Anaphylaxis management
Reading File
Finding Sources
Searching PubMed
"anaphylaxis"[MeSH Terms] AND "management"[MeSH Terms]
Reading File
Reading File
Searching PubMed
anaphylaxis epinephrine treatment
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have all the content needed for a comprehensive, well-structured answer. Let me compile it.
Anaphylaxis Management
Anaphylaxis is a life-threatening systemic hypersensitivity reaction requiring immediate recognition and treatment. Delay of even a few minutes can lead to hypoxia, circulatory collapse, and death.
Pathophysiology (Brief)
Mast cells (and basophils) activated by IgE-bound allergens release histamine, tryptase, prostaglandin D4, and leukotriene C4. These target the cardiovascular, cutaneous, respiratory, and GI systems, causing vasodilation, increased permeability, bronchospasm, and smooth muscle contraction. Non-IgE mechanisms (e.g., direct mast cell activation by radiocontrast, NSAIDs, opioids) produce an identical clinical picture.
Diagnosis - Clinical Criteria
Anaphylaxis is highly likely when any one of the following three criteria is met:
- Acute onset of illness with skin/mucosal involvement (hives, flushing, swollen lips/tongue) PLUS either respiratory compromise OR reduced BP/end-organ symptoms
- Two or more of the following occurring rapidly after exposure to a likely allergen: skin/mucosal symptoms, respiratory compromise, reduced BP, or persistent GI symptoms
- Reduced BP after exposure to a known allergen
Common Triggers
| Category | Examples |
|---|---|
| Foods | Peanuts, tree nuts, shellfish, milk, eggs |
| Medications (IgE) | Beta-lactam antibiotics |
| Medications (non-IgE) | NSAIDs, radiocontrast media, opioids |
| Venoms | Hymenoptera (wasps, bees, fire ants) |
| Perioperative | Neuromuscular blockers, latex, chlorhexidine |
| Biologics | Monoclonal antibodies, chemotherapy agents |
| Idiopathic | ~20% of cases |
Clinical Manifestations
| System | Symptoms/Signs |
|---|---|
| Skin | Urticaria, flushing, angioedema, pruritus (~80-90% of cases) |
| Respiratory | Stridor, bronchospasm, dyspnea, rhinorrhea |
| Cardiovascular | Hypotension, tachycardia, syncope, dysrhythmia |
| GI | Nausea, vomiting, abdominal cramps, diarrhea |
| Neurological | Altered consciousness, dizziness, seizure |
Note: Cardiovascular collapse can occur without skin features, particularly with insect sting anaphylaxis or perioperative reactions.
Management Algorithm
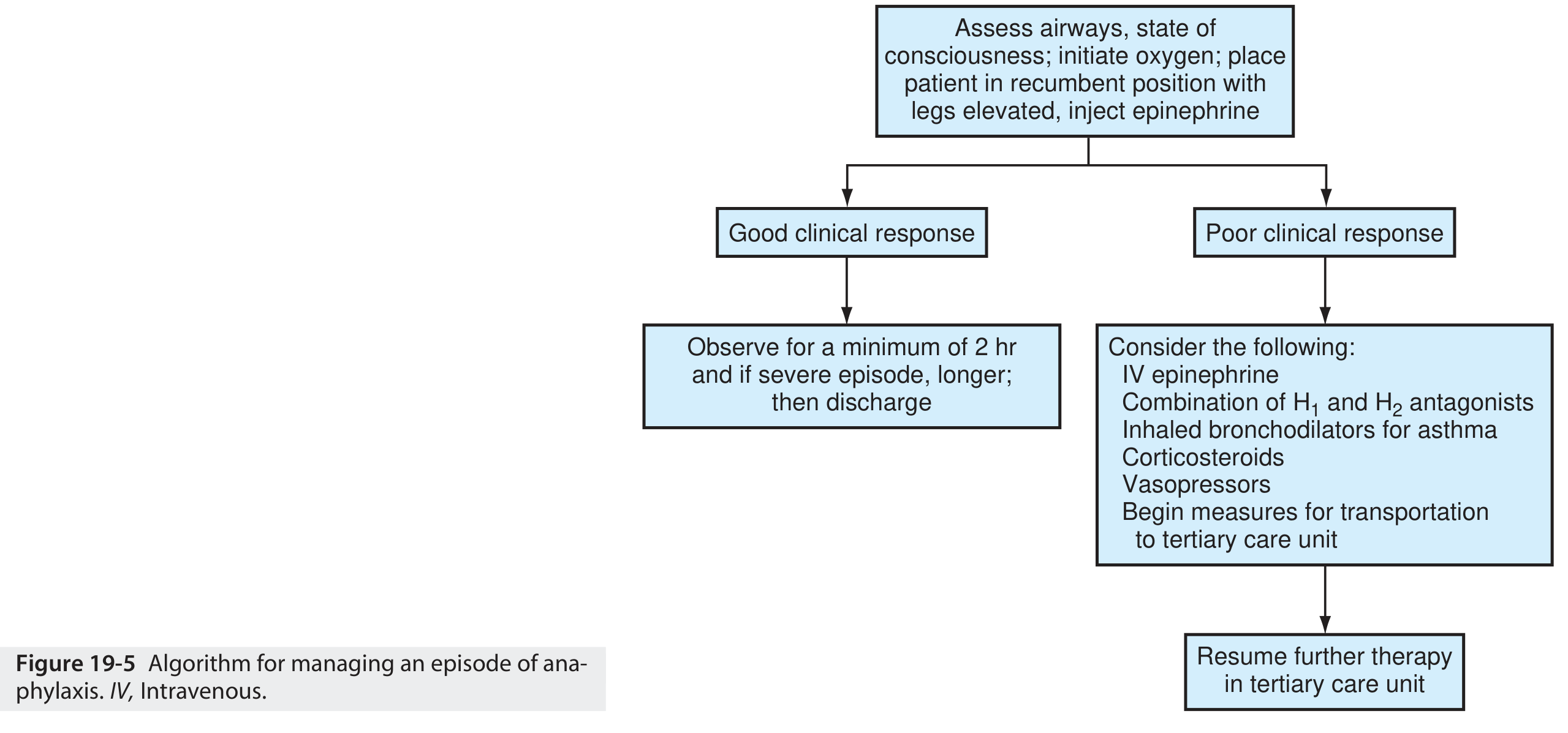
Step-by-Step Treatment
1. Immediate Actions (Simultaneous)
- Remove / stop the trigger (discontinue IV infusion, remove insect stinger)
- Call for help; activate emergency response if in community setting
- Positioning: supine with legs elevated (hypotension); left lateral decubitus (pregnancy); allow sitting up if respiratory distress or vomiting - do not stand the patient up suddenly
- Supplemental oxygen (high-flow, 100%)
- IV/IO access - large-bore peripheral line
- Continuous monitoring - cardiac, pulse oximetry
2. Epinephrine - First-Line, No Contraindications
Epinephrine is the sole first-line drug. There are no absolute contraindications. Antihistamines and corticosteroids are adjuncts only and must never precede or replace epinephrine.
Intramuscular (preferred route):
- Adults: 0.3-0.5 mg (0.3-0.5 mL of 1:1000 / 1 mg/mL solution) IM in the lateral thigh (vastus lateralis)
- Children: 0.01 mg/kg of 1:1000 solution IM in the lateral thigh (max 0.5 mg)
- Can be repeated every 5-10 minutes - up to 30% of patients require more than one dose
- IM into the vastus lateralis achieves peak plasma concentration in ~8 minutes vs. ~34 minutes subcutaneously - subcutaneous route is no longer recommended
Intravenous epinephrine (refractory hypotension after multiple IM doses + volume):
- Prepare: 1 mg in 1000 mL NS or D5W → concentration 1 mcg/mL
- Adults: start at 1 mcg/min, titrate up to maximum 10 mcg/min
- Children: 0.1 mcg/kg/min, up to 1.5 mcg/kg/min
- Requires cardiac monitoring; use central line if possible (extravasation causes tissue necrosis)
Mechanism of benefit:
- α1: vasoconstriction, reduces mucosal edema
- β1: positive inotropy and chronotropy
- β2: bronchodilation, stabilizes mast cells/basophils and reduces further mediator release
3. IV Fluids (Circulatory Collapse)
- Large volumes may be required - up to 1-2 L bolus initially in adults; repeat as needed
- Crystalloids (normal saline or Ringer's lactate) are first choice
- Massive fluid shifts can rapidly reduce intravascular volume due to increased capillary permeability
4. Airway Management
- Maintain airway patency - early intubation if laryngeal edema is developing
- If laryngeal edema does not respond rapidly to epinephrine: cricothyrotomy or tracheotomy
- Nebulized albuterol for persistent bronchospasm:
- Adults/children: 2.5 mg in 3 mL NS, repeat as needed or continuous
- Add ipratropium: adults 0.5 mg; children 0.25 mg in 3 mL NS
5. Adjunct Medications (Secondary - After Epinephrine)
| Drug | Indication | Dose |
|---|---|---|
| H1 antihistamine (diphenhydramine) | Skin symptoms, itch | Adults: 25-50 mg IM/IV; Children: 12.5-25 mg IM/IV |
| H2 antihistamine (famotidine/ranitidine) | Adjunct to H1 | Adults: 20 mg IV |
| Corticosteroids (methylprednisolone) | Adjunct - no acute benefit; may reduce biphasic risk (unproven) | Adults: 125-250 mg IV; Children: 1-2 mg/kg IV |
| Glucagon | Beta-blocker on board, epinephrine-refractory | 1-5 mg IV over 5 min, then 5-15 mcg/min infusion |
| Albuterol (inhaled) | Bronchospasm | 2.5 mg nebulized |
Corticosteroids have no significant immediate effect and do not reliably prevent biphasic reactions, but are commonly given. They should never delay epinephrine. - Washington Manual
Antihistamines relieve skin symptoms and may shorten reaction duration but have no effect on cardiovascular or respiratory components.
