke's lines | Paired white transverse bands on nails - hypoalbuminemia |
| Xanthelasma / xanthoma | Chronic hyperlipidemia |
| Blood pressure | Low/normal in MCD (underfill); elevated in FSGS, diabetic NS (overfill) |
| No haematuria (usually) | Absence of haematuria distinguishes NS from nephritic syndrome |
Paediatric-Specific Features
- Periorbital oedema may be the only presenting sign initially
- Often mistaken for allergic periorbital oedema (diagnosis is delayed)
- Symptoms often follow an upper respiratory infection (URTI) trigger
- Abdominal pain may indicate spontaneous bacterial peritonitis (SBP)
7. COMPLICATIONS
Mnemonic: "IT-CAKE" (I-nfection, T-hrombosis, C-ardiovascular, A-KI, K-idney progression, E-ndocrine)
| Complication | Mechanism | Clinical Presentation |
|---|---|---|
| Infection | ↓ IgG, ↓ complement, T-cell suppression | SBP (Strep. pneumoniae), cellulitis, sepsis, peritonitis |
| Thromboembolism | ↓ AT-III, protein C/S, ↑ fibrinogen, platelet activation | Renal vein thrombosis (flank pain, haematuria, ↑ creatinine), DVT, PE |
| Cardiovascular disease | Prolonged hyperlipidemia, hypertension | Accelerated atherosclerosis, MI |
| Acute Kidney Injury (AKI) | Hypovolemia (underfill), bilateral renal vein thrombosis | Oliguria, rising creatinine |
| Chronic Kidney Disease | Progressive glomerulosclerosis (especially FSGS, MN) | ESKD requiring dialysis/transplant |
| Endocrine/Metabolic | Protein losses | Vitamin D deficiency, iron deficiency anaemia, hypothyroidism (low total T4), growth retardation (children) |
| Iatrogenic | Steroid/immunosuppressant side effects | Cushingoid features, osteoporosis, cataract, glucose intolerance, opportunistic infections |
8. INVESTIGATIONS
TIER 1 - CONFIRM DIAGNOSIS
| Test | Expected Finding | Significance |
|---|---|---|
| 24-hour urine protein | > 3.5 g/24 hr | Gold standard for diagnosis |
| Spot urine protein:creatinine (UPCR) | > 3.0-3.5 mg/mg | Equivalent to 24-hr collection; used in children |
| Urinalysis (dipstick + microscopy) | 3-4+ protein; oval fat bodies; fatty casts; "Maltese cross" on polarised light | Lipiduria is pathognomonic |
| Serum albumin | < 3.0-3.5 g/dL | Hypoalbuminemia |
| Serum cholesterol, LDL, TG | ↑ Total cholesterol, ↑ LDL, ↑ TG, ↓ HDL | Hyperlipidemia |
| Serum creatinine / eGFR | Normal (MCD) or reduced (FSGS, diabetic) | Baseline renal function |
| Serum electrolytes | Hyponatremia (dilutional) | Guides fluid management |
TIER 2 - ESTABLISH AETIOLOGY (SEROLOGICAL WORKUP)
| Test | Positive Finding | Suggests |
|---|---|---|
| Serum C3, C4, CH50 | ↓ C3, ↓ C4 | SLE; ↓ C3 alone → MPGN, dense deposit disease |
| ANA, anti-dsDNA | Positive | Lupus nephritis |
| Anti-PLA2R antibody | Positive (70-80%) | Primary membranous nephropathy (diagnostic) |
| HBsAg, HBV viral load | Positive | HBV-associated MN |
| Anti-HCV, HCV RNA | Positive | MPGN, cryoglobulinemic GN |
| HIV antibody | Positive | Collapsing FSGS (HIVAN) |
| Blood glucose, HbA1c | Elevated | Diabetic nephropathy |
| SPEP/UPEP (electrophoresis) | M-spike | Multiple myeloma, AL amyloidosis |
| Serum free light chains | Elevated κ or λ | Myeloma, light chain disease |
| ASO titre, anti-DNase B | Elevated | Post-streptococcal (if mixed nephritic/nephrotic) |
| Fasting lipid profile | ↑ TC, ↑ LDL | Cardiovascular risk stratification |
TIER 3 - ASSESS COMPLICATIONS
| Test | Finding | Assesses |
|---|---|---|
| Renal ultrasound (+ Doppler) | Enlarged kidneys (HIVAN); renal vein clot | Structural disease, renal vein thrombosis |
| Serum calcium, 25-OH Vitamin D | ↓ | Vitamin D deficiency |
| Serum iron, TIBC, ferritin | Iron deficiency pattern | Transferrin loss → anaemia |
| Thyroid function (TSH, free T4) | Low total T4, TBG; TSH normal | TBG loss → spuriously low T4 |
| Coagulation profile (PT, APTT, fibrinogen, AT-III) | ↑ fibrinogen, ↓ AT-III | Hypercoagulable state |
| Chest X-ray | Pleural effusions, cardiomegaly | Volume overload |
| ECG | ST changes | Cardiac complications |
TIER 4 - RENAL BIOPSY
Indications for renal biopsy:
In Adults: Nearly always indicated to define the exact pathological diagnosis before beginning immunosuppressive treatment.
