BP management
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"hypertension" AND "management" AND "guidelines"
Finding Sources
Reading Article
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive data to compile a thorough response. Here is the full guide to BP management:
Blood Pressure Management - Comprehensive Clinical Guide
1. Classification
| Category | Systolic (mm Hg) | Diastolic (mm Hg) |
|---|---|---|
| Normal | < 120 | < 80 |
| Elevated | 120-129 | < 80 |
| Stage 1 Hypertension | 130-139 | 80-89 |
| Stage 2 Hypertension | ≥ 140 | ≥ 90 |
| Hypertensive Crisis | > 180 | > 120 |
(AHA/ACC 2017/2025 framework)
2. BP Targets
- Most adults: < 130/80 mm Hg (standard clinical measurement)
- High-risk adults using standardized measurement protocols (e.g., SPRINT-like): < 120 mm Hg systolic - trials show reduced cardiovascular mortality even in patients ≥75 years, including frail elderly who are not institutionalized
- Diabetes: < 130/80 mm Hg; consider < 120/80 mm Hg in those at high CV risk but low medication risk
- CKD (KDIGO 2021): SBP < 130 mm Hg; ACEi/ARB preferred
- Elderly (≥65 years): Same targets apply, but start drugs at low doses; monitor for orthostatic hypotension; use ambulatory or home BP monitoring to avoid overtreatment
Key nuance: Standard office BP readings are on average ~10 mm Hg higher than standardized protocol readings. A clinical target of < 130 mm Hg approximately corresponds to a SPRINT-protocol target of < 120 mm Hg. - Goldman-Cecil Medicine, p. 755
3. Non-Pharmacological (Lifestyle) Therapy
Should always accompany or precede drug therapy for Stage 1 hypertension, and adjunct drug therapy in Stage 2:
- Weight loss - reducing BMI in overweight/obese patients
- Sodium restriction - lowers BP in salt-sensitive patients
- DASH diet
- Alcohol limitation - < 20 g/day in women, < 40 g/day in men
- Regular aerobic exercise
- Smoking cessation (reduces overall CV risk)
- Renal denervation - evidence supports use in well-defined resistant hypertension
- Bariatric surgery - can normalize BP in grossly obese individuals
4. First-Line Drug Classes
| Class | Key Agents | Primary Mechanism |
|---|---|---|
| Thiazide/Thiazide-like diuretics | Chlorthalidone, indapamide, HCTZ | Na+ excretion → volume reduction |
| Calcium channel blockers (CCBs) | Amlodipine (DHP), verapamil, diltiazem | Vasodilation (DHP) or rate/conduction control |
| ACE inhibitors (ACEi) | Lisinopril, ramipril, enalapril | Block angiotensin I → II conversion |
| Angiotensin receptor blockers (ARBs) | Losartan, valsartan, irbesartan | Block AT1 receptor |
Grade I, Level A recommendation (US guidance): "For initiation of antihypertensive drug therapy, first-line agents include thiazide diuretics, CCBs, and ACE inhibitors or ARBs." - Comprehensive Clinical Nephrology, 7th Ed.