6. Refractory Anaphylaxis / Vasopressor Support
If hypotension persists despite epinephrine and IV fluids:
| Vasopressor | Dose |
|---|---|
| Norepinephrine | 0.05-0.5 mcg/kg/min IV (titrate) |
| Dopamine | 5-20 mcg/kg/min IV (titrate) |
| Phenylephrine | 1-5 mcg/kg/min IV |
| Vasopressin | 0.01-0.04 units/min IV |
Special Situations
Beta-Blocker Use
Epinephrine may have blunted effect. Glucagon (1-5 mg IV bolus then infusion) bypasses beta-receptors via cAMP-mediated pathway. Monitor for nausea/vomiting - have antiemetic ready.
ACE Inhibitor Use
Associated with increased anaphylaxis severity. ACE inhibitors block bradykinin degradation, worsening hypotension.
Radiocontrast Media Premedication
For patients with prior contrast anaphylaxis:
- Prednisone 50 mg oral at 13 h, 7 h, and 1 h before
- Diphenhydramine 50 mg oral 1 h before
- Consider ephedrine 25 mg oral 1 h before
- Consider H2 antagonist (famotidine 20 mg) 3 h before
Pregnancy
Position patient in left lateral decubitus to prevent vena cava compression. Epinephrine is still indicated - the risk of untreated anaphylaxis outweighs fetal risk.
Biphasic Reactions
- Occur in up to 20% of anaphylaxis cases - symptoms recur without re-exposure to the trigger
- Most occur within 8 hours, but can be delayed up to 72 hours
- Risk factors: hypotension, wide pulse pressure, unknown trigger, >1 epinephrine dose, prior anaphylaxis, delayed epinephrine administration
- Corticosteroids have not been shown to reliably prevent biphasic reactions
Disposition
| Situation | Disposition |
|---|---|
| Complete symptom resolution, low risk | Observe minimum 1 hour, then discharge |
| Increased biphasic risk factors (see above) | Observe 4-6 hours minimum |
| Protracted anaphylaxis, significant hypotension, airway involvement, >2 epinephrine doses | Hospitalize |
| Poor social support or unable to obtain auto-injector | Hospitalize |
Discharge Instructions
Every patient discharged after anaphylaxis must receive:
- Epinephrine auto-injector (EpiPen) - 2 devices prescribed; demonstrate use
- Individualized anaphylaxis action plan in writing
- Allergen avoidance counseling
- Medical ID (bracelet/wallet card) for known trigger
- Allergist/immunologist referral - for trigger workup, venom immunotherapy eligibility, and long-term management
Key Points Summary
- Epinephrine IM (lateral thigh) is always first-line - give it early, give it without hesitation
- Studies show only ~30% of prehospital patients and 50-70% of ED patients with anaphylaxis actually receive epinephrine - this is a significant care gap
- Antihistamines and steroids are adjuncts and must not delay or replace epinephrine
- Beta-blocker patients may need glucagon for refractory bronchospasm/hypotension
- Observe for biphasic reactions; discharge planning must include auto-injector prescription and follow-up
Sources:
- ROSEN's Emergency Medicine: Concepts and Clinical Practice, Chapter 106
- Goldman-Cecil Medicine, Chapter 233 (Schwartz & Castells)
- Washington Manual of Medical Therapeutics, Chapter on Allergy/Immunology
- Textbook of Family Medicine 9e, Chapter 19
Recent guideline: Golden DBK et al. "Anaphylaxis: A 2023 practice parameter update." Ann Allergy Asthma Immunol 2024 Feb [PMID: 38108678] - confirms epinephrine as sole first-line agent and updates observation period evidence.
How to diagnose anaphylaxis and management
Finding Sources
Finding Sources
Searching PubMed
anaphylaxis diagnosis criteria
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a complete, well-structured answer combining diagnosis and management.
Anaphylaxis: Diagnosis and Management
1. Definition
Anaphylaxis is a severe, life-threatening systemic hypersensitivity reaction caused by the rapid release of mediators (histamine, tryptase, prostaglandin D4, leukotriene C4) from mast cells and basophils. The principal target systems are the cardiovascular, cutaneous, respiratory, and gastrointestinal systems. Both IgE-mediated and non-IgE-mediated (direct mast cell activation) mechanisms produce the same clinical picture.
2. Diagnosis
Anaphylaxis is primarily a CLINICAL diagnosis
Laboratory tests take time and are rarely helpful acutely. The NIAID/FAAN and World Allergy Organization (WAO) diagnostic criteria (validated sensitivity 95-97%, specificity 71-82%) are:
NIAID/FAAN + WAO Diagnostic Criteria (Box 106.5, Rosen's)
Anaphylaxis is HIGHLY LIKELY when ANY ONE of the following three criteria is met:
Criterion 1 - Acute onset (minutes to hours) of illness with skin or mucosal involvement (generalized hives, flushing, swollen lips/tongue/uvula) PLUS at least one of:
- Respiratory compromise (dyspnea, wheeze, stridor, hypoxemia)
- Reduced BP or end-organ symptoms (hypotonia, syncope, incontinence)
Criterion 2 - Two or more of the following occurring rapidly after exposure to a likely allergen:
- Skin/mucosal involvement (hives, flushing, swollen lips/tongue)
- Respiratory compromise (dyspnea, wheeze, stridor, hypoxemia)
- Reduced BP or associated symptoms (syncope, collapse)
- Persistent GI symptoms (cramping, vomiting)
Criterion 3 - Reduced BP after exposure to a known allergen for that patient:
- Adults: systolic BP <90 mmHg or >30% drop from baseline
- Infants/children: age-specific low systolic BP
Key point: Criterion 2 catches anaphylaxis without skin features - this occurs in cardiovascular collapse from insect stings or perioperative reactions and is frequently missed.
Clinical Manifestations by System
| System | Frequency | Features |
|---|---|---|
| Skin/Mucosal | 80-90% | Urticaria, flushing, pruritus, angioedema, swelling of lips/tongue/uvula |
| Respiratory | 70-80% | Stridor (laryngeal edema), bronchospasm, wheeze, cough, chest tightness, dyspnea |
| Cardiovascular | 30-50% | Hypotension, tachycardia, dysrhythmia, syncope |
| GI | 25-30% | Crampy pain, nausea, vomiting, diarrhea (more common in elderly and food-triggered) |
| CNS | 20-30% | Dizziness, altered consciousness, seizure (from hypoperfusion) |
Note: In infants and children, hypotension is uncommon; skin and respiratory features predominate.