In Children - Biopsy is NOT initially required if the following typical features of MCNS (MCD) are present:
- Age 1-8 years
- Pure nephrotic syndrome (no haematuria, no hypertension, normal GFR, normal complement)
- No systemic features
Biopsy IS required in children when:
- Age < 1 year (suspect congenital NS - genetic)
- Age > 8-10 years (MCD less likely; MN, FSGS more likely)
- Macroscopic haematuria
- Persistent hypertension
- Hypocomplementemia (low C3/C4)
- Steroid resistance (SRNS)
- Systemic features (rash, arthritis, etc.)
Three modalities of biopsy interpretation:
- Light microscopy (H&E, PAS, Jones silver, Masson trichrome)
- Immunofluorescence (IgG, IgA, IgM, C1q, C3, C4)
- Electron microscopy (deposit location, foot process effacement extent)
9. DIFFERENTIAL DIAGNOSIS
| Condition | Differentiating Features |
|---|---|
| Nephritic syndrome | Haematuria + RBC casts + hypertension + oliguria predominate; proteinuria subnephrotic |
| Congestive heart failure | Raised JVP, cardiomegaly, bilateral crackles; serum albumin normal |
| Liver cirrhosis | Spider naevi, caput medusae, splenomegaly; signs of portal hypertension; ↑ PT; urine protein absent |
| Protein-losing enteropathy | GI symptoms; low albumin + LOW serum cholesterol (hepatic synthesis depressed too) |
| Allergic periorbital oedema | No proteinuria; responds to antihistamines; no dependent oedema |
| Pre-eclampsia | Pregnancy; hypertension + proteinuria + maternal complications |
10. MANAGEMENT
OVERALL FRAMEWORK
┌─────────────────────────────────────────────┐
│ NEPHROTIC SYNDROME │
│ │
│ STEP 1: Confirm diagnosis │
│ STEP 2: Assess & treat complications │
│ STEP 3: General/supportive care (ALL) │
│ STEP 4: Determine aetiology (biopsy/serology│
│ STEP 5: Disease-specific immunosuppression │
│ STEP 6: Monitor & manage relapse │
└─────────────────────────────────────────────┘
A. GENERAL (NON-SPECIFIC) MANAGEMENT
Applicable to ALL patients regardless of aetiology.
1. Diet
- Sodium restriction: < 2 g NaCl/day (reduces oedema and enhances diuretics)
- Protein: 0.8-1.0 g/kg/day (excessive protein worsens proteinuria; restriction aids anti-proteinuric measures)
- Fluid restriction: Only if hyponatremia (serum Na < 130 mEq/L) is present
- Low saturated fat, complex carbohydrate: Addresses hyperlipidemia
2. Oedema Management
OEDEMA MANAGEMENT
↓
Assess volume status:
MCD → likely UNDERFILL
FSGS/MN/Diabetic → likely OVERFILL
↓
ORAL LOOP DIURETIC (Furosemide 40-80 mg/day)
↓
INADEQUATE RESPONSE?
Add thiazide (metolazone 2.5-5 mg) → sequential nephron blockade
↓
STILL RESISTANT?