Beta-blockers are NOT first-line for uncomplicated hypertension - they are generally less effective at lowering BP and less protective against stroke. They are reserved for compelling indications (heart failure, ischemic heart disease, rate control in AF). - Goldman-Cecil Medicine
5. Treatment Algorithm
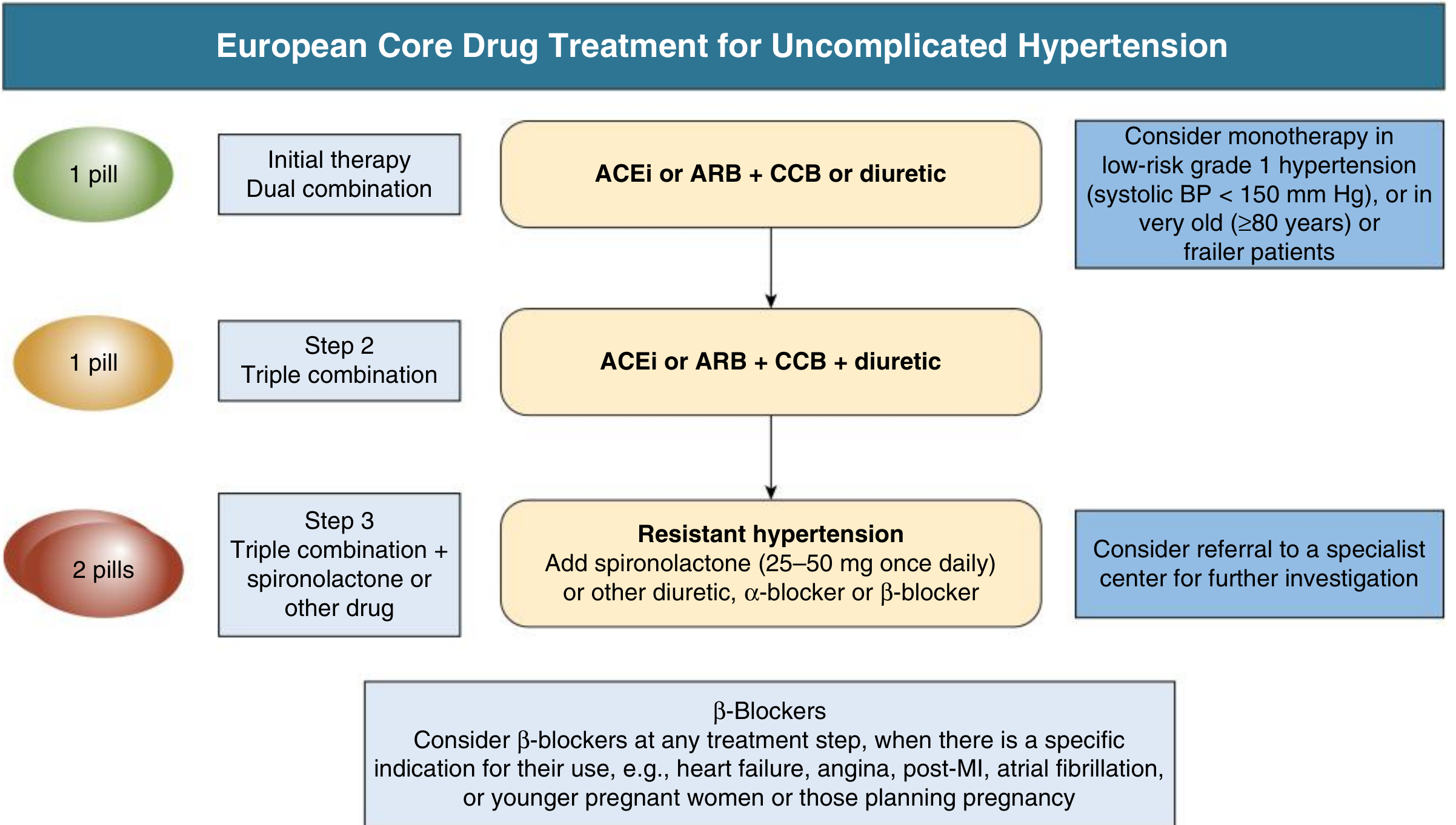
Step-by-Step Approach:
Step 1 - Initial therapy (dual combination):
- ACEi or ARB + CCB or thiazide diuretic
- Prefer combination for Stage 2 (BP > 20/10 mm Hg above target) - Grade I, Level C
- Monotherapy reasonable for Stage 1 (BP goal < 130/80 mm Hg) - Grade IIa, Level C
- Consider monotherapy in low-risk grade 1 (SBP < 150), very old (≥80 years), or frail patients
Step 2 - Triple combination (if Step 1 insufficient):
- ACEi or ARB + CCB + thiazide/thiazide-like diuretic
Step 3 - Resistant hypertension:
- Add spironolactone 25-50 mg once daily (most evidence)
- Alternatives: other diuretics, alpha-blocker, or beta-blocker
- Consider specialist referral
Beta-blockers: Add at any step when there is a specific indication (heart failure, angina, post-MI, AF, or younger pregnant women planning pregnancy).