Diagnostic Testing (Supportive, Not Acute)
| Test | Timing | Notes |
|---|---|---|
| Serum tryptase | Peak 60-90 min; measurable up to 5 h after onset | Most reliable biomarker; correlates with mast cell activation. Best for venom/drug-induced; may be normal in food-induced anaphylaxis |
| Serum histamine | Within <1 hour of onset | Very short half-life - rarely useful clinically |
| Serum IgE testing | After the acute episode | Confirms specific allergen sensitization |
| Skin prick testing | Outpatient, weeks later | Gold standard for allergy workup |
| Formula for acute tryptase | (1.2 × baseline) + 2 | A level above this supports anaphylaxis over elevated baseline (e.g., hereditary alpha-tryptasemia) |
"The absence of an elevated tryptase level does not exclude anaphylaxis." - Washington Manual
Differential Diagnosis (Harrison's 22E, Table 364-1)
| Condition | How to Distinguish |
|---|---|
| Mastocytosis | Elevated baseline tryptase; spindle-shaped mast cells on bone marrow biopsy |
| Pheochromocytoma | Elevated urine metanephrines |
| Carcinoid syndrome | Elevated urine 5-HIAA |
| Hereditary angioedema (HAE) | Decreased C4 during attacks; no urticaria |
| Acquired angioedema | Decreased C1q |
| Scombroid fish poisoning | Tryptase not elevated; negative skin test and challenge to fish |
| Vasovagal syncope | Bradycardia (not tachycardia); no urticaria, no bronchospasm |
| Panic attack | No objective signs; normal vitals and exam |
| Systemic capillary leak syndrome | Severe hypotension; no response to epinephrine/antihistamines |
3. Management
Management Algorithm
STEP 1 - Immediate Simultaneous Actions
- Remove/stop the trigger (stop IV infusion, remove insect stinger, tourniquet proximal to sting site)
- Call for help
- Position the patient:
- Hypotension → supine, legs elevated
- Respiratory distress/vomiting → allow comfortable position, elevate legs if possible
- Pregnancy → left lateral decubitus (prevents vena cava compression)
- Never stand patient up suddenly - can cause fatal cardiovascular collapse
- Supplemental high-flow oxygen (100%)
- Large-bore IV access (16-18 gauge preferred)
- Monitoring: continuous cardiac, BP, pulse oximetry
STEP 2 - Epinephrine (FIRST-LINE - No Contraindications)
Epinephrine is the sole first-line drug. Delay is associated with hypoxic encephalopathy and death. There are NO absolute contraindications in anaphylaxis.
Intramuscular (preferred):
| Patient | Dose | Site |
|---|---|---|
| Adults | 0.3-0.5 mg (0.3-0.5 mL of 1:1000 / 1 mg/mL) | IM anterolateral thigh (vastus lateralis) |
| Children | 0.01 mg/kg of 1:1000 solution (max 0.5 mg) | IM anterolateral thigh |
- Repeat every 5-10 minutes - up to 30% need more than one dose
- IM into the thigh reaches peak plasma level in ~8 minutes vs ~34 minutes subcutaneously
- Subcutaneous and inhaled routes are no longer recommended
- Auto-injectors (EpiPen 0.3 mg; EpiPen Jr 0.15 mg) are acceptable alternatives
Why epinephrine works:
| Receptor | Effect |
|---|---|
| α1 | Vasoconstriction, ↑ peripheral resistance, ↓ mucosal edema |
| β1 | Positive inotropy and chronotropy |
| β2 | Bronchodilation; stabilizes mast cells/basophils → ↓ further mediator release |
IV Epinephrine (only for refractory hypotension after multiple IM doses + IV fluids):
- Prepare: 1 mg in 1000 mL NS or D5W → 1 mcg/mL concentration
- Adults: start 1 mcg/min, titrate to max 10 mcg/min
- Children: 0.1 mcg/kg/min, titrate to max 1.5 mcg/kg/min
- Requires cardiac monitoring; use central line if possible (extravasation → tissue necrosis)
STEP 3 - IV Fluids
- Start rapid isotonic crystalloid (normal saline):
- Adults: 1000 mL IV in the first 5 min; several liters may be needed
- Children: 20-30 mL/kg in increments
- Massive fluid shifts occur from capillary leak - aggressive resuscitation may be required
STEP 4 - Airway Management
- Ensure patent airway at all times
- Early endotracheal intubation if laryngeal edema is developing - do not wait for full obstruction
- If laryngeal edema does not respond rapidly to epinephrine: cricothyrotomy or tracheotomy
- Nebulized bronchodilators for bronchospasm:
- Albuterol: 2.5 mg in 3 mL NS (adults and children), repeat or continuous
- Ipratropium: 0.5 mg (adults) / 0.25 mg (children) in 3 mL NS
STEP 5 - Second-Line Adjuncts (AFTER Epinephrine - Never Before)
| Drug | Dose (Adult) | Dose (Child) | Role |
|---|---|---|---|
| Diphenhydramine (H1) | 50 mg IV/IM | 1 mg/kg IV/IM | Relieves skin symptoms; no effect on CVS/respiratory |
| Famotidine (H2) | 40 mg IV | 0.5 mg/kg IV | Adjunct to H1 blockade |
| Methylprednisolone | 125-250 mg IV | 1-2 mg/kg IV | No acute benefit; possibly reduces biphasic (unproven) |
| Prednisone (oral) | 40-60 mg | 1-2 mg/kg | Alternative oral steroid |
Corticosteroids have no significant immediate effect and reliable evidence showing they prevent biphasic reactions is lacking. They must never precede or delay epinephrine.
STEP 6 - Refractory Cases / Special Situations
Refractory hypotension - additional vasopressors:
| Vasopressor | Dose |
|---|---|
| Norepinephrine | 0.05-0.5 mcg/kg/min IV (titrate) |
| Dopamine | 5-20 mcg/kg/min IV (titrate) |
| Phenylephrine | 1-5 mcg/kg/min IV |
| Vasopressin | 0.01-0.04 units/min IV |
Patient on beta-blockers:
- Epinephrine may have blunted effect
- Glucagon 1-5 mg IV bolus (adults) / 20-30 mcg/kg max 1 mg (children) over 5 min, then 5-15 mcg/min infusion
- Glucagon acts via cAMP pathway, bypassing beta-receptors
- Pre-treat with antiemetic - nausea/vomiting are common side effects
4. Biphasic Reactions
- Occur in up to 20% of patients - recurrence of anaphylaxis without re-exposure
- Most within 8 hours, rarely up to 72 hours
- Corticosteroids have not been shown to reliably prevent biphasic reactions
Risk factors for biphasic reaction:
- Hypotension at presentation
- Wide pulse pressure
- Unknown trigger
-
1 dose of epinephrine required
- Prior history of anaphylaxis
- Delayed epinephrine administration
- Cutaneous signs and symptoms
5. Disposition
| Clinical Situation | Recommendation |
|---|---|
| Complete symptom resolution, low risk | Minimum 1 hour observation, then discharge (95% NPV for biphasic at 1 hr) |
| Any biphasic risk factor present | 4-6 hours observation minimum (97.3% NPV at 6 hr) |
| Protracted anaphylaxis, significant airway involvement, hypertension, >2 epinephrine doses | Hospitalize |
| Poor social support, unable to obtain auto-injector | Hospitalize |
6. Discharge - Mandatory Steps
Every patient discharged after anaphylaxis must receive:
- Two epinephrine auto-injectors prescribed - demonstrate how to use them
- Written individualized anaphylaxis action plan
- Allergen avoidance education
- Medical ID (bracelet or wallet card) listing known trigger
- Allergist/immunologist referral - for allergen confirmation (skin/IgE testing), venom immunotherapy eligibility, and long-term desensitization options
Summary - Key Priorities
| Priority | Action |
|---|---|
| #1 | Recognize anaphylaxis using NIAID/FAAN criteria |
| #2 | Give IM epinephrine (lateral thigh) immediately |
| #3 | Supine positioning + IV access + O2 |
| #4 | IV fluids for hypotension |
| #5 | Secure airway early if compromise present |
| #6 | Adjuncts (antihistamines, steroids) - second-line only |
| #7 | Observe for biphasic reaction |
| #8 | Discharge with auto-injector + action plan + follow-up |
Sources:
- ROSEN's Emergency Medicine, Chapter 106 (Box 106.5, 106.7)
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 364
- Goldman-Cecil Medicine, Chapter 233
- Washington Manual of Medical Therapeutics, Allergy/Immunology chapter
Current guideline: Golden DBK et al. Anaphylaxis: A 2023 practice parameter update. Ann Allergy Asthma Immunol 2024 Feb. [PMID: 38108678] - confirms epinephrine as sole first-line agent with no absolute contraindications, and updates biphasic reaction evidence.
Sinus bradycardia under evaluation
Finding Sources
Finding Sources
Searching PubMed
sinus bradycardia evaluation management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed - ECG images, evaluation flowchart, treatment algorithm, drug tables, and clinical details from 5 major textbooks. Let me compile the comprehensive answer.