IV furosemide ± spironolactone (secondary hyperaldosteronism)
Note: IV albumin + furosemide is controversial and NOT routinely recommended
↓
CAUTION: In underfill patients (MCD) → aggressive diuresis risks AKI/hypovolemia
"Hypoalbuminemia reduces the binding of furosemide to plasma proteins and thereby enlarges its volume of distribution. A more logical approach to diuretic resistance is to limit albuminuria with an ACE inhibitor, ARB, or both." - Brenner & Rector's The Kidney, p. 2277
3. Anti-Proteinuric Strategy (RAAS Blockade)
- ACE inhibitors (enalapril, ramipril) OR ARBs (losartan, irbesartan) - first-line
- Reduce intraglomerular pressure → reduce proteinuria by 30-50%
- Slow CKD progression independently of BP effect
- Target urine protein < 1 g/day; ideally < 0.5 g/day
- Monitor: serum creatinine (acceptable rise ≤ 30% from baseline), serum K+ (hyperkalemia)
- Emerging: SGLT2 inhibitors (empagliflozin, dapagliflozin) - additive anti-proteinuric and renoprotective effects
4. Hyperlipidemia
- Statins: atorvastatin 10-40 mg or rosuvastatin 10-20 mg/night (first-line)
- Target LDL < 100 mg/dL; reduces cardiovascular risk
- Fibrates for severe hypertriglyceridemia (caution if using with statins - myopathy)
- Lipid-lowering alone does NOT treat underlying proteinuria
5. Anticoagulation
THROMBOSIS RISK IN NS
↓
HIGH RISK → Prophylactic anticoagulation
(Membranous nephropathy + albumin < 2.0-2.5 g/dL + proteinuria > 10 g/day)
↓
WARFARIN: Target INR 2.0-3.0 OR LMWH (enoxaparin)
Note: DOACs (rivaroxaban, apixaban) - altered protein binding in NS - use cautiously
↓
ESTABLISHED THROMBOSIS: Full anticoagulation × 6-12 months
6. Infection Prevention
- Pneumococcal vaccination (PCV13 + PPSV23) before starting immunosuppression
- Children: Oral penicillin V 125 mg BD prophylaxis during active disease (SBP prevention)
- Co-trimoxazole prophylaxis during high-dose steroids/cyclophosphamide (PCP pneumonia)
- Low threshold for antibiotics in any febrile NS patient
- Varicella vaccination if non-immune before immunosuppression
- Avoid live vaccines during immunosuppression
B. DISEASE-SPECIFIC MANAGEMENT
MCD / Steroid-Sensitive NS - Treatment Protocol
(Campbell Walsh Wein Urology, 3-Volume Set, p. 460; NKF Primer, 8th Ed.)
FIRST EPISODE OF NS IN CHILD (typical features = empirical treatment)
↓
PREDNISOLONE: 60 mg/m²/day (max 60 mg/day) OR 2 mg/kg/day (max 60 mg)
× 4-6 weeks daily
↓
Then: alternate-day prednisolone × 4-6 weeks, then taper and stop
↓
8 WEEKS
↙ ↘
REMISSION NO REMISSION
(protein clears) (SRNS)
↓ ↓
Taper & stop RENAL BIOPSY
