Define synapse, properties of synapse.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the information needed for a thorough answer. Here is a complete, well-organized response drawn from Guyton & Hall, Costanzo Physiology, Medical Physiology (Boron & Boulpaep), and Neuroscience: Exploring the Brain.
Synapse - Definition and Properties
Definition
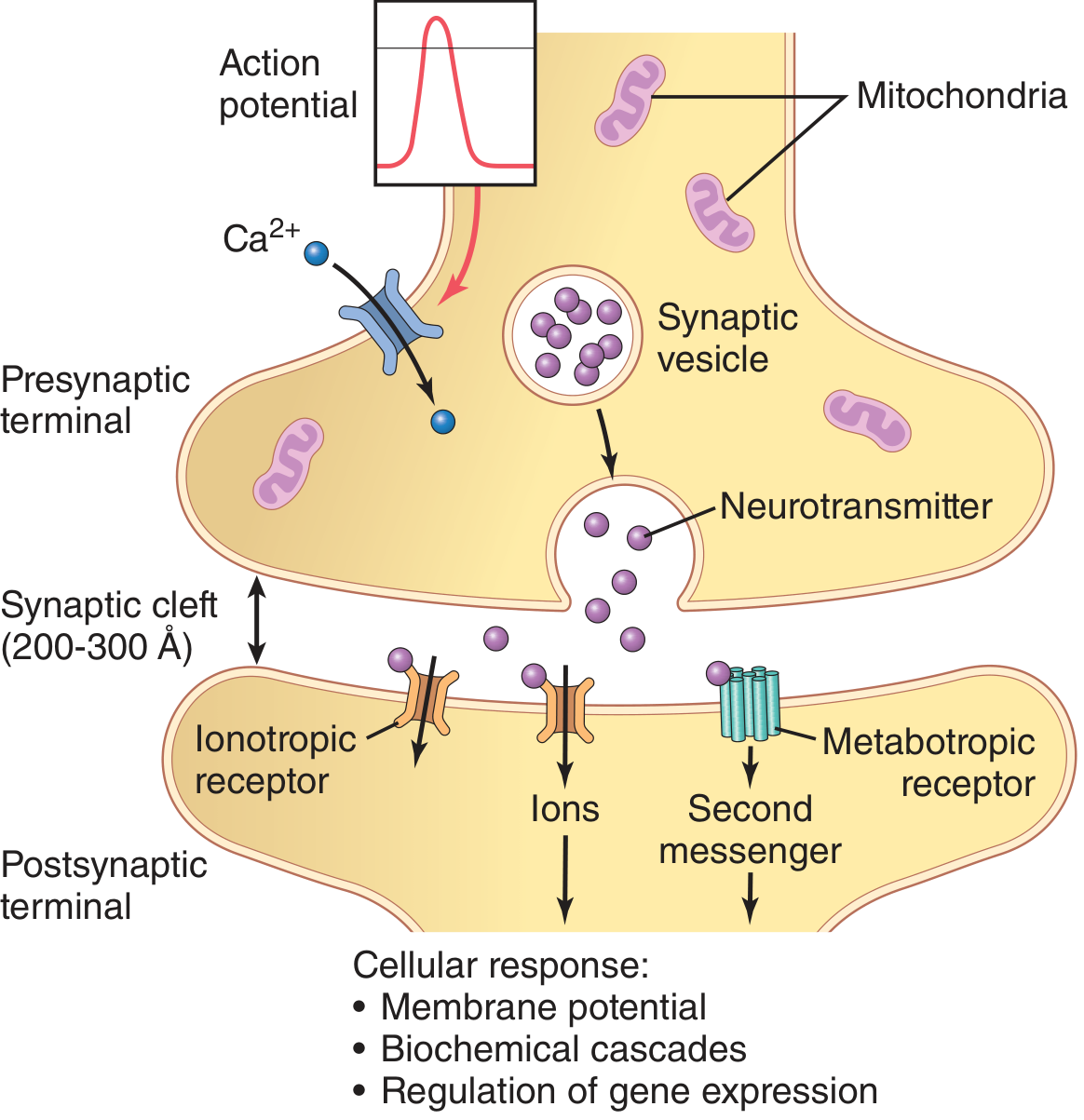
A synapse is the specialized junction between two neurons (or between a neuron and an effector cell such as a muscle or gland) through which information is transmitted from one cell to another. The term was coined by Charles Sherrington from the Greek word meaning "to clasp."
The synapse has two functional sides:
- Presynaptic side - usually the axon terminal of the transmitting neuron
- Postsynaptic side - usually a dendrite, soma (cell body), or occasionally another axon of the receiving neuron
- Synaptic cleft - the narrow extracellular space (200-300 Angstroms wide) separating the two membranes
Types of Synapses
1. Chemical Synapses
The most common type. An action potential in the presynaptic terminal triggers release of a chemical messenger (neurotransmitter) from synaptic vesicles. The neurotransmitter diffuses across the cleft and binds to receptors on the postsynaptic membrane, producing an electrical or biochemical response.
Key structural components:
- Presynaptic terminal (bouton/synaptic knob): Contains synaptic vesicles (with neurotransmitter), mitochondria (ATP supply for transmitter synthesis), and voltage-gated Ca2+ channels at active zones
- Synaptic vesicles: Store and release neurotransmitter by exocytosis
- Postsynaptic membrane: Bears ionotropic (ligand-gated ion channel) or metabotropic (G protein-coupled) receptors
2. Electrical Synapses
Formed by gap junctions - specialized protein channels (connexins) that directly connect the cytoplasm of adjacent cells, allowing ionic current to flow between them. Transmission is nearly instantaneous and can be bidirectional. Useful for synchronizing large groups of neurons (e.g., hypothalamic hormone-secreting neurons).