Sinus Bradycardia: Evaluation and Management
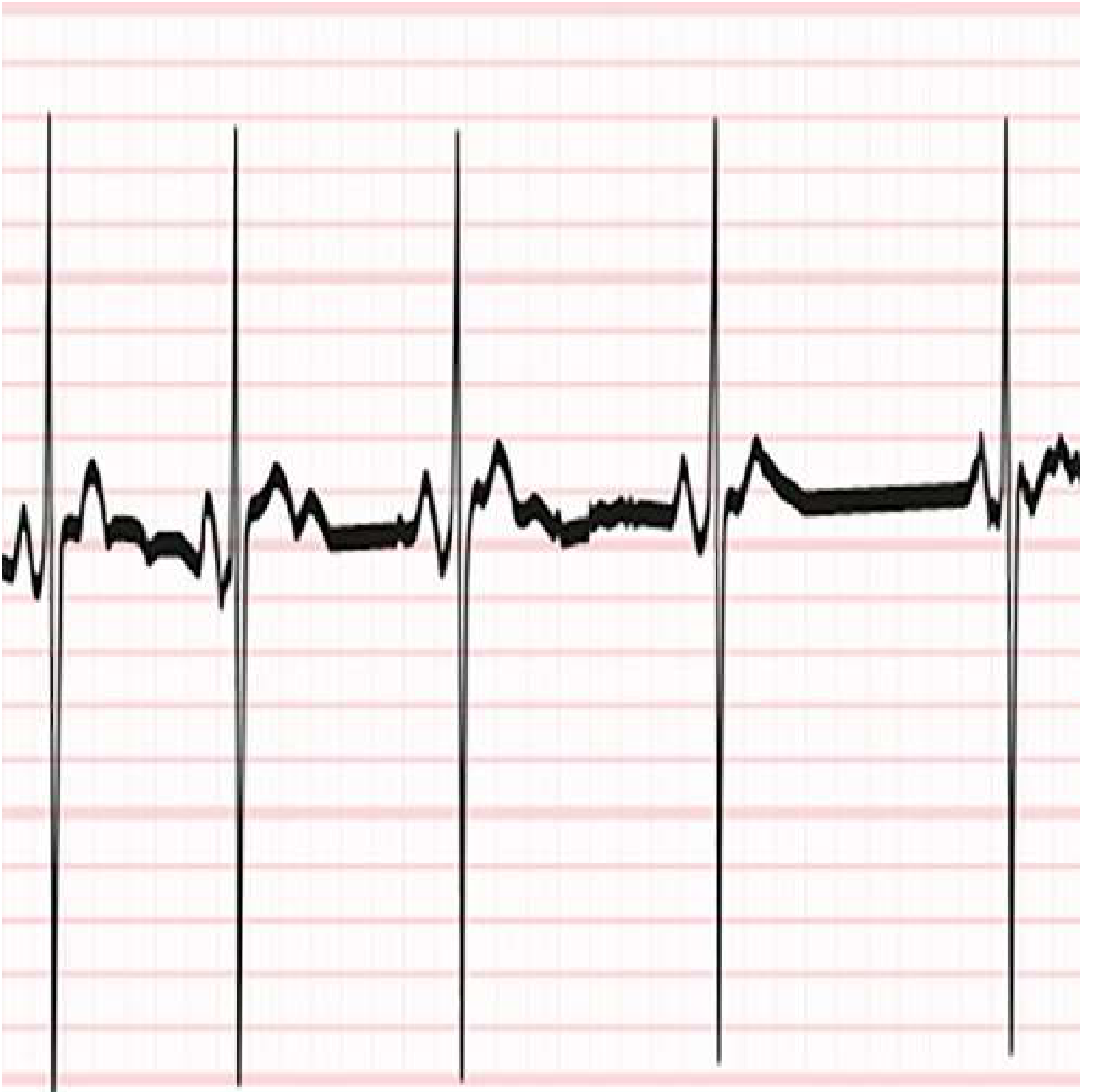
1. Definition and ECG Criteria
Sinus bradycardia is defined as a heart rate < 60 bpm arising from the sinoatrial (SA) node. Key ECG features:
- Normal P-wave morphology (upright in I, II; inverted in aVR)
- Fixed P-P interval = R-R interval (each P followed by a QRS)
- PR interval normal (0.12-0.20 s)
- Rate < 60 bpm
Rates of 45-50 bpm at rest can be physiologically normal in athletes and during sleep. A rate < 40 bpm is more specific for significant sinus node dysfunction (SND).
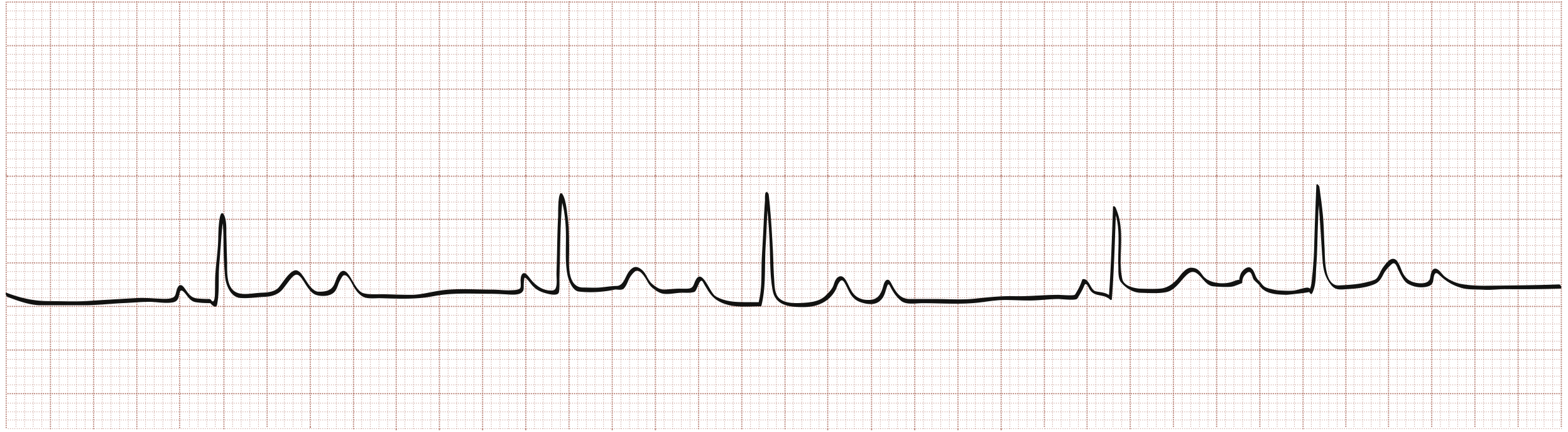
ECG Example - Sinus Bradycardia (progressive slowing from heightened vagal tone during sleep):
2. Causes
Physiologic (Normal) Causes
- Well-conditioned athletes (high vagal tone)
- Sleep, rest
- Young adults with elevated resting vagal tone
Medical Conditions
| Category | Examples |
|---|---|
| Metabolic/Endocrine | Hypothyroidism, hypothermia, hypoxia, electrolyte disturbances |
| Neurological | Increased intracranial pressure, vagal reflex (cough, pain, vomiting, visceral stimulation) |
| Cardiac | Acute inferior/right coronary MI (SA nodal artery), myocarditis, sick sinus syndrome, post-cardiac surgery, post-heart transplant |
| Infectious | Lyme disease, COVID-19 |
| Autonomic | Vasovagal (cardioinhibitory), carotid sinus hypersensitivity, spinal cord injury |
| Other | Sleep apnea, hemoperitoneum |
Drugs Causing Sinus Bradycardia (Goldman-Cecil / Harrison's)
| Drug Class | Specific Agents |
|---|---|
| Cardiac antihypertensives | Beta-blockers (including ophthalmic beta-blocker drops), non-DHP calcium channel blockers (diltiazem, verapamil), clonidine, methyldopa |
| Antiarrhythmics | Amiodarone, dronedarone, flecainide, propafenone, sotalol, quinidine |
| Cardiac glycosides | Digoxin |
| Psychoactive | SSRIs, TCAs, lithium, opioid analgesics, phenothiazines, phenytoin, cholinesterase inhibitors (donepezil), cannabis |
| Anesthetic/other | Propofol, muscle relaxants, ivabradine, remdesivir, reserpine |
Note: Beta-blocker eye drops for glaucoma are a frequently overlooked cause of systemic bradycardia.
3. Spectrum of Sinus Node Dysfunction (SND)
SND encompasses a continuum:
| Condition | Description |
|---|---|
| Sinus bradycardia | Rate < 60 bpm from SA node |
| Sinus pause / arrest | Failure of SA node to discharge; pause > 2-3 seconds |
| Sinoatrial exit block | SA node fires but impulse fails to reach atrium; classified as 1st, 2nd (Mobitz I/II), 3rd degree |
| Chronotropic incompetence | Failure to increase HR appropriately with exertion; max HR < 100 bpm on maximal exercise |
| Tachy-brady syndrome | Alternating bradyarrhythmia (sinus arrest) and tachyarrhythmia (usually AF); sinus pauses most evident after AF terminates |
| Sick sinus syndrome (SSS) | Any of the above causing symptoms (fatigue, dizziness, syncope, worsening HF) |
4. Clinical Features and Symptoms
Symptoms are caused by cerebral and peripheral hypoperfusion:
- Fatigue, exercise intolerance (most common, often underappreciated)
- Dizziness, presyncope, syncope (particularly in tachy-brady or severe pauses)
- Palpitations (in tachy-brady syndrome - the tachyarrhythmia phase)
- Worsening heart failure (chronotropic incompetence reducing cardiac output)
- Cognitive impairment (in elderly)
Asymptomatic sinus bradycardia has not been associated with adverse outcomes and does not typically warrant treatment.
