what is aponeuroses of muscles
aponeurosis of muscles anatomy definition function
Aponeuroses of Muscles
Definition
- Mulholland & Greenfield's Surgery, p. 3634: "An aponeurosis is defined as the non-muscle-fiber-containing portion of a muscle usually present at insertion points. Muscle fibers are said to 'give way' to the corresponding aponeurosis."
Structure
- Made of tightly packed, parallel collagen fibers arranged in multiple layers (the fiber directions alternate between layers, giving it tensile strength in multiple directions).
- Glistening white in appearance, tough and inextensible.
- Similar in composition to a tendon but shaped as a sheet rather than a cord.
- Distinct from fascia - fascia is fibrous tissue that lines or envelops muscles, whereas an aponeurosis is the functional insertion/origin of a muscle.
Functions
| Function | Explanation |
|---|---|
| Muscle attachment | Connects muscle to bone, cartilage, or another muscle |
| Force transmission | Transmits the pull of muscle fibers over a wide area |
| Energy absorption | Acts like a spring, absorbing mechanical energy during movement |
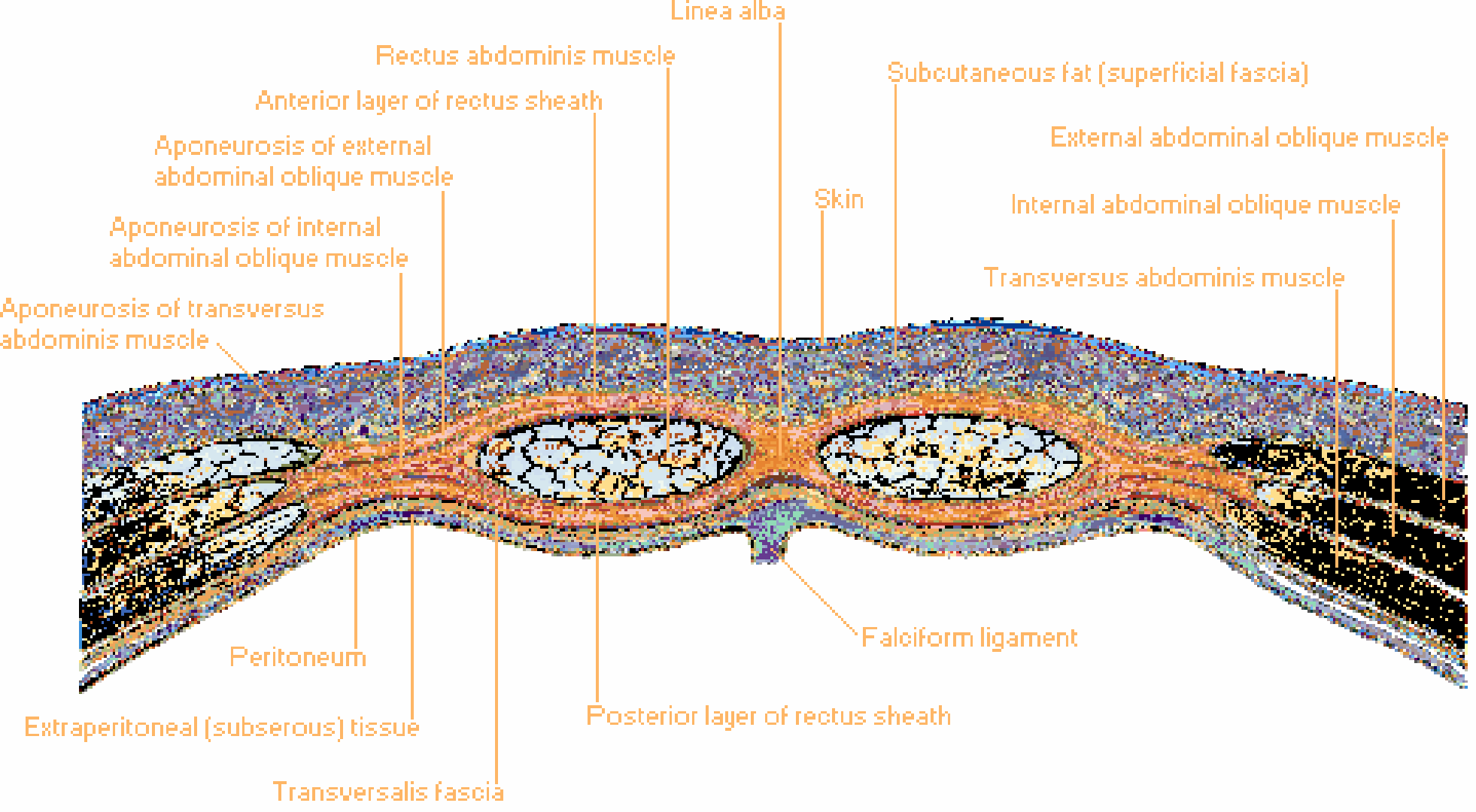
| Structural support | Forms protective sheaths around muscles (e.g., rectus sheath) |
| Ligament formation | Some aponeuroses fold on themselves to form ligaments (e.g., the inguinal ligament from the external oblique aponeurosis) |
Key Examples in the Body
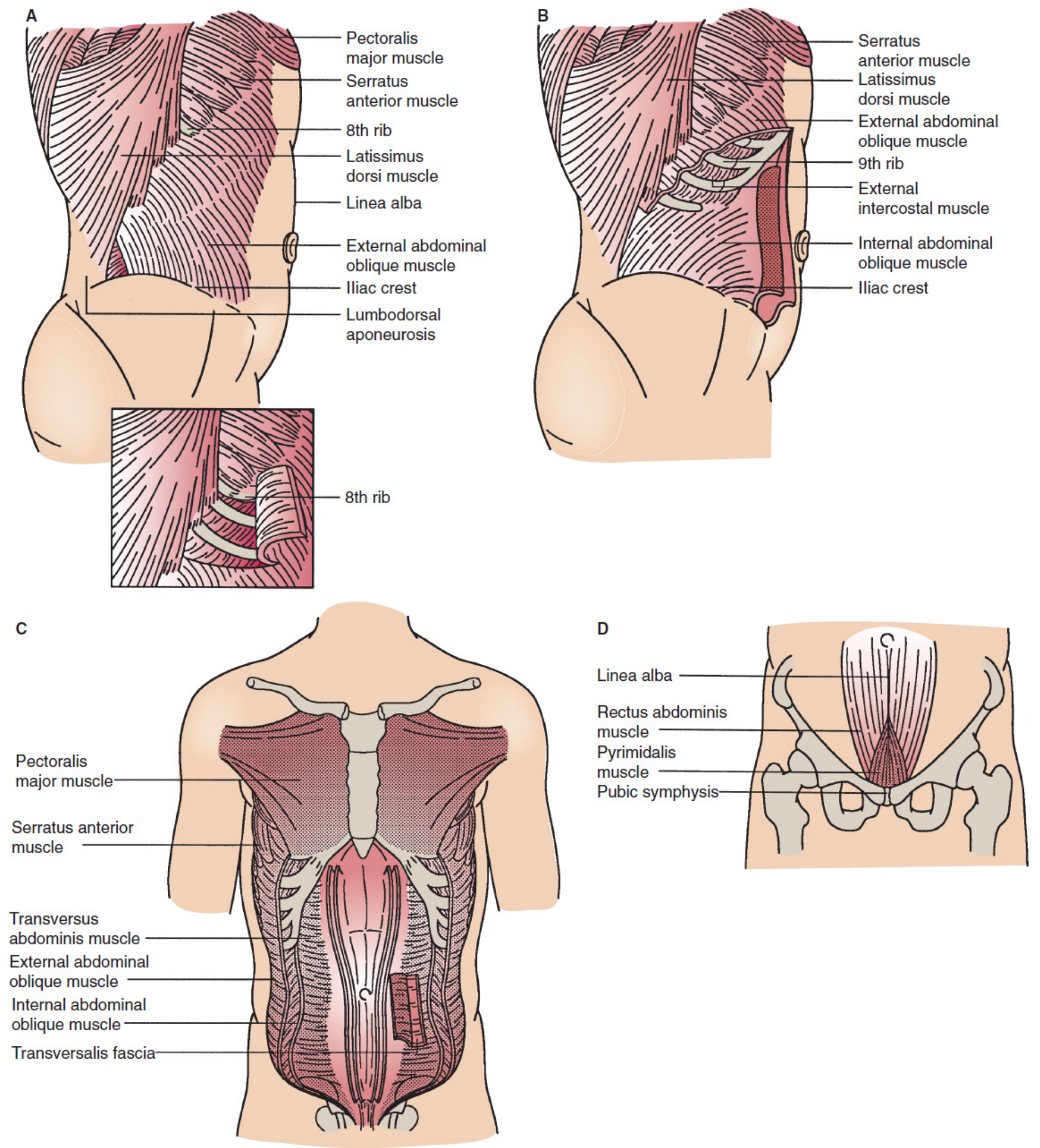
- External oblique aponeurosis - contributes to the anterior layer of the rectus sheath; its folded lower edge forms the inguinal ligament.