+ re-evaluate
Consider CNI,
rituximab
↓
RELAPSE? (proteinuria returns)
↓
INFREQUENT RELAPSE FREQUENT RELAPSE / SDNS
(<2 in 6 months) (≥2 relapses in 6 months)
↓ ↓
Repeat prednisolone STEROID-SPARING AGENTS:
course 1. Cyclophosphamide 2 mg/kg/day × 8-12 wks
2. Mycophenolate mofetil (MMF) 800-1200 mg/m²/day
3. Calcineurin inhibitor (CNI):
Cyclosporine 4-5 mg/kg/day OR
Tacrolimus 0.1-0.15 mg/kg/day
4. Rituximab 375 mg/m² IV × 1-4 doses
5. Levamisole (in some guidelines)
"Corticosteroids will induce a remission in the vast majority of children with nephrotic syndrome... Almost 50% of children with SSNS will experience multiple relapses." — Campbell Walsh Wein Urology, 3-Volume Set, p. 460
FSGS - Treatment Protocol
| FSGS Subtype | Treatment |
|---|---|
| Primary FSGS (idiopathic) | Prednisolone 1 mg/kg/day (max 80 mg) × 4-6 months; if SRNS: CNI (cyclosporine 3-5 mg/kg/day) ± low-dose steroids; rituximab for SDNS |
| Secondary FSGS | Treat underlying cause (HIV → ART; obesity → weight loss; nephrotoxic drug → stop); ACE-I/ARB; NO immunosuppression |
| Genetic FSGS | Supportive (ACE-I/ARB); steroids ineffective; genetic counselling; transplant |
| Collapsing FSGS (HIV) | Antiretroviral therapy (ART) is primary treatment; ACE-I/ARB |
Membranous Nephropathy - Risk-Stratified Treatment
(Comprehensive Clinical Nephrology, 7th Ed., p. 303)
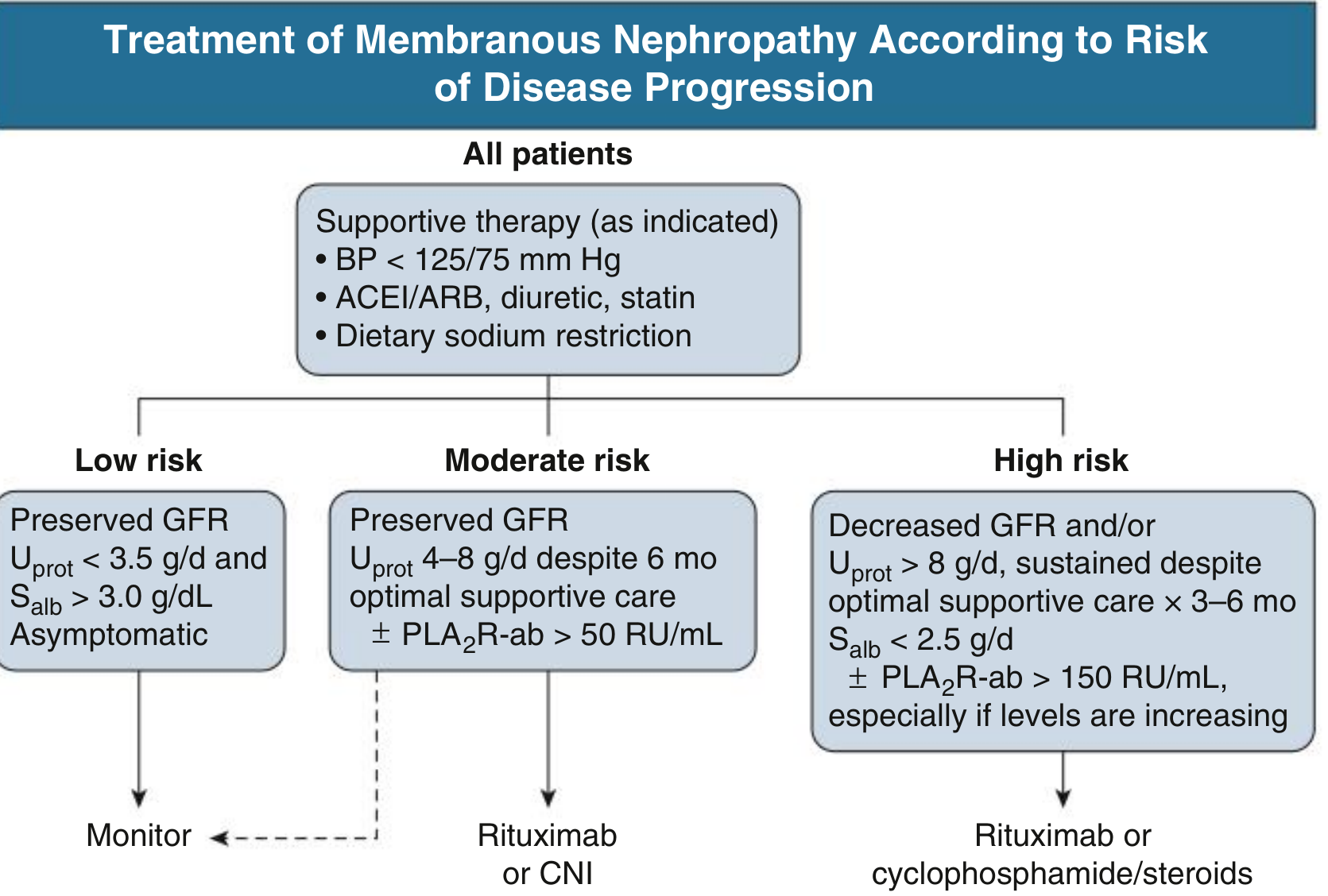
- Low risk: Preserved GFR, protein < 3.5 g/day, albumin > 3.0 g/dL → Monitor; 30% spontaneous remission
- Moderate risk: Protein 4-8 g/day, preserved GFR, anti-PLA2R > 50 RU/mL → Rituximab (preferred) or calcineurin inhibitor
- High risk: Protein > 8 g/day OR declining GFR OR albumin < 2.5 g/dL OR anti-PLA2R > 150 RU/mL → Rituximab OR Ponticelli regimen (alternating methylprednisolone + chlorambucil/cyclophosphamide monthly × 6 months)
Ponticelli Regimen (Months 1, 3, 5: IV methylprednisolone 1g × 3 days then oral prednisolone 0.5 mg/kg/day × 27 days; Months 2, 4, 6: chlorambucil 0.2 mg/kg/day)
Congenital Nephrotic Syndrome (CNS)
- Immunosuppression is NOT effective (genetic basis)
- Conservative: Na/fluid restriction, IV albumin + loop diuretics
- Hypercaloric diet, thyroid hormone replacement (TBG loss)
- Prophylaxis for thrombosis and infection
- Ultimately: bilateral nephrectomy + dialysis + renal transplantation (Campbell Walsh Wein Urology, 3-Volume Set, p. 462)
11. MONITORING RESPONSE TO TREATMENT
| Parameter | Frequency | Target |
|---|---|---|
| Urine protein:creatinine ratio | Weekly (active) → monthly (remission) | < 0.3 mg/mg |