Steps in Chemical Synaptic Transmission
From Medical Physiology (Boron & Boulpaep), transmission occurs in 7 steps:
- Neurotransmitter is packaged into vesicles and concentrated/docked at the presynaptic terminal (via SNARE proteins: synaptobrevin/v-SNARE + syntaxin + SNAP-25/t-SNAREs)
- Presynaptic membrane depolarizes (action potential arrives)
- Depolarization opens voltage-gated Ca2+ channels; Ca2+ enters the terminal
- Ca2+ binds to synaptotagmin (a Ca2+-sensing protein), triggering vesicle-membrane fusion and exocytosis - transmitter release increases ~100,000-fold; each exocytosis takes only a fraction of a millisecond
- Transmitter is released into the cleft in quantized (quantal) amounts and diffuses passively across
- Transmitter binds to postsynaptic receptors - opens ion channels (ionotropic) or activates G protein cascades (metabotropic)
- Transmitter is cleared by diffusion, enzymatic degradation, or reuptake into cells
Properties of the Synapse
1. One-Way (Unidirectional) Conduction
Chemical synapses transmit signals only from presynaptic to postsynaptic neuron. This is because only the presynaptic terminal contains vesicles, and only the postsynaptic membrane has receptors. This directionality allows the nervous system to direct signals to specific targets. (Electrical synapses, by contrast, can transmit bidirectionally.)
2. Synaptic Delay
A minimum time is required for chemical transmission - typically 0.5 ms at the shortest and usually 1-5 ms at most synapses. This delay accounts for: (a) discharge of transmitter from the presynaptic terminal, (b) diffusion across the cleft, (c) action of transmitter on the receptor, (d) the response of the postsynaptic membrane. The delay is absent (or near-zero) at electrical synapses.
3. Summation
Spatial summation: Multiple presynaptic terminals firing simultaneously summate their effects on the postsynaptic neuron. Each terminal produces a small local potential (EPSP or IPSP); the algebraic sum determines whether threshold is reached.
Temporal summation: A single presynaptic terminal fires rapidly in succession, and the potentials from each impulse add together because they overlap in time before the previous one has decayed.
4. Facilitation, Augmentation, and Post-Tetanic Potentiation
Repeated stimulation may cause the postsynaptic response to be greater than expected. The common mechanism is increased Ca2+ accumulation in the presynaptic terminal, leading to enhanced neurotransmitter release. Long-term potentiation (LTP) - important in memory and learning - involves both increased presynaptic release and increased postsynaptic receptor sensitivity.
5. Synaptic Fatigue
When excitatory synapses are repetitively stimulated at a rapid rate, the postsynaptic response progressively diminishes over milliseconds to seconds. The main mechanism is depletion of neurotransmitter stores in the presynaptic terminal. Contributing factors include: progressive inactivation of postsynaptic receptors and accumulation of abnormal ion concentrations inside the postsynaptic cell. Fatigue is a protective mechanism - it limits runaway excitation and helps terminate events like epileptic seizures.
6. Effect of pH (Acidosis/Alkalosis)
- Alkalosis increases neuronal excitability - arterial pH rising from 7.4 to 7.8-8.0 can precipitate epileptic seizures
- Acidosis depresses neuronal activity - pH below 7.0 typically causes coma (as in severe diabetic ketoacidosis or uremia)
7. Effect of Hypoxia
Neuronal excitability is critically dependent on oxygen. Cessation of oxygen for only a few seconds can render neurons inexcitable. Interruption of cerebral blood flow causes unconsciousness within 3-7 seconds.
8. Effect of Drugs
- Excitatory agents: Caffeine, theophylline (lower neuronal excitation threshold); strychnine (blocks inhibitory glycine receptors, causing tonic spasms)
- Depressant/anesthetic agents: Increase membrane threshold for excitation, decreasing synaptic transmission (often by dissolving in lipid membranes and altering their physical properties)
9. Excitation vs. Inhibition
The postsynaptic effect depends entirely on the type of neurotransmitter released and the receptor present:
- Excitatory neurotransmitters (e.g., glutamate) - cause depolarization (EPSP)
- Inhibitory neurotransmitters (e.g., GABA, glycine) - cause hyperpolarization (IPSP)
A single neuron integrates the sum of all EPSPs and IPSPs continuously. If the net depolarization reaches threshold at the axon hillock, an action potential is fired.
10. Quantal Release
Neurotransmitter is released in discrete packets called quanta (each quanta = contents of one synaptic vesicle). Spontaneous, random release of single quanta occurs even at rest, producing miniature end-plate potentials (mEPPs). Evoked release during an action potential involves the simultaneous release of many quanta.
11. Convergence and Divergence
- Convergence: Many presynaptic neurons synapse on one postsynaptic neuron (up to 10,000-200,000 synaptic knobs on a single motor neuron)
- Divergence: One presynaptic neuron may synapse on many postsynaptic neurons, distributing the signal widely
Summary Table: Electrical vs. Chemical Synapses
| Feature | Electrical Synapse | Chemical Synapse |
|---|---|---|
| Structural gap | Very narrow (2-4 nm gap junction) | Wider synaptic cleft (200-300 Å) |
| Mediator | Ionic current (no chemical) | Neurotransmitter |
| Direction | Bidirectional (usually) | Unidirectional |
| Delay | Virtually none | 0.5-5 ms |
| Amplification | None | Yes (signal amplified) |
| Modulation | Limited | Extensive |
| Example | Hypothalamic neurons, retinal cells | Most CNS synapses, NMJ |
Sources:
- Guyton and Hall Textbook of Medical Physiology, Ch. 46 - Chemical and Electrical Synapses, Special Characteristics of Synaptic Transmission
- Medical Physiology (Boron & Boulpaep) - Neuronal Synapses, Steps in Synaptic Transmission
- Costanzo Physiology, 7th Edition - Chemical Synapses, Summation, Synaptic Fatigue
- Neuroscience: Exploring the Brain, 5th Edition - The Synapse, Synaptic Integration
Answer these each and every questions
Reading File
Running Command
cd /home/daytona/workspace/attachments/f5d09866-5156-4275-b131-8e4ab6b0aa19 && p…
Reading File
Reading File
Reading File
Reading File
Reading File
Asking for Preferences
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Chapter 1: General Physiology - Complete Answers
Q1. Feedback Mechanisms - Positive and Negative
Definition
A feedback mechanism is a regulatory system in which the output (response) of a process feeds back to influence the input (stimulus), thereby maintaining homeostasis.