6. Compelling Indications - Drug Choice by Condition
| Condition | Preferred Agent(s) |
|---|---|
| Heart failure (HFrEF) | ACEi/ARB, beta-blocker, aldosterone antagonist, ARNI |
| Post-MI / CAD | Beta-blocker, ACEi/ARB |
| CKD / proteinuria | ACEi or ARB (first-line for renoprotection) |
| Diabetes | ACEi or ARB preferred (especially with albuminuria) |
| Isolated systolic HTN (elderly) | Thiazide-like diuretic, CCB (amlodipine) |
| Atrial fibrillation (rate control) | Beta-blocker, non-DHP CCB (verapamil/diltiazem) |
| Resistant HTN | Spironolactone (or eplerenone) |
| Post-renal transplant | Thiazide, CCB, ACEi/ARB (after 6-12 months with stable graft) |
ACEi + ARB combination must be avoided - minimal added BP lowering with high risk of renal impairment and hyperkalemia. - Goldman-Cecil Medicine
7. Key Drug Notes
Thiazide-like diuretics (chlorthalidone > HCTZ): Chlorthalidone and indapamide preferred over HCTZ due to longer half-life and better 24-hour coverage. Risk of hyponatremia (especially in elderly), hypokalemia, hyperuricemia.
CCBs: Amlodipine (DHP) is preferred for uncomplicated HTN. Non-DHP agents (verapamil, diltiazem) are potent CYP3A4 inhibitors - statin dose adjustment required (e.g., simvastatin ≤ 20 mg with amlodipine; lower with verapamil/diltiazem). Grapefruit juice raises DHP levels (except amlodipine).
ACEi: Can cause dry cough (switch to ARB). Contraindicated in bilateral renal artery stenosis and pregnancy. Monitor K+ and creatinine.
ARBs: Better tolerated than ACEi (no cough). Contraindicated in pregnancy.
Spironolactone vs. eplerenone: Spironolactone lowers BP more effectively; eplerenone more selective (less gynecomastia, erectile dysfunction). Avoid both if eGFR < 45 mL/min/1.73 m².
Emerging agents:
- ARNI (sacubitril/valsartan): Established in HFrEF; effective 24-hour BP lowering including nocturnal BP; superior to ARB alone - potential role in hypertension
- SGLT2 inhibitors (empagliflozin, dapagliflozin): BP lowering via natriuresis; contributes to CV and renal outcome benefits
8. Hypertensive Emergency vs. Urgency
| Feature | Emergency | Urgency |
|---|---|---|
| BP level | SBP > 180 or DBP > 120 | Same BP threshold |
| Target organ damage | Present (stroke, MI, AKI, retinopathy) | Absent |
| Route | IV medications | Oral medications |
| Rate of reduction | Controlled reduction (not too rapid) | Over hours to days |
Target organ damage examples: LV hypertrophy, albuminuria, impaired renal function, unstable angina, acute MI, encephalopathy, aortic dissection.
IV agents for hypertensive emergency:
- CCBs: Nicardipine, clevidipine
- Nitric oxide vasodilators: Sodium nitroprusside, nitroglycerin
- Adrenergic blockers: Labetalol, esmolol, phentolamine
- Vasodilator: Hydralazine
- Dopamine agonist: Fenoldopam
Initial goal is a controlled reduction - not rapid normalization, which risks hypoperfusion of target organs. - Lippincott Pharmacology
9. Special Populations
| Population | Key Consideration |
|---|---|
| Elderly / Frail | Start low, go slow; monitor orthostatic BP; avoid overtreatment with home/ambulatory monitoring |
| Pregnancy | Methyldopa, labetalol, nifedipine are safe; ACEi/ARB contraindicated; hydralazine still used for severe cases |
| CKD | ACEi/ARB for renoprotection; avoid K+-sparing agents at eGFR < 45 |
| Diabetes | ACEi/ARB first-line with albuminuria; target < 130/80 |
| Post-transplant | Standard first-line drugs after 6-12 months; CNIs (cyclosporine, tacrolimus) are potent CYP3A4 inhibitors |
10. Drug Interactions to Know
- NSAIDs (except sulindac, celecoxib): Raise BP; impair kidney function
- Acetaminophen: Can also raise BP via unknown mechanism
- Verapamil/diltiazem + statins: Significant CYP3A4 inhibition; reduce statin dose
- Grapefruit + DHP CCBs (not amlodipine): Up to 24-hour increase in drug levels
- ACEi/ARB + K+-sparing diuretics: High hyperkalemia risk
- Iron + methyldopa: Reduces methyldopa absorption by ~50%
2025 Guideline Update
The 2025 AHA/ACC Hypertension Guideline (PMID: 40811516) replaces the 2017 guideline and is intended as a "living document." It covers updated evidence from 2015-2024 and refines recommendations for BP targets, drug selection, and special populations. Note there is an erratum published (PMID: 42160500).