5. Evaluation
Step-by-Step Approach (2018 ACC/AHA/HRS Guideline)
Evaluation Flowchart (Fuster/AHA-ACC/HRS 2018):

Step 1 - History and Physical Exam
- Full medication review (drugs most common reversible cause)
- Symptoms: onset, duration, correlation with activity/rest, syncope
- Exertional symptoms (suggest chronotropic incompetence)
- Associated conditions: thyroid disease, sleep apnea, Lyme exposure, recent MI
Step 2 - 12-Lead ECG
- Confirm sinus bradycardia
- Assess for AV block (often coexists with SND)
- Look for inferior MI pattern (RCA/SA nodal artery ischemia)
- PR interval prolongation, bundle branch block
Step 3 - Laboratory Tests
| Test | Rationale |
|---|---|
| TSH | Rule out hypothyroidism |
| Electrolytes (K+, Ca2+, Mg2+) | Electrolyte-induced bradycardia |
| Blood glucose | Hypoglycemia |
| Lyme serology | If exposure history or endemic area |
| Drug levels | Digoxin toxicity |
| CBC | Systemic illness contributing |
Step 4 - Echocardiography (Class IIa)
- Evaluate for structural heart disease (cardiomyopathy, valvular disease, wall motion abnormalities)
- Assess LV/RV function
- Look for infiltrative disease (amyloid, sarcoid)
Step 5 - Ambulatory ECG Monitoring (Class I for symptomatic patients)
| Monitoring Type | Duration | Indication |
|---|---|---|
| Holter monitor | 24-48 hours | Daily symptoms |
| Extended Holter | 7-14 days | Less frequent symptoms |
| Event recorder (patient-activated) | Up to 30 days | Infrequent symptoms |
| Implantable loop recorder (ILR) | Up to 3 years | Very infrequent episodes, unexplained syncope |
Goal: Symptom-rhythm correlation - documenting that symptoms coincide with bradycardia on the recording.
Step 6 - Exercise Stress Testing (Class IIa)
- Used to assess chronotropic incompetence
- Failure to reach 80% of age-predicted maximum HR = chronotropic incompetence
- Also useful for exertion-related symptoms
Step 7 - Advanced Imaging (Class IIa)
If infiltrative cardiomyopathy, endocarditis, or adult congenital heart disease (ACHD) is suspected:
- Cardiac MRI (sarcoidosis, amyloid, myocarditis)
- Cardiac CT (ACHD, structural)
Step 8 - Electrophysiology Study (EPS) (Class IIb - limited role)
- Not recommended as a primary diagnostic tool for SND
- May be useful when EPS is already indicated for AV block or syncope
- Can measure sinus node recovery time (SNRT) and sinoatrial conduction time
6. Management
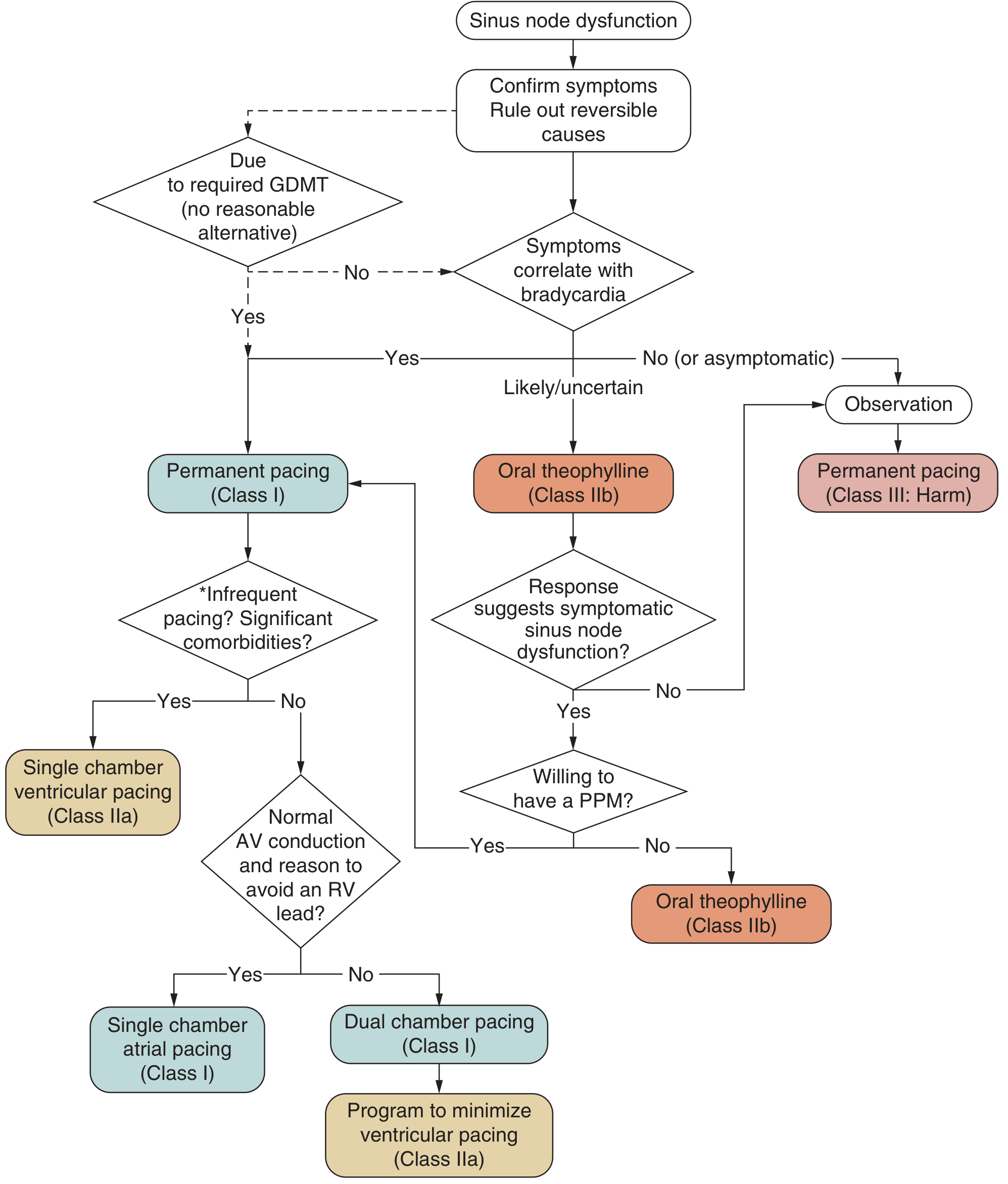
Treatment Algorithm (ACC/AHA/HRS 2018):
Acute / Emergency Management
For hemodynamically significant symptomatic bradycardia:
| Treatment | Dose | Notes |
|---|---|---|
| Atropine (first-line) | 1 mg IV q3-5 min; max 3 mg | Blocks vagal tone; works at SA and AV node |
| Dopamine infusion | 5-20 mcg/kg/min IV | If atropine fails |
| Epinephrine infusion | 2-10 mcg/min IV | Alternative to dopamine |
| Isoproterenol | 2-10 mcg/min IV | Specifically for post-heart transplant (atropine ineffective due to cardiac denervation) |
| Transcutaneous pacing | Rate 60-80 bpm | Rarely needed for sinus bradycardia; bridging measure |
| Transvenous temporary pacing | Rate 60-80 bpm | For refractory cases while awaiting definitive therapy |
Atropine is ineffective in post-cardiac transplant patients because the transplanted heart is denervated.
Chronic Management
Step 1 - Remove/Treat Reversible Causes
- Stop or reduce offending drugs (beta-blockers, CCBs, digoxin, amiodarone)
- Treat hypothyroidism, sleep apnea, Lyme disease, ischemia
- Correct electrolytes
- If drug is medically necessary, consider pacemaker to allow continued use
Step 2 - Asymptomatic Sinus Bradycardia
- Observe - no treatment required
- Permanent pacing is Class III (Harm) for asymptomatic sinus bradycardia
Step 3 - Symptomatic SND with Confirmed Symptom-Rhythm Correlation
Permanent Pacemaker (PPM) - Indications:
| Class | Indication |
|---|---|
| I (Indicated) | Symptoms directly attributable to SND |
| I (Indicated) | Symptomatic bradycardia from guideline-directed necessary drug therapy with no alternative |
| IIa (Reasonable) | Tachy-brady syndrome with bradycardia symptoms |
| IIa (Reasonable) | Symptomatic chronotropic incompetence |
| IIb (May consider) | Uncertain symptom-rhythm correlation - trial of oral theophylline first |
| III (Harmful) | Asymptomatic SND |
Choice of Pacing Mode:
| Situation | Recommended Pacing Mode |
|---|---|
| SND with intact AV conduction | Single-chamber atrial (AAI) pacing (Class I) |
| SND with uncertain/absent AV conduction | Dual-chamber (DDD) pacing (Class I) |
| Infrequent pacing expected or significant comorbidities | Single-chamber ventricular (VVI) acceptable (Class IIa) |
| Dual-chamber PPM with intact AV conduction | Program to minimize RV pacing (Class IIa) |
Atrial-based pacing is preferred over single-chamber ventricular pacing - reduces incidence of AF, pacemaker syndrome, and heart failure.