Components of a Feedback System
Every feedback system has:
- Sensor/Receptor - detects a change in the controlled variable
- Control center - processes information and determines the response
- Effector - carries out the corrective response
A. Negative Feedback Mechanism
Definition: The response (output) acts to oppose or reverse the original stimulus, bringing the variable back toward its set point.
Key Features:
- Most common type in the body
- Stabilizing - maintains homeostasis
- The system "feeds back negatively" to reduce the error
Examples:
| Variable | Sensor | Control Center | Effector | Response |
|---|---|---|---|---|
| Body temperature (↑) | Thermoreceptors | Hypothalamus | Sweat glands, cutaneous vasodilation | Temperature falls back to normal |
| Blood glucose (↑) | Beta cells of pancreas | Pancreas | Insulin secretion | Glucose uptake, level falls |
| Blood pressure (↑) | Baroreceptors (carotid sinus) | Medullary cardiovascular center | Heart rate ↓, vasodilation | Blood pressure falls |
| Blood Ca2+ (↑) | Parathyroid cells | Parathyroid gland | Calcitonin secretion | Ca2+ falls |
| Serum osmolality (↑) | Osmoreceptors | Hypothalamus | ADH secretion | Water reabsorption, osmolality falls |
B. Positive Feedback Mechanism
Definition: The response (output) amplifies or reinforces the original stimulus, driving the system further away from the set point until a specific endpoint is reached.
Key Features:
- Less common - not used for routine homeostasis
- Self-amplifying and explosive in nature
- Always moves toward a final outcome (event-driven)
- Requires an external mechanism to terminate the loop
Examples:
-
Action Potential (Hodgkin Cycle):
- Depolarization → Na+ channels open → Na+ influx → further depolarization → more Na+ channels open (self-amplifying)
- Terminated by: Na+ channel inactivation + K+ channel opening
-
Parturition (childbirth):
- Fetal head stretches cervix → oxytocin released → uterine contractions → more cervical stretch → more oxytocin
- Terminated by: delivery of baby
-
Blood clotting (coagulation cascade):
- Each step amplifies the next, producing a burst of thrombin and fibrin clot
- Terminated by: clot formation + natural anticoagulants
-
Surge of LH at ovulation:
- Rising estrogen (at high levels) triggers LH surge → ovulation
- Terminated by: collapse of estrogen after ovulation
Comparison Table
| Feature | Negative Feedback | Positive Feedback |
|---|---|---|
| Direction | Opposes stimulus | Amplifies stimulus |
| Purpose | Maintain homeostasis | Drive a process to completion |
| Frequency | Very common | Rare |
| Stability | Stabilizing | Destabilizing (until endpoint) |
| Termination | Self-terminating | Requires external termination |
| Examples | BP, temperature, glucose regulation | Action potential, parturition, LH surge, coagulation |
Q2. Transport Across Cell Membrane
The cell membrane is a selectively permeable phospholipid bilayer. Substances cross it by two broad mechanisms:
A. Passive Transport (no energy required)
Substances move down their concentration/electrochemical gradient.
1. Simple Diffusion
- Lipid-soluble (non-polar) substances pass directly through the lipid bilayer
- Rate depends on: concentration gradient, membrane thickness, lipid solubility (partition coefficient), surface area, molecular size
- Fick's Law: Rate of diffusion = (D × A × ΔC) / thickness
- Examples: O2, CO2, steroids, urea, ethanol, fatty acids
2. Facilitated Diffusion
- Water-soluble or charged substances cross via specific carrier proteins or channel proteins, still down their gradient (no energy needed)
a) Channel-mediated:
- Ion channels (Na+, K+, Ca2+, Cl- channels)
- Aquaporins (water channels)
- Can be: voltage-gated, ligand-gated, mechanically gated
b) Carrier-mediated:
- Conformational change in a carrier protein shuttles the solute
- Shows: saturation kinetics, specificity, competition
- Example: GLUT transporters for glucose
3. Osmosis
- Movement of water across a semipermeable membrane from low solute concentration to high solute concentration
- Driven by osmotic pressure gradient
- Osmolarity: Number of osmoles per litre of solution
- Normal plasma osmolality = 285-295 mOsm/kg
B. Active Transport (energy required)
Substances move against their concentration/electrochemical gradient. Requires ATP (directly or indirectly).