Sources: Comprehensive Clinical Nephrology 7th Ed. | Goldman-Cecil Medicine | Goodman & Gilman's Pharmacological Basis of Therapeutics | Lippincott Illustrated Reviews Pharmacology | Brenner and Rector's The Kidney
DM medication
Finding Sources
Searching PubMed
"type 2 diabetes" AND "pharmacotherapy" AND "guidelines"
Finding Sources
Searching PubMed
"diabetes mellitus" AND "GLP-1" AND "SGLT2"
Finding Sources
Finding Sources
Reading Article
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I have comprehensive data from multiple sources. Now let me compile the complete guide.
Diabetes Mellitus (DM) Medications - Comprehensive Guide
Diagnosis Recap
| Test | Diabetes | Prediabetes |
|---|---|---|
| Fasting plasma glucose | ≥ 126 mg/dL | 100-125 mg/dL |
| 2-hr postprandial glucose | ≥ 200 mg/dL | 140-199 mg/dL |
| HbA1c | ≥ 6.5% | 5.7-6.4% |
Drug Classes at a Glance
| Class | Key Agents | Mechanism | HbA1c Lowering | Hypo Risk | Weight Effect |
|---|---|---|---|---|---|
| Biguanides | Metformin | ↓ hepatic glucose output | 1-2% | No | Neutral |
| Sulfonylureas | Glipizide, Glimepiride, Glyburide | ↑ insulin secretion | 1-2% | Yes | Gain |
| Meglitinides | Repaglinide, Nateglinide | ↑ insulin secretion (prandial) | 0.5-1% | Yes (rarely) | Gain |
| TZDs | Pioglitazone | ↓ insulin resistance (PPARγ) | 0.5-1.4% | No | Gain |
| DPP-4 inhibitors | Sitagliptin, Linagliptin, Saxagliptin | ↑ GLP-1/GIP → glucose-dependent insulin ↑ | 0.5-0.8% | No | Neutral |
| GLP-1 RAs | Semaglutide, Liraglutide, Dulaglutide | Glucose-dependent insulin ↑, glucagon ↓, gastric emptying ↓ | 0.8-2% | No | Loss |
| SGLT2 inhibitors | Empagliflozin, Dapagliflozin, Canagliflozin | ↑ urinary glucose excretion | 0.5-1% | No | Loss |
| α-glucosidase inhibitors | Acarbose, Miglitol | ↓ intestinal glucose absorption | 0.5-0.8% | No | Neutral |
| Insulin | Multiple formulations | Direct glucose uptake | Variable | Yes | Gain |
1. Biguanides - Metformin
Mechanism: Activates AMP-kinase → suppresses hepatic gluconeogenesis; increases peripheral glucose utilization; does not stimulate insulin secretion.
Why it's first-line:
- No hypoglycemia risk
- Weight neutral or modest weight loss
- Cheap, widely available
- Proven CV safety (UKPDS)
- Well-established safety profile
Dosing: Start 500 mg with meals, titrate to 1000-2000 mg/day in divided doses. Extended-release formulation available.
Key adverse effects:
- GI side effects (nausea, diarrhea) - take with food, titrate slowly
- Lactic acidosis (rare, primarily in renal/hepatic failure)
- Vitamin B12 deficiency with long-term use - monitor levels
Contraindications:
- eGFR < 30 mL/min (use with caution 30-45)
- Active liver disease
- Contrast dye administration (hold temporarily)
- Excessive alcohol use
2. Sulfonylureas
Mechanism: Bind SUR1 subunit of K+ATP channels on beta cells → depolarization → Ca²+ influx → insulin secretion (glucose-independent).
Agents:
- First-gen (rarely used): Tolbutamide, chlorpropamide
- Second-gen (preferred): Glipizide, glimepiride, glyburide
Key points:
- Glipizide and glimepiride preferred over glyburide in elderly and CKD (glyburide has active metabolites → accumulation → prolonged hypoglycemia)
- Most common cause of hypoglycemia among oral agents
- Weight gain occurs
- Metabolized by liver; excreted by kidney
3. Meglitinides
Mechanism: Same as sulfonylureas (K+ATP channel closure) but shorter-acting - taken with each meal for prandial coverage.