Pharmacologic Options (Limited Role)
- Oral theophylline (methylxanthine): Class IIb - may increase HR and improve symptoms; used as trial when symptom-rhythm correlation is uncertain, or as bridge/alternative when patient declines PPM
- Terbutaline (beta-agonist): Occasionally used as temporary bridge when PPM must be delayed (e.g., active infection)
7. Special Situations
| Situation | Key Consideration |
|---|---|
| Post-heart transplant | Normal resting HR is 90-110 bpm; "normal" rate may be relative bradycardia; use isoproterenol, not atropine |
| Post-cardiac surgery | SA nodal artery may be injured; temporary pacing usually sufficient while awaiting recovery |
| Acute inferior MI | Bradycardia is often transient (vagal); treat if hemodynamically compromised; rarely needs PPM |
| Spinal cord injury | Parasympathetic dominance; triggers include suctioning and turning; theophylline/aminophylline can help |
| Tachy-brady syndrome | Treat the tachycardia (antiarrhythmics, catheter ablation); PPM required if arrhythmia control not achievable |
| Beta-blocker on board | Glucagon 1-5 mg IV (bypasses beta-receptors) for refractory bradycardia |
| Athletes | Sinus bradycardia down to 30s is physiologic; evaluation only if symptomatic |
8. Summary Approach
Sinus Bradycardia Found
↓
Symptomatic? (fatigue, dizziness, syncope, exercise intolerance)
↙ ↘
NO YES
Observe Review medications → Stop offending drug if possible
Check TSH, electrolytes, ECG for MI
Echo (if structural disease suspected)
Ambulatory monitor for symptom-rhythm correlation
↓
Symptoms correlate with bradycardia?
↙ ↘
YES UNCERTAIN
Permanent Oral theophylline
Pacemaker trial → If responds → PPM
(Class I) If not → Observe
Sources:
- ROSEN's Emergency Medicine, Chapter 65
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 251 (Figure 251-3)
- Goldman-Cecil Medicine, Chapter 51 (Table 51-3)
- Fuster and Hurst's The Heart 15E, Chapter 38 (Figures 38-6, 38-7 - ACC/AHA/HRS 2018 algorithms)
- Harrison's 22E, Chapter 251 - Medical Conditions and Medications Associated with SND
Bradycardia
Finding Sources
Finding Sources
Searching PubMed
bradycardia conduction disease management guidelines
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Loading Image
Reading File
Finding Sources
I now have comprehensive material from Braunwald's, Rosen's, Goldman-Cecil, Harrison's, and Miller's Anesthesia. Let me compile the complete response.
Bradycardia: Complete Overview
1. Definition
Bradycardia is defined as a ventricular rate < 60 beats per minute (bpm). In practice, rates above 50 bpm are not usually clinically concerning. Bradycardia results from either:
- Depression of the sinoatrial (SA) node (impaired impulse generation)
- Conduction system block (impaired impulse transmission - SA exit block, AV block, infranodal block)
When the rate falls below a critical threshold, a subsidiary (escape) pacemaker from the AV junction or ventricle takes over, producing an escape rhythm.
2. Classification of Bradyarrhythmias
Bradycardia
├── SA Node Level
│ ├── Sinus bradycardia
│ ├── Sinus pause / arrest
│ ├── Sinoatrial exit block (1st, 2nd, 3rd degree)
│ ├── Sick sinus syndrome (SSS)
│ └── Tachy-brady (bradycardia-tachycardia) syndrome
│
└── AV Conduction Level
├── First-degree AV block
├── Second-degree AV block
│ ├── Mobitz Type I (Wenckebach) - AV nodal
│ └── Mobitz Type II - Infranodal
├── High-grade (advanced) AV block
└── Third-degree (complete) AV block
3. SA Node Disorders
Sinus Bradycardia
- Rate < 60 bpm (Braunwald: < 50 bpm is the stricter criterion)
- Normal P-wave morphology, constant PR interval, P:QRS = 1:1
- Often physiologic in athletes, during sleep, with high vagal tone
- Pathologic with hypothyroidism, drugs, ischemia (inferior MI), sick sinus syndrome
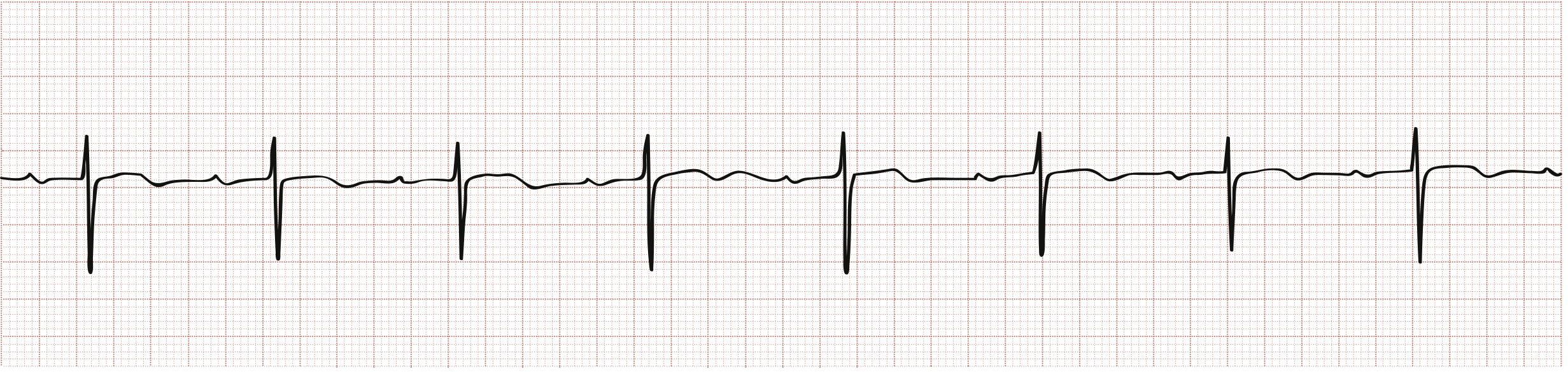
ECG - First-degree AV block (prolonged PR with normal rate pattern):
Sinus Arrest / SA Exit Block
- Sinus arrest: SA node fails to generate impulse → absent P wave, pause not a multiple of P-P interval
- SA exit block: SA fires but impulse blocked before reaching atrium → pause is a multiple of baseline P-P interval (e.g., 2:1, 3:1 block patterns)
- Both can cause escape rhythms if prolonged (junctional or ventricular)
Sick Sinus Syndrome (SSS)
- Group of disorders from disease of SA node and surrounding tissue
- Includes: sinus bradycardia, sinus arrest, SA exit block, chronotropic incompetence
- Most common in older adults (fibrotic degeneration)
- Associated with cardiomyopathies, connective tissue diseases, drugs
Tachy-Brady Syndrome
- Alternating bradyarrhythmia (sinus arrest/pause) and tachyarrhythmia (usually atrial fibrillation)
- The long pause is most evident after AF terminates
- Symptoms include both palpitations (tachycardia phase) and syncope/presyncope (bradycardia phase)
4. AV Conduction Blocks
First-Degree AV Block
| Feature | Details |
|---|---|
| ECG | PR interval > 0.20 s (200 ms); every P followed by QRS |
| QRS | Usually narrow |
| Mechanism | Slowed conduction at AV node (most common), rarely His-Purkinje |
| Significance | Normal variant in up to 2% of healthy young adults; benign |
| Treatment | None; avoid nodal blocking agents |
Second-Degree AV Block
ECG - Wenckebach (Mobitz I): progressively lengthening PR until dropped beat:
| Feature | Mobitz Type I (Wenckebach) | Mobitz Type II |
|---|---|---|
| ECG | Progressive PR lengthening → dropped beat | Constant PR interval → sudden dropped beat without warning |
| QRS | Usually narrow | Usually wide (bundle branch block pattern) |
| Location | AV node | Infranodal (His-Purkinje) |
| Conduction | Decremental (increasing fatigue) | All-or-none (no fatigue) |
| Clinical setting | Inferior MI, digoxin/beta-blocker, high vagal tone, benign | Anteroseptal MI, Lenegre disease, cardiomyopathy - often chronic |
| Response to atropine | Improves | Worsens |
| Response to exercise | Improves | Worsens |
| Prognosis | Generally benign; transient in inferior MI | Worse - precursor to complete heart block |
| Treatment | Usually none; monitor | Pacemaker if severe |
When the ratio is exactly 2:1, type cannot be distinguished without longer strip - a prolonged PR makes Mobitz I more likely; wide QRS makes Mobitz II more likely.