1. Primary Active Transport
- Uses ATP directly
- Na+-K+ ATPase pump: Pumps 3 Na+ out, 2 K+ in per ATP cycle; electrogenic; maintains resting membrane potential
- Ca2+-ATPase pump: Removes Ca2+ from cytoplasm
- H+-K+ ATPase: In gastric parietal cells (acid secretion)
2. Secondary Active Transport
- Uses the electrochemical gradient created by the Na+-K+ pump (indirect ATP use)
a) Co-transport (Symport): Na+ and another solute move in the same direction
- Example: SGLT (Na+-glucose cotransporter) in intestine and renal tubule; Na+-amino acid transporters
b) Counter-transport (Antiport): Na+ moves in, another solute moves out
- Example: Na+-H+ exchanger, Na+-Ca2+ exchanger
C. Vesicular Transport (for large molecules)
| Type | Direction | Process | Examples |
|---|---|---|---|
| Endocytosis | Into cell | Membrane engulfs particle | Receptor-mediated endocytosis (LDL, hormones) |
| Phagocytosis | Into cell | Large particles engulfed | Bacteria engulfed by macrophages |
| Pinocytosis | Into cell | Fluid + dissolved solutes | Protein absorption |
| Exocytosis | Out of cell | Vesicle fuses with membrane | Neurotransmitter release, hormone secretion |
Summary Table: Transport Mechanisms
| Mechanism | Energy | Direction | Examples |
|---|---|---|---|
| Simple diffusion | No | Down gradient | O2, CO2, steroids |
| Facilitated diffusion (channel) | No | Down gradient | Na+, K+, water (AQP) |
| Facilitated diffusion (carrier) | No | Down gradient | Glucose (GLUT) |
| Primary active transport | Yes (ATP) | Against gradient | Na+-K+ pump, Ca2+ pump |
| Secondary active (symport) | Indirect | Against gradient of one | SGLT (Na+-glucose) |
| Secondary active (antiport) | Indirect | Against gradient of one | Na+-H+ exchanger |
| Endocytosis/Exocytosis | Yes | Both directions | LDL uptake, neurotransmitter release |
Q3. Body Fluid Compartments - Oedema - ORS
A. Body Fluid Compartments
Total body water (TBW) = ~60% of body weight in adult male (50% in adult female)
- In a 70 kg adult man: TBW = 42 litres
Two main compartments:
Total Body Water (42 L)
├── Intracellular Fluid (ICF) = 28 L (2/3 of TBW = ~40% body weight)
└── Extracellular Fluid (ECF) = 14 L (1/3 of TBW = ~20% body weight)
├── Plasma = 3 L (~4.5% body weight)
├── Interstitial Fluid = 11 L (~15% body weight)
└── Transcellular Fluid = ~1-2 L (synovial, CSF, peritoneal, pericardial, intraocular)
Rule of 60-40-20:
- 60% body weight = total body water
- 40% body weight = intracellular fluid
- 20% body weight = extracellular fluid
Composition:
| Ion/Substance | ICF | ECF (Plasma) |
|---|---|---|
| Main cation | K+ (140 mEq/L) | Na+ (142 mEq/L) |
| Main anion | Proteins, Phosphate | Cl-, HCO3- |
| Glucose | Low | ~90 mg/dL |
| Protein | High | Albumin (main) |
| Osmolarity | ~285 mOsm/L | ~285 mOsm/L |
Measurement of fluid compartments: Indicator dilution principle (Volume = Amount injected / Concentration at equilibrium)
- TBW: Tritiated water, antipyrine
- ECF: Inulin, mannitol, sucrose, sodium thiosulfate
- Plasma volume: Evans blue dye, radioactive albumin
- Blood volume = Plasma volume / (1 - haematocrit)
- ICF = TBW - ECF
B. Oedema
Definition: Accumulation of excess fluid in the interstitial (extracellular) tissue spaces.
Starling Forces (Govern fluid exchange at capillary)
Fluid movement = Kf [(Pc - Pi) - σ(πc - πi)]
Where:
- Pc = Capillary hydrostatic pressure (pushes fluid OUT)
- Pi = Interstitial hydrostatic pressure (pushes fluid IN)
- πc = Plasma oncotic (colloid osmotic) pressure (pulls fluid IN)
- πi = Interstitial oncotic pressure (pulls fluid OUT)
Causes of Oedema (by mechanism):
| Mechanism | Cause | Examples |
|---|---|---|
| ↑ Capillary hydrostatic pressure | Venous obstruction, heart failure | CCF, DVT, portal hypertension |
| ↓ Plasma oncotic pressure | Low albumin | Nephrotic syndrome, liver failure, malnutrition (kwashiorkor) |
| ↑ Capillary permeability | Inflammation, allergy | Burns, anaphylaxis, sepsis |
| Lymphatic obstruction | Lymph cannot drain interstitium | Filariasis (elephantiasis), post-mastectomy lymphoedema |
| Na+ and water retention | Renal causes | Renal failure, hyperaldosteronism |
Types:
- Pitting oedema: Leaves a pit when pressed (cardiac, renal, nutritional, venous)
- Non-pitting oedema: No pitting (lymphoedema, myxoedema in hypothyroidism)
C. ORS (Oral Rehydration Solution)
Principle: The discovery that glucose (even in the presence of diarrhoea) actively co-transports Na+ across the intestinal epithelium via the SGLT1 (Na+-glucose cotransporter) drove the development of ORS.
WHO Standard ORS Composition (per litre of water):
| Substance | Amount |
|---|---|
| NaCl | 3.5 g |
| KCl | 1.5 g |
| Trisodium citrate (or NaHCO3) | 2.9 g |
| Glucose (anhydrous) | 20 g |
| Na+ | 75 mEq/L |
| K+ | 20 mEq/L |
| Cl- | 65 mEq/L |
| Citrate | 10 mEq/L |
| Glucose | 75 mmol/L |
| Osmolarity | 245 mOsm/L (reduced osmolarity ORS) |
Mechanism:
- Na+ and glucose are co-transported into enterocytes by SGLT1
- Na+ absorption drives water absorption osmotically
- Citrate/bicarbonate corrects metabolic acidosis
- K+ replaces losses from diarrhoea
Indications: Mild to moderate dehydration from diarrhoea (cholera, gastroenteritis)
Q4. Resting Membrane Potential (RMP) and Action Potential
A. Resting Membrane Potential (RMP)
Definition: The potential difference across the cell membrane in a resting (non-excited) excitable cell, with the interior negative relative to the exterior.
