What is Gullain barre syndrome
Reading File
Finding Sources
Searching PubMed
"Guillain-Barre syndrome"[MeSH Terms]
Reading File
Reading File
Reading File
Searching Images
Guillain-Barre syndrome ascending paralysis pathology nerve demyelination
I have comprehensive textbook data and images. Here is a thorough answer:
Guillain-Barré Syndrome (GBS)
Definition
Guillain-Barré syndrome is an acute, immune-mediated polyneuropathy of the peripheral nervous system characterized by rapidly progressive ascending motor weakness, areflexia, and — in its classic form — multifocal inflammatory demyelination of spinal roots and peripheral nerves. It is one of the most common life-threatening peripheral nervous system disorders, with an incidence of 0.81–1.89 cases per 100,000 per year worldwide. — Miller's Anesthesia, 10e
Historical Background
First described in 1916 by Guillain, Barré, and Strohl, who emphasized the triad of motor weakness, areflexia, and albuminocytological dissociation in the CSF (elevated protein without pleocytosis). Before the era of positive-pressure ventilation, mortality was ~33%; it has since fallen to 1–5%. — Bradley and Daroff's Neurology in Clinical Practice
Pathophysiology
About two-thirds of GBS cases are triggered by a preceding infection (typically 1–3 weeks prior). The infection provokes microbe-specific T cells and antibodies that cross-react with gangliosides and glycolipids on peripheral nerve sheaths — a process of molecular mimicry.
- Both T-cell-mediated and antibody-mediated mechanisms are involved; T cells are believed to play the dominant role.
- Injury is most extensive in nerve roots and proximal nerve segments.
- Mononuclear infiltrates rich in macrophages cause demyelination (and in axonal subtypes, direct axonal damage).
Common triggers:
| Infectious | Non-Infectious |
|---|---|
| Campylobacter jejuni (most common) | Vaccinations |
| Epstein-Barr virus | Immune checkpoint inhibitors |
| Cytomegalovirus | Surgery |
| HIV | |
| Zika virus, Chikungunya | |
| SARS-CoV-2 |
— Robbins & Kumar Basic Pathology; Miller's Anesthesia, 10e
Subtypes and Variants
| Subtype | Key Features |
|---|---|
| AIDP (Acute Inflammatory Demyelinating Polyneuropathy) | Most common in Europe/North America; demyelinating |
| AMAN (Acute Motor Axonal Neuropathy) | Motor only; associated with C. jejuni; anti-GM1/GD1a antibodies; common in northern China |
| AMSAN (Acute Motor-Sensory Axonal Neuropathy) | Motor + sensory axonal; severe, poor recovery |
| Miller-Fisher Syndrome (MFS) | Triad of ophthalmoplegia, ataxia, areflexia; anti-GQ1b antibodies; 6% of GBS in the West, up to 18% in Taiwan |
| Pharyngeal-cervical-brachial variant | Bulbar + upper limb weakness |
| Facial diplegia with paresthesias | Bilateral facial palsy |
| Paraparetic variant | Lower limb predominance |
— Bradley and Daroff's Neurology in Clinical Practice
Clinical Features
Required for diagnosis:
- Progressive weakness of both legs and arms
- Areflexia or hyporeflexia
Supportive features:
- Progression over days to 4 weeks, then plateau
- Relative symmetry of deficits
- Mild sensory symptoms
- Bifacial palsies
- Autonomic dysfunction (dysautonomia in up to 20% — arrhythmias, BP swings, urinary retention)
- Absence of fever at onset
- Recovery begins 2–4 weeks after progression ceases
Respiratory involvement:
- Respiratory failure occurs in 20–30% of cases — a major reason for ICU admission.
- Mortality rises to 14.3% when mechanical ventilation is required.
- In ~5% of patients, maximal deficit is reached within 72 hours.