High-Grade / Advanced AV Block
- Two or more consecutive P waves fail to conduct
- Between 2nd and 3rd degree block
- Usually treated as third-degree block
Third-Degree (Complete) AV Block
| Feature | Details |
|---|---|
| ECG | Complete dissociation of P waves and QRS complexes; P rate > QRS rate |
| P waves | Regular at sinus rate (faster) |
| QRS | Regular but independent (escape rhythm); narrow if junctional (40-60 bpm), wide if ventricular (20-40 bpm) |
| PR interval | No consistent relationship - varies randomly |
| Causes | Senescent degeneration, acute ischemia (inferior or anterior MI), Lyme disease, Chagas disease, drugs, congenital |
| Symptoms | Fatigue, syncope (Stokes-Adams attacks), heart failure |
| Treatment | Pacemaker (permanent) - always required if symptomatic |
5. Causes of Bradycardia
Common Medical Causes
| Category | Conditions |
|---|---|
| Physiologic | Athletes, sleep, high vagal tone, young adults |
| Cardiac | Acute inferior MI (SA/AV nodal ischemia via RCA), anterior MI (AV/infranodal block via LAD), myocarditis, cardiomyopathy, post-cardiac surgery/transplant |
| Metabolic | Hypothyroidism, hypothermia, hyperkalemia, hypoxia, hypoglycemia |
| Neurological | Increased intracranial pressure, vagal reflex (vomiting, cough, pain, Valsalva), vasovagal syncope, carotid sinus hypersensitivity, spinal cord injury |
| Infectious | Lyme disease (AV block), Chagas disease, COVID-19, endocarditis |
| Infiltrative | Sarcoidosis, amyloidosis, hemochromatosis |
| Autoimmune | SLE (congenital complete heart block via anti-Ro/La), myocarditis |
Drugs Causing Bradycardia
| Class | Agents |
|---|---|
| Beta-blockers | All, including ophthalmic drops (timolol) |
| Non-DHP calcium channel blockers | Diltiazem, verapamil |
| Antiarrhythmics | Amiodarone, dronedarone, sotalol, flecainide, propafenone |
| Cardiac glycosides | Digoxin |
| Antihypertensives | Clonidine, methyldopa, ivabradine |
| Psychoactive | SSRIs, TCAs, lithium, opioids, phenothiazines, donepezil, phenytoin |
| Anesthetic/other | Propofol, dexmedetomidine, succinylcholine, remdesivir, cannabis |
6. Clinical Features
Symptoms are caused by inadequate cardiac output and cerebral hypoperfusion:
| Symptom | Notes |
|---|---|
| Fatigue, weakness | Most common; often underappreciated |
| Dizziness, presyncope | Particularly with position change |
| Syncope (Stokes-Adams attacks) | Sudden LOC without warning - hallmark of complete AV block or sick sinus; no prodrome unlike vasovagal |
| Palpitations | From escape beats or in tachy-brady syndrome |
| Exercise intolerance | Especially with chronotropic incompetence |
| Worsening heart failure | Reduced cardiac output |
| Cognitive slowing | Particularly in elderly |
| Chest pain | If bradycardia causing demand ischemia |
7. Evaluation
Initial Assessment
- 12-lead ECG - identify the rhythm, P:QRS relationship, PR interval, QRS width
- Vital signs - BP, SpO2, signs of hemodynamic compromise
- History - medications, symptoms, exertion, syncope, prior cardiac history
- Labs - TSH, electrolytes (K+, Ca2+, Mg2+), digoxin level, blood glucose, Lyme serology if indicated
Further Workup (Outpatient / Stable)
- Echocardiogram - structural heart disease, cardiomyopathy, infiltrative disease (Class IIa)
- Ambulatory ECG monitoring - Holter (24-48 h), extended event recorder (up to 30 days), implantable loop recorder (up to 3 years) for infrequent/unexplained syncope
- Exercise stress test - chronotropic incompetence, exertion-related symptoms (Class IIa)
- Cardiac MRI - suspected sarcoid, amyloid, myocarditis (Class IIa)
- Electrophysiology study (EPS) - limited role for SND; more useful for unexplained syncope, suspected infranodal block (Class IIb)
8. Management
Acute Symptomatic Bradycardia (ACLS Approach)
First assess: Is the patient hemodynamically unstable?
- Hypotension, altered consciousness, chest pain, signs of shock, acute heart failure
Step 1 - Atropine (First-Line)
| Parameter | Details |
|---|---|
| Dose | 0.5-1 mg IV bolus, repeat every 3-5 min to max 3 mg |
| Mechanism | Blocks muscarinic vagal tone at SA and AV nodes |
| Works for | Sinus bradycardia, Mobitz I, vagally-mediated bradycardia |
| Does NOT work well for | Mobitz II, complete AV block (infranodal - no vagal innervation below AV node) |
| Avoid in | Acute ischemia/MI (can worsen ischemia by increasing HR); infranodal blocks |
| Ineffective in | Post-cardiac transplant (denervated heart) |
Step 2 - If Atropine Fails / Infranodal Block
| Treatment | Dose | Notes |
|---|---|---|
| Transcutaneous pacing | Rate 60-80 bpm | Immediate bridge; uncomfortable - sedate if possible |
| Dopamine infusion | 5-20 mcg/kg/min IV | Chronotropic + vasopressor effect |
| Epinephrine infusion | 2-10 mcg/min IV | Alternative to dopamine |
| Isoproterenol | 2-10 mcg/min IV | Post-transplant bradycardia (beta-1 agonist, bypasses vagal block) |
| Glucagon | 1-5 mg IV then 5-15 mcg/min infusion | Beta-blocker or CCB overdose (bypasses blocked receptors via cAMP) |
| Transvenous temporary pacing | Rate 60-80 bpm | Definitive bridge for unstable patients |
Step 3 - Treat Reversible Causes
- Stop/reduce offending drugs
- Treat acute MI (reperfusion), hypothyroidism, hyperkalemia, Lyme disease, hypoxia
- Correct electrolytes
Chronic Management - Pacemaker Indications
Sinus Node Dysfunction
| Class | Indication |
|---|---|
| I - Indicated | Symptomatic bradycardia or syncope directly attributable to SND |
| I - Indicated | Symptomatic bradycardia from necessary guideline-directed drug therapy (no alternative) |
| IIa - Reasonable | Symptomatic tachy-brady syndrome |
| IIa - Reasonable | Symptomatic chronotropic incompetence |
| IIb - May consider | Uncertain symptom-rhythm correlation; trial of theophylline first |
| III - Harmful | Asymptomatic sinus bradycardia |
AV Block
| Arrhythmia | Pacemaker Need | Notes |
|---|---|---|
| First-degree AV block | None | Benign; monitor |
| Mobitz I (Wenckebach) | None usually | Treat underlying cause; pacemaker if severely symptomatic |
| Mobitz II | Yes (if significant) | Can progress to complete block; pacemaker strongly considered |
| High-grade AV block | Yes | Treat as complete block |
| Third-degree (complete) | Yes - almost always | Permanent pacemaker; temporary pacing as bridge |
Pacing Mode Selection (ACC/AHA/HRS 2018)
| Situation | Preferred Mode |
|---|---|
| SND with intact AV conduction | AAI (single-chamber atrial) |
| SND with uncertain AV conduction | DDD (dual-chamber) |
| AV block with intact sinus function | DDD (dual-chamber) |
| Significant comorbidities, infrequent pacing expected | VVI (single-chamber ventricular) acceptable |
| DDD + intact AV conduction | Program to minimize RV pacing |
Atrial-based pacing is preferred over single-chamber ventricular pacing - reduces AF incidence, pacemaker syndrome, and heart failure.