Normal values:
- Nerve fibers: -70 mV (Guyton & Hall)
- Skeletal muscle: -90 mV
- Cardiac muscle: -90 mV
- Smooth muscle: -50 to -55 mV
Basis of RMP
Ion concentrations across nerve membrane (from Guyton & Hall):
| Ion | Outside (mEq/L) | Inside (mEq/L) | Ratio |
|---|---|---|---|
| Na+ | 142 | 14 | 10:1 (out > in) |
| K+ | 4 | 140 | 35:1 (in > out) |
| Cl- | 103 | 4 | 26:1 (out > in) |
Three factors establish RMP:
-
K+ diffusion potential: Membrane is ~100x more permeable to K+ than Na+ at rest. K+ leaks out down its concentration gradient, leaving negative charge inside. K+ equilibrium potential (Ek) = -94 mV.
-
Na+ leak: Small but slightly depolarizes. Na+ Nernst potential = +61 mV. The combined Goldman equation potential for Na+ and K+ gives -86 mV.
-
Na+-K+ ATPase pump: Electrogenic - pumps 3 Na+ out for 2 K+ in, contributing an additional -4 mV. This also actively maintains the concentration gradients.
Result: Net RMP ≈ -90 mV (Guyton) or -70 to -80 mV (Costanzo)
Nernst Equation (equilibrium potential for a single ion):
E = (61/z) × log([ion]outside / [ion]inside)
B. Action Potential (AP)
Definition: A rapid, transient, self-propagating reversal of membrane polarity in excitable cells, serving as the fundamental unit of signal transmission.
Phases of Action Potential:
| Phase | What Happens | Ion Movement | Membrane Potential |
|---|---|---|---|
| Resting | Membrane at rest | K+ leak outward maintains RMP | -70 mV |
| Depolarization (upstroke) | Stimulus → reaches threshold (-55 mV) → voltage-gated Na+ channels open rapidly | Na+ rushes IN (inward current) | -70 → 0 → +35 mV (overshoot) |
| Repolarization | Na+ channels inactivate; voltage-gated K+ channels open | K+ flows OUT | +35 → -70 mV |
| Undershoot (hyperpolarizing afterpotential) | K+ channels slow to close | Excess K+ outflow | Below -70 mV |
| Return to resting | K+ channels close; Na+-K+ pump restores gradients | Na+ out, K+ in | Returns to -70 mV |
Threshold potential: ~-55 mV (must be reached for AP to fire)
Overshoot: Membrane becomes briefly positive (approximately +35 mV) - approaches Na+ equilibrium potential (+61 mV) but doesn't reach it
Properties of Action Potential:
- All-or-None law: Either full AP fires or none - no partial APs
- Propagation: Non-decremental spread along the axon
- Absolute refractory period: Na+ channels completely inactivated; no AP possible regardless of stimulus strength (~1 ms in nerve)
- Relative refractory period: Na+ channels partially recovered; a stronger-than-normal stimulus can evoke AP
- Threshold: A minimum depolarization must be reached
Ionic Basis - Hodgkin & Huxley Cycle (Positive Feedback):
Depolarization → Na+ channels open → Na+ in → more depolarization → more Na+ channels open (self-amplifying) → terminated by Na+ channel inactivation + K+ channel opening
Sources:
- Guyton and Hall Textbook of Medical Physiology - Body fluid compartments, RMP, Action potential
- Costanzo Physiology, 7th Edition - RMP, Action potential, transport mechanisms
- Medical Physiology (Boron & Boulpaep) - Membrane transport, RMP
Tell me when you're ready to continue with Chapter 2: Blood and I'll answer all those topics as well.
Continue
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Chapter 2: Blood - Complete Answers
Q1. Plasma Proteins
Definition
Plasma proteins are the proteins dissolved in blood plasma. Total plasma protein concentration = 6–8 g/dL.
Classification and Functions
| Protein | Normal Level | Site of Synthesis | Functions |
|---|---|---|---|
| Albumin | 3.5–5.0 g/dL | Liver | Maintains oncotic pressure (80% of total); transport of bilirubin, hormones, fatty acids, drugs; nutritional reserve; acts as buffer |
| Globulins | 2.0–3.5 g/dL | Liver (α, β); Lymphocytes (γ) | α1: α1-antitrypsin, α1-acid glycoprotein; α2: ceruloplasmin, haptoglobin; β: transferrin, complement; γ: immunoglobulins (IgG, IgA, IgM, IgE, IgD) |
| Fibrinogen | 200–400 mg/dL | Liver | Blood coagulation - converted to fibrin by thrombin; acute phase reactant |
| Prothrombin | — | Liver (vitamin K dependent) | Coagulation - converted to thrombin |
| Transferrin | — | Liver | Iron transport in plasma |
| Ceruloplasmin | — | Liver | Copper transport; ferroxidase activity |
| Haptoglobin | — | Liver | Binds free haemoglobin; prevents renal loss |
| Complement proteins | — | Liver | Innate immunity |
Key Functions of Plasma Proteins (summary)
- Oncotic pressure (colloid osmotic pressure): ~25 mmHg - prevents fluid leaking from capillaries; albumin contributes most
- Transport: Bind and carry hormones (thyroxine, cortisol), lipids, drugs, bilirubin, metals
- Coagulation: Fibrinogen, prothrombin, clotting factors
- Immunity: Immunoglobulins (antibodies), complement
- Buffering: 15% of blood buffering capacity (via -COOH and -NH2 groups)
- Acute phase response: CRP, fibrinogen, α1-antitrypsin rise during inflammation
- Nutritional reserve: Amino acid pool
Hypoproteinaemia - Causes and Effects
- Causes: Malnutrition/starvation, liver disease (decreased synthesis), nephrotic syndrome (urinary loss), protein-losing enteropathy
- Effect: Decreased oncotic pressure → oedema
A:G Ratio (Albumin:Globulin) = normally 1.5-2.5:1; inverted in chronic liver disease, multiple myeloma
Q2. Haemoglobin, Erythropoiesis, Polycythemia
A. Haemoglobin (Hb)
Structure:
- Molecular weight: 64,500 Da
- 4 subunits: each has a globin chain + haem group
- Haem = protoporphyrin ring + Fe²⁺ (ferrous iron)
- Each haem binds ONE O2 molecule → one Hb molecule carries 4 O2 molecules
- Adult Hb (HbA1): 2α + 2β chains (major fraction, 97%)
- HbA2: 2α + 2δ (2.5%)
- HbF (Foetal): 2α + 2γ - higher O2 affinity than HbA (lower 2,3-DPG binding)
Normal values:
- Adult male: 13.5–17.5 g/dL
- Adult female: 12–16 g/dL
- Newborn: ~19 g/dL
Functions of Hb:
- O2 transport (oxyhaemoglobin)
- CO2 transport (carbaminohaemoglobin - ~23% of CO2)
- Buffering (Haldane effect)
- Carries NO (nitric oxide)
O2-Hb Dissociation Curve:
- Sigmoid (S-shaped) due to cooperative binding (allosteric effect)
- Right shift (↓ affinity, ↑ O2 release): ↑ CO2, ↑ H+ (↓ pH), ↑ temperature, ↑ 2,3-DPG (Bohr effect)
- Left shift (↑ affinity, ↓ O2 release): ↓ CO2, ↓ H+, ↓ temperature, ↓ 2,3-DPG, HbF, CO poisoning, methaemoglobin
B. Erythropoiesis
Definition: The process of formation of red blood cells (erythrocytes).
