Filters used in cpb detailed notes
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here are detailed notes on Filters Used in Cardiopulmonary Bypass (CPB):
Filters Used in Cardiopulmonary Bypass (CPB)
Overview
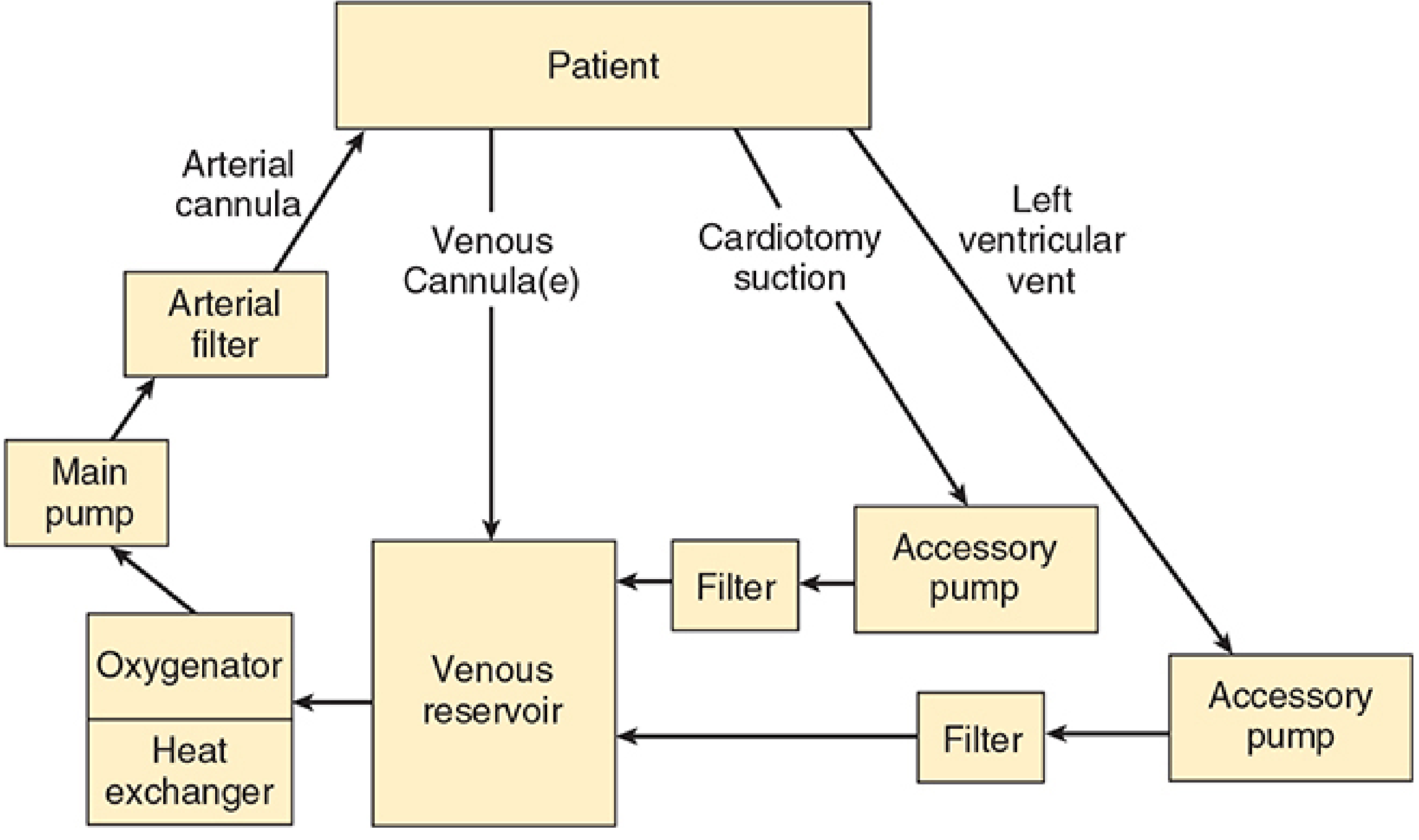
The CPB circuit contains multiple filters at different points. The six basic components of the CPB machine are: venous reservoir, oxygenator, heat exchanger, main pump, arterial filter, and connecting tubing. In addition, accessory pumps use separate inline filters before blood returns to the reservoir. A number of other filters, alarms, and in-line monitors are also typically incorporated.
1. Arterial Line Filter (Main Filter)
Location: Final inline filter, placed AFTER the main pump and BEFORE the arterial cannula (aortic return)
Pore size: Passes only particles smaller than 27-40 μm - traps everything larger
Purpose:
- Removes particulate matter - thrombi, fat globules, tissue debris that may enter via cardiotomy suction
- Traps gas bubbles (air microemboli) - has a built-in stopcock to vent these out
- Provides the last line of defense against systemic embolism before blood returns to the patient
Design features:
- Always arranged in parallel with a normally clamped bypass limb - if the filter clogs, the bypass limb can be opened to maintain perfusion
- Has a built-in stopcock to bleed off trapped gas bubbles
- Arterial inflow pressure is measured proximal to the filter (before it) so that clogging can be detected; the pressure difference across the filter reflects filter resistance
Clinical significance:
- The pressure drop across the arterial filter + arterial tubing + aortic cannula = the measured inflow pressure. Monitoring this is important for detecting problems with the arterial inflow line.