9. Summary Table - Quick Reference
| Rhythm | ECG Key Feature | Clinical Risk | Treatment |
|---|---|---|---|
| Sinus bradycardia | Normal P, rate < 60 | Low if asymptomatic | Observe; atropine if symptomatic |
| Sinus arrest | Absent P, pause not multiple of P-P | Moderate | Treat cause; PPM if recurrent |
| First-degree AV block | PR > 200 ms, all P conducted | None | No treatment |
| Mobitz I (Wenckebach) | PR lengthens → dropped beat | Low | Observe; treat cause |
| Mobitz II | Constant PR → sudden dropped beat | High - risk of complete block | PPM; atropine ineffective |
| Complete (3rd degree) AV block | P and QRS dissociated | High - syncope, death | Temporary then permanent pacemaker |
| Sick sinus syndrome | Variable - brady ± tachy | Moderate-high | PPM; treat tachyarrhythmia |
| Tachy-brady syndrome | AF/SVT alternating with sinus pause | Moderate-high | PPM + antiarrhythmic or ablation |
Sources:
- ROSEN's Emergency Medicine, Chapter 65 (Dysrhythmias)
- Braunwald's Heart Disease 2 Vol Set, Chapter 68 (Bradyarrhythmias)
- Goldman-Cecil Medicine, Chapter 51, Table 49-8
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 251 (Fig. 251-3)
- Fuster and Hurst's The Heart 15E, Chapter 38 (ACC/AHA/HRS 2018 Guideline algorithms)
- Miller's Anesthesia 10E, Chapter 32 (ACLS bradycardia)
Can hypotension cause bradycardia
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
I now have rich physiological content from multiple authoritative sources. Let me compile the complete, authoritative answer.
Can Hypotension Cause Bradycardia?
Short answer: Yes - but it is the paradoxical, physiologically counterintuitive response. Normally, hypotension triggers reflex tachycardia via baroreceptors. However, several specific mechanisms can produce hypotension simultaneously with or causing bradycardia - the combination is a well-recognized and clinically important pattern.
The Normal Response to Hypotension: Reflex Tachycardia
Under normal physiology, a fall in blood pressure is detected by arterial baroreceptors (carotid sinus, aortic arch). The reflex response is:
Hypotension → ↓ baroreceptor firing → ↑ sympathetic outflow + ↓ parasympathetic tone → tachycardia + vasoconstriction → restored BP
This is the expected compensatory response - seen in hemorrhage, dehydration, sepsis, and most causes of hypotension.
Mechanisms Where Hypotension Co-exists With (or Causes) Bradycardia
1. Vasovagal (Neurocardiogenic) Syncope - Most Common
This is the classic paradoxical bradycardia-with-hypotension scenario.
Mechanism (Ganong's Physiology):
- Prolonged upright posture or emotional trigger → blood pools in lower extremities → ↓ venous return → ↓ intracardiac volume
- Arterial baroreceptors sense the fall in BP and appropriately trigger sympathetic activation (tachycardia, increased contractility)
- However, mechanoreceptors (stretch receptors) in the wall of the left ventricle respond to the underfilled, vigorously contracting ventricle by sending paradoxical signals via unmyelinated vagal C fibers
- This triggers a paradoxical surge in parasympathetic tone → bradycardia + vasodilation + hypotension
- The individual becomes lightheaded and may lose consciousness
Two subtypes:
- Cardioinhibitory: predominant bradycardia (HR drops sharply, even to asystole briefly)
- Vasodepressor: predominant vasodilation/hypotension with little bradycardia
- Mixed: both occur together (most common)
"Pressure receptors in the wall of the left ventricle respond by sending signals that trigger paradoxical bradycardia and decreased contractility, resulting in sudden marked hypotension." - Ganong's Review of Medical Physiology
2. Bezold-Jarisch Reflex - A Core Physiology Mechanism
This reflex directly produces the triad of hypotension + bradycardia + coronary vasodilation in response to noxious ventricular stimuli.
Mechanism (Miller's Anesthesia / Ganong's):
- Trigger: Chemoreceptors and mechanoreceptors in the left ventricular wall sense noxious stimuli (ischemia, reperfusion, chemical irritants, ventricular underfilling)
- Receptor type: 5-HT3 (serotonin) receptors on unmyelinated vagal C fibers
- Pathway: Afferent signal travels via vagal C fibers → brainstem → ↑ efferent parasympathetic output
- Result: Bradycardia + hypotension + coronary artery dilation
Clinical situations where Bezold-Jarisch reflex activates:
| Trigger | Setting |
|---|---|
| Myocardial ischemia / reperfusion | During acute MI (especially inferior), post-thrombolysis |
| Radiocontrast agents | During coronary angiography |
| Spinal / neuraxial anesthesia | Hypotension after spinal block → reflex bradycardia worsens hypotension |
| Severe ventricular underfilling | Hypovolemia, hemorrhage (paradoxical) |
| Serotonin-releasing stimuli | Chemical exposures, capsaicin |
"The Bezold–Jarisch reflex responds to noxious ventricular stimuli... by inducing the triad of hypotension, bradycardia, and coronary artery dilatation." - Miller's Anesthesia 10E
"Activation of 5-HT3 receptors... in response to systemic hypotension increases efferent vagal signaling, producing bradycardia, reduced cardiac output, and worsened hypotension." - Barash Clinical Anesthesia
Note the critical clinical implication: hypotension triggers the reflex → bradycardia → further ↓ cardiac output → worse hypotension - a vicious cycle.
3. Cushing Reflex (Neurogenic - Raised ICP)
The Cushing reflex occurs with increased intracranial pressure (ICP) causing brainstem ischemia. This produces hypertension (not hypotension) + bradycardia + irregular respirations - so the hemodynamic context here is actually raised BP, not low BP. However, it is listed because hypotension in the context of brain injury can trigger it if ICP surpasses MAP.
4. Inferior / Right Ventricular Myocardial Infarction
- RCA occlusion causes ischemia of the SA node (60% supplied by RCA) and AV node (85-90% supplied by RCA)
- Simultaneously, the Bezold-Jarisch reflex is activated by ischemic ventricular receptors
- Result: Bradycardia (sinus or AV block) + hypotension (from RV failure and reduced preload)
- Atropine is used for the bradycardia; IV fluids are critical for RV infarct hypotension
- This is one of the most clinically important hypotension-bradycardia combinations
5. Neuraxial (Spinal/Epidural) Anesthesia
- Sympathetic blockade → vasodilation → hypotension
- Reduced venous return → ventricular underfilling → Bezold-Jarisch reflex → bradycardia
- Can be severe; treated with atropine, ephedrine, or phenylephrine
- Ondansetron (5-HT3 antagonist) may reduce the risk by blocking the reflex receptor
6. Carotid Sinus Hypersensitivity
- Pressure on the carotid sinus (tight collar, head turning) → exaggerated baroreceptor firing → paradoxical ↑ vagal tone → bradycardia + hypotension
- Cardioinhibitory type: primarily bradycardia
- Vasodepressor type: primarily hypotension
7. Drugs
Some drugs produce both hypotension AND bradycardia simultaneously by dual mechanisms:
| Drug | Mechanism |
|---|---|
| Beta-blockers | ↓ HR (chronotropy) + ↓ CO → hypotension |
| Non-DHP calcium channel blockers (verapamil, diltiazem) | ↓ HR + vasodilation → hypotension |
| Digoxin toxicity | Vagal activation → bradycardia/AV block + low CO |
| Clonidine / dexmedetomidine | Central α2 agonist → ↓ sympathetic tone → both bradycardia + hypotension |
| Propofol | Vasodilation + impairs baroreceptor reflex → hypotension; may trigger Bezold-Jarisch bradycardia |
| Opioids | Vagotonia + vasodilation |
Summary: When Do You See Hypotension + Bradycardia Together?
| Mechanism | Example |
|---|---|
| Bezold-Jarisch reflex | Inferior MI, spinal anesthesia, severe hypovolemia |
| Vasovagal syncope | Prolonged standing, pain, emotional stress |
| Carotid sinus hypersensitivity | Pressure on neck |
| Drug effects | Beta-blockers, verapamil, clonidine, propofol overdose |
| Acute inferior MI | SA/AV nodal ischemia + RV failure |
| Tension pneumothorax | Obstructive shock → ↓ venous return → Bezold-Jarisch |
| Anaphylaxis | Hypotension dominant; bradycardia can occur if Bezold-Jarisch activated |
Clinical Importance
- Hypotension + bradycardia is a dangerous combination because both reduce cardiac output simultaneously (CO = HR × SV)
- In hemorrhagic shock, paradoxical bradycardia signals decompensation - a very ominous sign
- Do not give atropine alone for bradycardia in the context of inferior MI with hypotension - you must also treat the RV infarct and ischemia
- In spinal anesthesia, treating the hypotension (with phenylephrine or fluids) often breaks the Bezold-Jarisch cycle and resolves the bradycardia simultaneously
Sources:
- Ganong's Review of Medical Physiology 26E, Chapter 32 (Bezold-Jarisch Reflex, Vasovagal Syncope)
- Miller's Anesthesia 10E, Chapter 4 (Bezold-Jarisch Reflex)
- Barash Clinical Anesthesia 9E, Chapter 35 (Neuraxial anesthesia bradycardia)
- Morgan & Mikhail's Clinical Anesthesiology 7E
- Katzung Basic & Clinical Pharmacology 16E (5-HT3 receptor-mediated Bezold-Jarisch)
This is a shared conversation. Sign in to Orris to start your own chat.