Sites:
- Foetal: Yolk sac (0-2 months) → Liver & Spleen (2-7 months) → Bone marrow (from 5 months onward)
- After birth: Red bone marrow (sternum, vertebrae, ribs, pelvis, skull, proximal long bones)
Stages of Development (in bone marrow):
Pluripotent Stem Cell
↓
CFU-GEMM (Mixed myeloid progenitor)
↓
BFU-E (Burst-forming unit - erythroid)
↓
CFU-E (Colony-forming unit - erythroid)
↓
Pronormoblast (Proerythroblast)
↓
Early Normoblast (Basophilic erythroblast) - active Hb synthesis begins
↓
Intermediate Normoblast (Polychromatic erythroblast)
↓
Late Normoblast (Orthochromatic erythroblast) - nucleus extruded
↓
Reticulocyte (still has ribosomes + mRNA, can synthesize Hb)
↓ (1-2 days in circulation, matures in spleen)
Mature RBC (biconcave disc, no nucleus, no organelles)
Requirements for Erythropoiesis:
| Factor | Role |
|---|---|
| Iron | Haem synthesis |
| Vitamin B12 | DNA synthesis (nuclear maturation); absorbed with intrinsic factor |
| Folic acid | DNA synthesis |
| Vitamin C | Iron absorption |
| Erythropoietin (EPO) | Key growth factor |
| Proteins | Globin chain synthesis |
| Vitamin B6 (pyridoxine) | δ-ALA synthesis (first step of haem) |
| Copper | Ceruloplasmin → Fe3+ to Fe2+ conversion |
Regulation by Erythropoietin (EPO):
- Produced mainly by peritubular cells of the kidney (90%) and liver (10%)
- Stimulus: Tissue hypoxia (↓ pO2, anaemia, ↑ altitude, reduced blood flow)
- Action: Stimulates BFU-E → CFU-E differentiation, accelerates maturation, increases reticulocyte release
- Negative feedback: When Hb rises and oxygenation improves, EPO production drops
Normal RBC count:
- Male: 4.5–5.5 million/μL
- Female: 3.8–5.0 million/μL
- Life span: ~120 days
- Destruction: By macrophages in spleen, liver, bone marrow (reticuloendothelial system)
C. Polycythemia
Definition: Increase in the total RBC mass / haemoglobin concentration above normal.
| Type | Definition | Mechanism |
|---|---|---|
| Primary polycythemia (Polycythemia vera) | Clonal myeloproliferative disorder | JAK2 mutation → autonomous RBC production independent of EPO; EPO levels LOW |
| Secondary polycythemia | Increased RBC production in response to stimulus | EPO levels HIGH |
| - Physiological | High altitude, heavy exercise | ↓ O2 tension → ↑ EPO |
| - Pathological | Chronic lung disease, cyanotic heart disease, renal cell carcinoma (inappropriate EPO), EPO doping | |
| Relative (Spurious) polycythemia | Normal RBC mass but reduced plasma volume | Dehydration, burns (Gaisbock syndrome) |
Features of Polycythemia vera:
- Raised Hb, haematocrit, RBC count
- Splenomegaly
- Plethoric facies, hypertension
- Thrombotic tendency (stroke, DVT, PE)
- Pruritus after hot bath (histamine from basophils)
- Bleeding tendency (abnormal platelet function)
Q3. Anaemia and Jaundice
A. Anaemia
Definition: Reduction in haemoglobin concentration below the normal for age and sex:
- Male: Hb < 13.5 g/dL
- Female: Hb < 12.0 g/dL
- Children: Hb < 11 g/dL
Classification by Pathophysiology:
| Mechanism | Examples |
|---|---|
| Decreased production | Iron deficiency, B12/folate deficiency, aplastic anaemia, anaemia of chronic disease, renal failure (↓ EPO) |
| Increased destruction (haemolysis) | Sickle cell disease, thalassaemia, G6PD deficiency, hereditary spherocytosis, autoimmune haemolytic anaemia, malaria |
| Blood loss | GI bleeding, menorrhagia, trauma |
Classification by MCV (cell size):
| Type | MCV | Causes |
|---|---|---|
| Microcytic hypochromic | < 80 fL | Iron deficiency, thalassaemia, sideroblastic, chronic disease |
| Normocytic normochromic | 80-100 fL | Acute blood loss, haemolysis, aplastic anaemia, renal failure |
| Macrocytic | > 100 fL | B12/folate deficiency (megaloblastic), alcohol, liver disease, hypothyroidism |
Clinical Features: Pallor, fatigue, breathlessness on exertion, palpitations, tachycardia, systolic flow murmur, koilonychia (iron deficiency), glossitis, angular stomatitis, neurological signs (B12 deficiency)
B. Jaundice (Icterus)
Definition: Yellow discolouration of skin, sclerae, and mucous membranes due to elevated serum bilirubin (> 2-3 mg/dL; clinical detection > 1 mg/dL when sensitive).