- Inflow pressures should be watched continuously for sudden rises indicating filter obstruction
(Source: Morgan & Mikhail's Clinical Anesthesiology, 7e; Barash Clinical Anesthesia, 9e)
2. Cardiotomy/Accessory Pump Filters
Location: Inline on the return lines from accessory pumps (cardiotomy suction pump and LV vent pump), positioned BEFORE blood re-enters the venous reservoir
Purpose:
- The cardiotomy suction pump aspirates blood from the surgical field and returns it to the main reservoir. This line is a portal for fat, tissue debris, thrombi, and bone fragments entering the circuit
- The filter catches this debris before it reaches the reservoir and potentially the patient
- The LV vent filter similarly screens blood drained from the left ventricle
Clinical note: This is the main reason cardiotomy suction is considered a major source of embolic and inflammatory burden - even with filtration, fat microemboli and activated inflammatory mediators can pass through.
(Source: Morgan & Mikhail's Clinical Anesthesiology, 7e - see circuit diagram above)
3. Heat Exchanger Bubble Trap / Filter
Location: Built into the heat exchanger unit (which is downstream of the oxygenator)
Purpose:
- Gas solubility decreases as blood temperature rises during rewarming
- Dissolved gas comes out of solution and forms bubbles during the rewarming phase
- A filter/trap built into the heat exchanger unit catches these bubbles before they enter the main circuit
Key point: This is especially relevant during the rewarming phase at the end of CPB when bubble formation risk is highest.
(Source: Morgan & Mikhail's Clinical Anesthesiology, 7e)
4. Leukocyte Depletion Filter (LDF)
Location: Inline in the CPB circuit (position varies - can be on the arterial line or on cardioplegia delivery lines)
Purpose:
- Selectively removes activated leukocytes from circulating blood
- Aims to reduce the systemic inflammatory response triggered by CPB (contact of blood with foreign surfaces activates complement, leukocytes, platelets, coagulation cascade)
- Leukocyte-depleted blood cardioplegia has been shown to improve myocardial preservation in some studies
- Hemofiltration (ultrafiltration) during CPB, which removes inflammatory cytokines, appears beneficial particularly in pediatric patients
Evidence:
- A review of 63 studies (Warren et al.) concluded leukocyte filtration may have some modest benefits, but definitive evidence of improvement in inflammatory-mediated complications is insufficient
- Leukocyte depletion reduces inflammation and may reduce complications, but the evidence for routine use remains weak
(Source: Morgan & Mikhail's Clinical Anesthesiology, 7e; Miller's Anesthesia, 10e)
5. Micropore / Screen Filter (Blood Transfusion Context)
Pore size: Most investigators recommend 40 μm pore size - this minimizes microembolization without causing excessive elevation in filtration pressure
Purpose:
- Used when salvaged blood or bank blood is returned during or after CPB
- Reduces risk of microembolization from microaggregates that form in stored blood (platelets, fibrin, leukocyte aggregates)
Evidence: A pore size of 40 μm is most widely supported - pore sizes from 20-170 μm have been studied; 40 μm strikes the best balance between filtration efficiency and maintaining flow without excess pressure drop.
(Source: Roberts & Hedges' Clinical Procedures in Emergency Medicine)
Summary Table
| Filter | Location | Pore Size | Primary Function |
|---|---|---|---|
| Arterial line filter | Post-pump, pre-aortic cannula | 27-40 μm | Remove particulates + trap gas emboli |
| Cardiotomy/vent filter | Post-accessory pump, pre-reservoir | Variable | Remove debris from surgical field blood |
| Heat exchanger bubble trap | Within heat exchanger unit | Gas trap | Catch bubbles formed during rewarming |
| Leukocyte depletion filter | Inline arterial or cardioplegia line | Selective | Remove activated leukocytes, reduce inflammation |
| Micropore filter | On blood salvage/transfusion return | 40 μm (recommended) | Remove microaggregates from stored/salvaged blood |
Key Clinical Points
- Arterial filter = most important filter in the standard CPB circuit - mandatory component, protects against both particulate and gaseous emboli
- Bypass limb is always present in parallel with the arterial filter - can be opened if filter clogs
- Pressure monitoring proximal to the arterial filter detects clogging early
- Cardiotomy suction is the biggest source of debris - its filter is important but not perfect (fat and activated cells still pass)
- Leukocyte filters address the inflammatory response to CPB - benefit is real but modest; not universally used
- Bubble traps in the heat exchanger are passive safety features for the rewarming phase
- In pediatric CPB, hemofiltration (ultrafiltration) as a filtering strategy to remove cytokines and excess fluid has stronger evidence than in adults
This is a shared conversation. Sign in to Orris to start your own chat.