- Internal oblique aponeurosis - splits to form both the anterior and posterior layers of the rectus sheath above the arcuate line.
- Transversus abdominis aponeurosis - merges with the posterior rectus sheath above the arcuate line.
- Located in the palm of the hand, deep to the skin.
- Triangular sheet of dense connective tissue, continuous with the palmaris longus tendon proximally and dividing into four bands distally toward the fingers.
- Protects the underlying tendons, vessels, and nerves of the palm.
- Thick, strong band on the sole of the foot.
- Originates from the calcaneus (heel bone) and fans out to the toes.
- Supports the longitudinal arch of the foot and absorbs impact during walking/running.
- Inflammation of this structure causes the common condition "plantar fasciitis."
- Sheet of fibrous tissue on the top of the skull, connecting the frontalis muscle (forehead) anteriorly to the occipitalis muscle posteriorly.
- Allows the scalp to move over the skull.
- Fan-shaped sheet from the biceps tendon that spreads medially over the forearm flexors.
- Protects the brachial artery and median nerve passing beneath it.
- The distal part of the levator palpebrae superioris muscle flattens into an aponeurosis that inserts into the upper eyelid tarsal plate - responsible for lifting the upper eyelid.
Aponeurosis vs. Tendon vs. Fascia
| Feature | Aponeurosis | Tendon | Fascia |
|---|---|---|---|
| Shape | Flat, sheet-like | Cord-like | Sheet, wraps structures |
| Function | Muscle attachment (broad) | Muscle attachment (focal) | Envelops, separates muscles |
| Collagen arrangement | Multi-directional layers | Parallel bundles | Irregular |
| Example | Linea alba | Achilles tendon | Thoracolumbar fascia |
Clinical Relevance
- Hernias - Weaknesses or tears in abdominal aponeuroses allow viscera to protrude (inguinal, umbilical, incisional hernias). Hernia repair surgery relies heavily on the strength of aponeurotic tissue to hold sutures.
- Plantar fasciitis - Overuse injury to the plantar aponeurosis causing heel pain.
- Dupuytren's contracture - Fibrosis and contraction of the palmar aponeurosis causing fingers to curl.
- Ptosis - Dehiscence (separation) or disinsertion of the levator aponeurosis is a leading cause of drooping eyelid.
Selective vasoconstriction of the efferent arteriole (up to certain extent) increases hydrostatic pressure in the glomerular capillaries, and therefore increases the glomerular filtration rate. As efferent arteriolar constriction continues to increase, the glomerular filtration rate begins to decrease due to a flow-mediated rise in oncotic pressure in the glomerular capillaries. The filtration fraction always increases with increasing efferent arteriole constriction. this i want as small notes
Efferent Arteriole Constriction & GFR
🔹 Phase 1 — Mild to Moderate Constriction
- Efferent arteriole constriction raises resistance to outflow from the glomerulus
- Blood is "dammed back" → glomerular capillary hydrostatic pressure (P
GC) rises - Higher P
GCdrives more filtration → GFR increases
🔹 Phase 2 — Severe / Progressive Constriction
- Blood flow through the glomerulus becomes markedly reduced
- More water and small solutes are filtered per unit of plasma → plasma proteins become concentrated
- Oncotic pressure (π
GC) rises significantly — this opposes filtration - The rise in oncotic pressure overcomes the benefit of raised hydrostatic pressure
- Net filtration pressure falls → GFR decreases
🔹 Filtration Fraction (FF) — Always Increases
- Renal plasma flow (RPF) falls with increasing efferent constriction (reduced overall flow)
- Even when GFR eventually falls, RPF falls faster and proportionally more
- Therefore, FF always increases with progressive efferent arteriole constriction
🔹 Summary Table
| Degree of Efferent Constriction | P | Oncotic Pressure | GFR | RPF | FF |
|---|---|---|---|---|---|
| Mild | ↑ | Slight ↑ | ↑ | ↓ | ↑ |
| Severe | ↑ (plateau) | ↑↑ | ↓ | ↓↓ | ↑↑ |
🔹 Key Concept in One Line
Efferent constriction is a "double-edged" mechanism — it first raises GFR by increasing hydrostatic pressure, then lowers GFR by raising oncotic pressure, but filtration fraction rises throughout.
I don't have time to make big, big notes. I want like just a single point engine note that I can remember it and solve questions.
Efferent Arteriole Constriction
- Mild → ↑P
GC→ ↑GFR - Severe → ↑↑oncotic pressure → ↓GFR
- FF always ↑ (RPF drops faster than GFR)
What is it you are cutting at PGE, socelanding increases is what you cut it.