| Serum albumin | Monthly | > 3.5 g/dL |
| Serum creatinine/eGFR | Monthly | Stable/improving |
| Blood pressure | Every visit | < 125/75 mmHg |
| Fasting lipid profile | Every 3-6 months | LDL < 100 mg/dL |
| Growth parameters | Each visit (children) | Normal height/weight velocity |
| Steroid complications | Each visit | Glucose, BP, bone density, eyes |
| Anti-PLA2R titer (MN) | 3-6 monthly | Declining = treatment response |
Outcome Definitions:
- Complete remission: Urine protein < 0.3 g/day × 3 months
- Partial remission: ≥ 50% reduction AND protein < 3.5 g/day
- Relapse: Return of proteinuria > 3.5 g/day (or > 2+ on dipstick × 3 days) after remission
- Steroid resistance: No remission after 16 weeks full-dose steroids (adult) / 8 weeks (child)
12. PROGNOSIS
| Disease | Prognosis |
|---|---|
| MCD in children | Excellent; > 90% remission with steroids; relapses common (50%); CKD extremely rare |
| MCD in adults | Good; 75-85% remission; slower recovery; occasional steroid resistance |
| Primary FSGS | Guarded; 50% ESKD within 10 years without treatment; better if tip variant |
| Membranous Nephropathy | Rule of thirds (remit / persist / ESKD); 25% ESKD at 8 years |
| Diabetic NS | Progressive CKD; RAAS blockade + SGLT2i slow progression |
| Congenital NS (Finnish type) | Poor without bilateral nephrectomy + transplant; transplant outcomes good |
| Lupus nephritis (Class V MN) | Variable; close follow-up needed; risk of transformation |
| Amyloidosis | Poor; ESKD within 2-5 years |
SUMMARY TABLE: NEPHROTIC SYNDROME AT A GLANCE
| Feature | MCD | FSGS | Membranous | MPGN |
|---|---|---|---|---|
| Age group | Children (peak 2-6 yrs) | Young adults | Adults >50 yrs | Young adults |
| % of adult NS | 15% | 25-35% | 25-30% | 5-10% |
| LM | Normal | Focal segmental sclerosis | GBM thickening; spikes | Mesangial proliferation; GBM splitting |
| IF | Negative | IgM + C3 (segmental) | Granular IgG + C3 | IgG + C3 + C1q + C4 |
| EM | Foot process effacement ONLY | Foot process effacement + denudation | Subepithelial deposits | Subendothelial deposits |
| Complement | Normal | Normal | Normal | ↓ C3, ↓ C4 |
| Haematuria | Absent | May be present | May be present | Present |
| Steroid response | Excellent (>90%) | Poor (40-60% SRNS) | Variable | Variable |
| Thrombosis risk | Low | Moderate | HIGH | Moderate |
| Prognosis | Excellent | 50% ESKD in 10 yrs | Rule of thirds | Variable |
| Key antibody | Anti-nephrin (newer) | — | Anti-PLA2R (70-80%) | — |
STANDARD TEXTBOOK REFERENCES
| Reference | Chapter/Page | Content |
|---|---|---|