- Repaglinide - stronger, also reduces FPG
- Nateglinide - primarily postprandial effect
Key advantage over SUs: Shorter action, lower hypoglycemia risk, useful when meal timing is irregular.
4. Thiazolidinediones (TZDs / Glitazones)
Mechanism: PPARγ agonists → ↑ insulin sensitivity in adipose, muscle, and liver. Redistribution of fat from visceral to subcutaneous.
Agents: Pioglitazone (available); Rosiglitazone (restricted/unavailable in many countries due to CV concerns)
Advantages: Durable glycemic control; pioglitazone has CV benefit data (PROactive trial)
Adverse effects:
- Fluid retention / edema (3-4%; up to 15% with insulin)
- Heart failure - contraindicated in NYHA class III-IV
- Weight gain
- Bone fractures (especially in women)
- Bladder cancer risk with pioglitazone (inconsistent data, ongoing monitoring)
- Check LFTs before initiation; avoid if ALT > 2.5x ULN
5. DPP-4 Inhibitors ("Gliptins")
Mechanism: Inhibit dipeptidyl peptidase-4 → prevents breakdown of endogenous GLP-1 and GIP → glucose-dependent ↑ insulin, ↓ glucagon.
Agents: Sitagliptin (Januvia), Linagliptin (Tradjenta), Saxagliptin (Onglyza), Alogliptin (Nesina)
Key advantages: Well tolerated, weight neutral, no hypoglycemia, once-daily dosing.
Renal dosing:
- Sitagliptin: reduce dose for eGFR < 45
- Saxagliptin: reduce for eGFR < 45; also ↑ HF risk
- Alogliptin: reduce for eGFR < 60; potential liver risk
- Linagliptin: No renal dose adjustment (biliary excretion) - preferred in CKD
Adverse effects: Nasopharyngitis/URI, rare pancreatitis, joint pain (FDA warning), angioedema/SJS (rare). Do not combine with GLP-1 RAs (redundant mechanism).
6. GLP-1 Receptor Agonists
Mechanism: Activate GLP-1 receptors → glucose-dependent insulin secretion, ↓ glucagon, ↓ gastric emptying, ↑ satiety → weight loss.
Agents and dosing:
| Agent | Route | Frequency | CV Data |
|---|---|---|---|
| Semaglutide (Ozempic/Rybelsus) | SC or oral | Weekly (SC) / Daily (oral) | SUSTAIN-6: CV benefit |
| Liraglutide (Victoza) | SC | Daily | LEADER: CV benefit |
| Dulaglutide (Trulicity) | SC | Weekly | REWIND: CV benefit |
| Exenatide (Byetta/Bydureon) | SC | Twice daily / weekly | - |
| Tirzepatide (Mounjaro) | SC | Weekly | Dual GIP+GLP-1 RA; large HbA1c and weight reduction |
Cardiovascular/Renal benefits: SGLT2 inhibitors and GLP-1 RAs both reduce MACE, HF hospitalizations, and kidney disease progression. The 2025 BMJ living guideline strongly recommends GLP-1 RAs in high CV/CKD risk patients.
Adverse effects: Nausea, vomiting, diarrhea (dose-dependent, usually transient). Rare: pancreatitis, thyroid C-cell tumors (avoid in MEN2/family history of medullary thyroid cancer). Injection site reactions.
Tirzepatide (dual GIP+GLP-1 RA): largest weight loss data of any approved agent; weak recommendation in favor for patients with obesity across all CV risk strata (BMJ 2025 guideline).
7. SGLT2 Inhibitors ("Flozins")
Mechanism: Inhibit SGLT2 in proximal tubule → ↑ urinary glucose excretion (glycosuria); lowers glucose threshold from ~180 mg/dL to ~40 mg/dL. Also promotes natriuresis → BP reduction.
Agents: Empagliflozin (Jardiance), Dapagliflozin (Farxiga), Canagliflozin (Invokana), Ertugliflozin (Steglatro)
HbA1c reduction: 0.5-1%; greater at higher baseline HbA1c.
Weight loss: 2-5 kg (caloric loss via glycosuria).