— Bradley and Daroff's; Miller's Anesthesia, 10e
Diagnosis
| Investigation | Finding in GBS |
|---|---|
| CSF | Elevated protein, <10 cells/μL (albuminocytological dissociation) |
| Nerve conduction studies / EMG | Slowed conduction velocity, conduction block (demyelinating); reduced amplitudes (axonal) |
| MRI spine (with contrast) | Enhancement of cauda equina / nerve roots |
| Serology | Anti-GQ1b (MFS), anti-GM1 (AMAN), C. jejuni serology |
| ECG | Arrhythmias from autonomic instability |
Axonal degeneration on NCS and anti-GM1 antibody positivity are associated with worse prognosis. — Miller's Anesthesia, 10e
MRI Images in GBS
Below is an MRI of the lumbar spine in GBS showing enhancement of nerve roots of the cauda equina — a classic radiological hallmark of the blood-nerve barrier breakdown in AIDP:
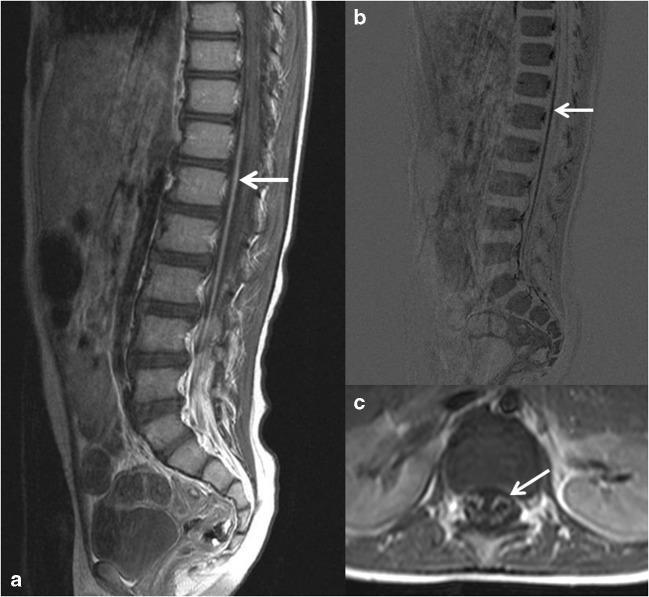
Contrast-enhanced T1 MRI showing anterior motor nerve root enhancement in GBS. Panel (c) highlights isolated ventral root involvement.
Respiratory Monitoring (ICU Thresholds)
The "20-15-12 rule" guides ICU admission and intubation decisions:
- Forced vital capacity (FVC) < 20 mL/kg → close monitoring
- FVC < 15 mL/kg → probable intubation
- Maximal inspiratory pressure (MIP) < −30 cmH₂O → respiratory compromise
- Hypercarbia is a late sign — do not wait for it.
The EGRIS score (Erasmus GBS Respiratory Insufficiency Score) is a validated tool for predicting ICU need based on severity of weakness, timing, and bulbar symptoms. — Miller's Anesthesia, 10e
Treatment
| Treatment | Mechanism |
|---|---|
| IV Immunoglobulin (IVIg) | Suppresses immune responses (mechanism not fully understood) |
| Plasmapheresis (plasma exchange) | Removes offending antibodies from circulation |
| Supportive care | Ventilatory support, DVT prophylaxis, pain management, autonomic monitoring |
| Corticosteroids | Not effective in GBS (do not use) |
Both IVIg and plasmapheresis are equally effective; they are not additive when combined. Early tracheostomy is appropriate when prolonged respiratory failure is anticipated. — Robbins & Kumar; Miller's Anesthesia, 10e
Prognosis
- Most patients begin recovering 2–4 weeks after disease nadir.
- Recovery can take months to years depending on axonal injury severity.
- ~20% of patients have significant residual disability at 6 months.
- AMAN and AMSAN subtypes carry poorer prognosis.
Comparison: GBS vs CIDP
| Feature | GBS | CIDP |
|---|---|---|
| Onset | Acute (days–4 weeks) | Subacute–chronic (>2 months) |
| Course | Monophasic | Relapsing-remitting or progressive |
| CSF protein | Elevated | Elevated |
| Treatment | IVIg or plasmapheresis | IVIg, steroids, plasmapheresis |
— Robbins & Kumar Basic Pathology
Sources: Bradley and Daroff's Neurology in Clinical Practice | Robbins & Kumar Basic Pathology | Miller's Anesthesia, 10e
This is a shared conversation. Sign in to Orris to start your own chat.