| Robbins, Cotran & Kumar - Pathologic Basis of Disease (10th Ed.) | Ch. 20, pp. 827-845 | Pathology, pathogenesis, morphology of each type |
| Brenner & Rector's The Kidney (2-Volume Set) | Ch. 31, pp. 1339-1360; Ch. 50 | Detailed pathogenesis, protein alterations, diuretics |
| Goldman-Cecil Medicine (26th Ed.) | Ch. 107, pp. 1255-1260 | Clinical diagnosis and management |
| Harrison's Principles of Internal Medicine (22nd Ed., 2025) | Ch. on Glomerular Diseases | Systemic approach, latest evidence |
| NKF Primer on Kidney Diseases (8th Ed.) | Ch. 16-18, pp. 189-220 | Modern management, FSGS classification, MN algorithm |
| Comprehensive Clinical Nephrology (7th Ed.) | Ch. 20-21 | MN risk stratification; rituximab; KDIGO guidelines |
| Campbell Walsh Wein Urology (3-Volume Set) | Ch. 21, pp. 459-466 | Paediatric nephrotic syndrome; SSNS/SRNS/FRNS/SDNS |
| Nelson Textbook of Pediatrics (21st Ed.) | Ch. 545 | Paediatric NS; ISKDC criteria; steroid protocols |
| Forfar and Arneil's Textbook of Pediatrics | Renal chapter | Congenital NS; paediatric management |
EXAMINER'S CHECKLIST - WHAT PROFESSORS LOOK FOR
A first-class answer to "Nephrotic Syndrome LAQ" must cover:
✅ Clear definition with all four components and thresholds (adults vs children)
✅ Complete aetiology - primary vs secondary, with examples in each category
✅ Classification - histological (4 types) AND clinical (SSNS/SRNS/FRNS/SDNS)
✅ Pathogenesis cascade - proteinuria → hypoalbuminemia → oedema (underfill/overfill) → hyperlipidemia → hypercoagulability → infection susceptibility
✅ Clinical features - Muehrcke's lines, frothy urine, periorbital oedema, features distinguishing NS from nephritic
✅ Complications - especially thrombosis (renal vein), SBP, AKI
✅ Investigations in tiers - routine, serological (anti-PLA2R), renal biopsy with indications
✅ Biopsy - indications in children vs adults; three modalities (LM, IF, EM)
✅ Management - general (diet, diuretics, RAAS, statins, anticoagulation, vaccines) AND disease-specific (steroid protocol for MCD, FSGS, membranous risk algorithm)
✅ Paediatric emphasis - ISKDC criteria, steroid protocol, when NOT to biopsy, FRNS/SDNS management
✅ Prognosis - disease-by-disease
✅ At least 3-4 standard book citations by name and chapter
Sources: Brenner & Rector's The Kidney (2-Volume Set); NKF Primer on Kidney Diseases, 8th Ed.; Robbins, Cotran & Kumar Pathologic Basis of Disease; Comprehensive Clinical Nephrology, 7th Ed.; Campbell Walsh Wein Urology (3-Volume Set)
This is a shared conversation. Sign in to Orris to start your own chat.