Key organ-protective benefits:
- Heart failure: Reduced HF hospitalization in both HFrEF and HFpEF
- CKD: Delays progression (CREDENCE, DAPA-CKD trials)
- CV outcomes: Reduced MACE in high-risk patients (EMPA-REG, CANVAS, DECLARE)
2025 BMJ Living Guideline (PMID: 40813129):
- Higher CV/CKD risk or HF: Strong recommendation FOR SGLT2 inhibitors
- Moderate risk: Weak recommendation in favor
- Lower risk: Weak recommendation against
Dosing:
- Canagliflozin: 100-300 mg daily (avoid if eGFR < 30)
- Dapagliflozin: 10 mg daily (5 mg in hepatic failure)
- Empagliflozin: 10-25 mg daily
Adverse effects:
- Genitourinary infections (UTIs, candidal vulvovaginitis)
- Euglycemic DKA (especially Type 1; not approved for T1DM due to this risk)
- Volume depletion / hypotension
- Fournier's gangrene (rare)
- Canagliflozin: ↑ risk of lower limb amputations and fractures
8. α-Glucosidase Inhibitors
Mechanism: Competitively inhibit intestinal α-glucosidases → delay digestion and absorption of complex carbohydrates → ↓ postprandial glucose.
Agents: Acarbose, Miglitol
- Acarbose: 50 mg twice daily, titrate to 100 mg TID
- Miglitol: 25 mg TID, titrate to 50-100 mg TID
Adverse effects: Flatulence, diarrhea, abdominal cramping - major limiting factor.
Contraindications: IBD, colonic ulceration, intestinal obstruction, renal failure (miglitol).
9. Insulin
Profiles
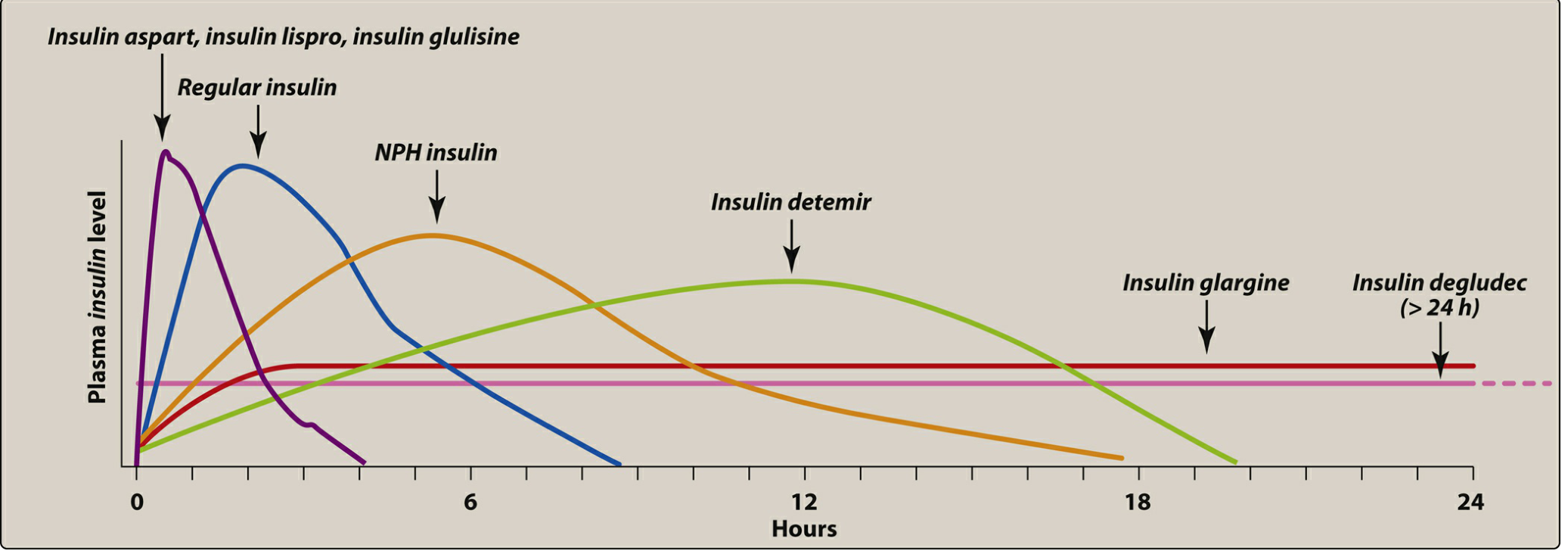
| Type | Onset | Peak | Duration | Examples |
|---|---|---|---|---|
| Rapid-acting | 15-30 min | 30-90 min | 3-5 hr | Lispro, Aspart, Glulisine |
| Short-acting | 30-60 min | 50-120 min | 6-10 hr | Regular (Humulin R) |
| Intermediate | 1-2 hr | 4-8 hr | 12-18 hr | NPH (Humulin N) |
| Long-acting | 1-4 hr | No peak | 20-24+ hr | Glargine, Detemir |
| Ultra long-acting | 1-2 hr | No peak | > 24 hr | Degludec |
| Inhaled | 12-15 min | 10-20 min | 2-3 hr | Afrezza |
Key Insulin Concepts
Basal-bolus regimen: Long-acting (once daily, e.g. glargine) + rapid-acting at each meal - most physiological approach.