Bilirubin Metabolism:
- Haemoglobin broken down by RES → Haem → Biliverdin → Unconjugated bilirubin (indirect, water-insoluble, albumin-bound)
- Transported to liver → conjugated with glucuronic acid by UDP-glucuronyl transferase → Conjugated bilirubin (direct, water-soluble)
- Excreted in bile → gut → Urobilinogen (some reabsorbed - enterohepatic circulation) → Urobilin (stool colour) + Stercobilin
Classification of Jaundice:
| Type | Cause | Bilirubin | Urine | Stool |
|---|---|---|---|---|
| Pre-hepatic (Haemolytic) | Excess RBC destruction | ↑ Unconjugated | Urobilinogen ↑ (no bilirubin) | Dark |
| Hepatic (Hepatocellular) | Liver cell damage | Both ↑ | Bilirubin + Urobilinogen | Pale/normal |
| Post-hepatic (Obstructive) | Bile duct obstruction | ↑ Conjugated | Bilirubin ↑ (dark urine), no urobilinogen | Pale (clay coloured), steatorrhoea |
Examples:
- Pre-hepatic: Haemolytic anaemias, malaria, transfusion reaction
- Hepatic: Hepatitis, cirrhosis, Gilbert's syndrome, Crigler-Najjar
- Post-hepatic: Gallstones, carcinoma head of pancreas, cholangiocarcinoma
Neonatal Jaundice:
- Physiological: Days 2-3 to day 10 due to high foetal Hb breakdown + immature liver glucuronyl transferase
- Pathological: Rh/ABO incompatibility, G6PD, congenital infections
- Kernicterus: Unconjugated bilirubin crosses BBB → deposits in basal ganglia → brain damage
Q4. Functions of WBC (White Blood Cells)
Normal WBC count: 4,000-11,000/μL
| WBC Type | % | Functions |
|---|---|---|
| Neutrophils | 55-70% | Phagocytosis of bacteria; first responders; release lysozyme, defensins, myeloperoxidase; NET (neutrophil extracellular traps) formation |
| Eosinophils | 1-4% | Defense against parasites (helminths); release major basic protein; modulate allergic reactions; phagocytosis; eosinophilia in allergy and parasitic infections |
| Basophils | 0-1% | Release histamine and heparin (hypersensitivity reactions); IgE receptors on surface; similar function to mast cells |
| Monocytes | 2-8% | Phagocytosis; differentiate into macrophages in tissues; antigen presentation; release cytokines (IL-1, TNF); part of mononuclear phagocyte system |
| Lymphocytes | 20-40% | Specific immunity: B cells → antibody production; T cells → cell-mediated immunity; NK cells → kill virus-infected and tumour cells |
Leukocyte Disorders:
- Leukocytosis: ↑ WBCs - infection, inflammation, leukaemia
- Leukopenia: ↓ WBCs - viral infections, aplastic anaemia, chemotherapy
- Shift to left: Increased band (immature) neutrophils - severe bacterial infection
Q5. Immunity - Classification, Humoral and Cell-Mediated
Classification of Immunity
Immunity
├── Innate (Non-specific, Natural)
│ ├── Physical barriers (skin, mucous membranes)
│ ├── Chemical barriers (lysozyme, acids, complement)
│ └── Cellular (neutrophils, macrophages, NK cells)
└── Adaptive (Specific, Acquired)
├── Active
│ ├── Natural (after infection)
│ └── Artificial (vaccination)
└── Passive
├── Natural (maternal IgG via placenta; IgA via breast milk)
└── Artificial (antiserum injection)
Humoral Immunity (B-cell mediated)
- Mediated by: B lymphocytes → Plasma cells → Antibodies (immunoglobulins)
- Antigen recognition: B cells recognize soluble antigens directly via B-cell receptor (BCR)
- Process:
- Antigen → recognized by B cell → T helper cell (CD4+) provides co-stimulation
- B cell proliferates → plasma cells (antibody secretion) + memory B cells
- Antibodies circulate and neutralize antigen
- Antibody Classes: IgG (most abundant; crosses placenta), IgA (secretory, in saliva/milk), IgM (first produced; pentamer; activates complement), IgE (allergy/parasites), IgD (B-cell surface receptor)
- Effective against: Extracellular bacteria, toxins, viruses (before cell entry)
Cell-Mediated Immunity (T-cell mediated)
- Mediated by: T lymphocytes (T cells)
- Types:
- CD4+ T helper (Th) cells: Recognize antigen on MHC class II; activate B cells, CD8+ T cells, macrophages; produce cytokines
- Th1 (IL-2, IFN-γ): Activates macrophages and cytotoxic T cells
- Th2 (IL-4, IL-5): Activates B cells, eosinophils; antibody production
- CD8+ Cytotoxic T cells (CTL): Recognize antigen on MHC class I; directly kill virus-infected cells and tumour cells via perforin/granzyme
- Regulatory T cells (Treg): Suppress immune responses; prevent autoimmunity
- CD4+ T helper (Th) cells: Recognize antigen on MHC class II; activate B cells, CD8+ T cells, macrophages; produce cytokines
- Effective against: Intracellular pathogens (viruses, mycobacteria, fungi), tumour cells, transplant rejection, delayed hypersensitivity
Q6. Functions of Platelets, Mechanism of Blood Coagulation (Intrinsic and Extrinsic)
A. Functions of Platelets
Normal count: 150,000–450,000/μL | Life span: ~10 days | Origin: Megakaryocytes in bone marrow
Functions:
- Vascular repair - adhesion: Platelets adhere to exposed collagen (via vWF and GPIb receptor) when endothelium is damaged
- Platelet plug formation: Platelets aggregate to seal small vessel breaks (primary haemostasis)
- Activation and release reaction: ADP, thromboxane A2, serotonin released → amplify aggregation; TXA2 causes vasoconstriction
- Support coagulation: Platelet phospholipids (platelet factor 3 / PF3) provide surface for coagulation factor complexes (intrinsic tenase, prothrombinase)
- Clot retraction: Platelet thrombostenin (actin-myosin) contracts the clot
- Platelet-derived growth factor (PDGF): Promotes vascular wall repair
- Vasoconstriction: Via thromboxane A2 and serotonin release
Thrombocytopenia (platelets < 100,000/μL): Petechiae, purpura, prolonged bleeding time
B. Mechanism of Blood Coagulation
The coagulation cascade converts soluble fibrinogen to insoluble fibrin via sequential activation of clotting factors.