Rapid-acting insulins are taken 15 min before meals (or within 15-20 min after starting eating); regular insulin 30 min before meals.
Type 1 DM: Insulin is mandatory - absolute deficiency.
Type 2 DM insulin initiation: Start with basal insulin (glargine/detemir 10 units at bedtime); titrate up by 2 units every 3 days to fasting glucose target.
Adverse effects: Hypoglycemia (most serious), weight gain, lipodystrophy at injection site (rotate sites), hypokalemia (high doses).
10. Other Agents
Amylin analog - Pramlintide (Symlin):
- Mimics amylin (co-secreted with insulin)
- ↓ postprandial glucose, glucagon, and gastric emptying
- Used as adjunct to insulin in T1DM and T2DM
Bromocriptine (Cycloset): Dopamine agonist - modest HbA1c lowering (~0.5%); mechanism unclear; limited clinical use.
Colesevelam (Welchol): Bile acid sequestrant - modest HbA1c lowering; also lowers LDL; useful in patients needing lipid-lowering.
Finerenone: Non-steroidal mineralocorticoid receptor antagonist. Weak recommendation in favor for CKD patients at higher CV risk (BMJ 2025 guideline).
Treatment Algorithm for Type 2 DM
Lifestyle modification + Metformin (if no contraindication)
│
├── ASCVD/HF/CKD present?
│ → Add GLP-1 RA or SGLT2i (evidence-based, organ-protective)
│
├── Need more glucose lowering?
│ → Add second agent from complementary class
│
├── HbA1c still above target?
│ → Triple therapy or add basal insulin
│
└── Insulin required?
→ Basal insulin first; add prandial if needed
Key 2025 guideline update (BMJ Living CPG, PMID: 40813129):
- Higher CV/CKD/HF risk: Strong recommendation for SGLT2i or GLP-1 RA
- Tirzepatide: Weakly recommended in those with obesity across all risk levels
Glycemic Targets (ADA)
| Parameter | Target |
|---|---|
| HbA1c | < 7.0% (individualize: 7.5-8% in frail elderly) |
| Fasting glucose | 80-130 mg/dL |
| 2-hr postprandial | < 180 mg/dL |
DCCT (T1DM): Tight control (HbA1c ~7.2%) reduced microvascular complications by ~60% vs. conventional (HbA1c ~8.9%).
UKPDS (T2DM): Intensive glycemic control reduced microvascular events; BP control with ACEi or beta-blocker independently reduced macrovascular events.
Special Situations
| Situation | Preferred / Avoid |
|---|---|
| CKD (eGFR < 30) | Prefer linagliptin, insulin; avoid metformin, SGLT2i, glyburide |
| HF | SGLT2i (beneficial); avoid TZDs (Class III-IV) |
| ASCVD | GLP-1 RA or SGLT2i for CV protection |
| Obesity | GLP-1 RA, SGLT2i, tirzepatide |
| Elderly | Avoid sulfonylureas (hypoglycemia), glyburide especially |
| Pregnancy | Insulin (first-line); metformin (used but crosses placenta); avoid most oral agents |
| Liver disease | Avoid metformin, TZDs; insulin preferred |
Sources: Katzung's Basic and Clinical Pharmacology 16th Ed. | Lippincott Illustrated Reviews Pharmacology | Goldman-Cecil Medicine | Goodman & Gilman's Pharmacological Basis of Therapeutics | BMJ Living CPG 2025 [PMID: 40813129]
This is a shared conversation. Sign in to Orris to start your own chat.