Clotting Factors:
| Factor | Name |
|---|---|
| I | Fibrinogen |
| II | Prothrombin |
| III | Tissue Factor (Thromboplastin) |
| IV | Calcium |
| V | Proaccelerin (Labile factor) |
| VII | Proconvertin (Stable factor) |
| VIII | Antihemophilic factor A |
| IX | Christmas factor (Antihemophilic factor B) |
| X | Stuart-Prower factor |
| XI | Plasma thromboplastin antecedent |
| XII | Hageman factor (contact factor) |
| XIII | Fibrin stabilizing factor |
Extrinsic Pathway (Tissue Factor Pathway - FAST):
- Trigger: Tissue damage → Tissue Factor (Factor III) released
- TF + Factor VII → TF-VIIa complex
- Activates Factor X → Xa (with Ca2+ and Factor V)
- Time: 15 seconds | Measured by: PT (Prothrombin Time)
Intrinsic Pathway (Contact Activation - SLOW):
- Trigger: Contact of Factor XII with exposed subendothelial collagen
- XII → XIIa → XI → XIa → IX → IXa → (with VIII, Ca2+, PF3) → X → Xa
- Time: 1-6 minutes | Measured by: aPTT (activated Partial Thromboplastin Time)
Common Pathway:
Xa + Va + Ca2+ + Phospholipid (Prothrombinase complex)
↓
Prothrombin (II) → Thrombin (IIa)
↓
Fibrinogen (I) → Fibrin monomer
↓ (Factor XIIIa + Ca2+)
Cross-linked Fibrin clot (stable)
Q7. Anticoagulants - Natural and Artificial
A. Natural Anticoagulants
| Anticoagulant | Mechanism |
|---|---|
| Intact endothelium | Smooth surface prevents contact activation; glycocalyx repels clotting factors; produces prostacyclin (PGI2) and NO → inhibit platelet aggregation |
| Thrombomodulin | Endothelial protein binds thrombin → activates Protein C |
| Protein C + Protein S | Protein C (activated by thrombomodulin-thrombin complex) inactivates Factors Va and VIIIa; Protein S is cofactor |
| Antithrombin III (AT-III) | α-globulin; inhibits thrombin and Factors IXa, Xa, XIa, XIIa; activity greatly enhanced by heparin |
| Fibrin itself | Adsorbs and removes 85-90% of thrombin during clot formation |
| Tissue Factor Pathway Inhibitor (TFPI) | Inhibits TF-VIIa complex; limits extrinsic pathway |
| α2-macroglobulin | Binds and inactivates thrombin |
| Plasminogen/Plasmin (fibrinolysis) | tPA and uPA convert plasminogen to plasmin → lyses fibrin clot; α2-antiplasmin inhibits excess plasmin |
B. Artificial (Clinical) Anticoagulants
| Anticoagulant | Mechanism | Route | Use |
|---|---|---|---|
| Heparin (unfractionated) | Activates AT-III ~1000-fold → inhibits thrombin (IIa) and Xa | IV/SC | Immediate anticoagulation; DVT, PE, ACS, dialysis |
| Low Molecular Weight Heparin (LMWH) (enoxaparin, dalteparin) | Mainly inhibits Factor Xa; more predictable pharmacokinetics | SC | DVT prophylaxis/treatment, ACS; preferred in pregnancy |
| Warfarin | Vitamin K antagonist - inhibits hepatic synthesis of factors II, VII, IX, X (and Proteins C, S) | Oral | Long-term anticoagulation; AF, mechanical heart valves; monitored by INR/PT |
| Direct Oral Anticoagulants (DOACs) | Oral | ||
| - Rivaroxaban, Apixaban | Direct Factor Xa inhibitors | AF, DVT/PE, post-orthopaedic surgery | |
| - Dabigatran | Direct thrombin (IIa) inhibitor | AF, DVT/PE | |
| Sodium citrate/EDTA | Chelate Ca2+ (Factor IV) | In vitro | Blood collection tubes, blood banking |
| Heparin (in vitro) | As above | In vitro | Blood gas syringes |
Q8. Blood Groups - Landsteiner's Law, ABO, Rh System, HDN
A. Landsteiner's Law
"If an antigen is present on the red cell surface, the corresponding antibody will be absent from the plasma; if the antigen is absent from the red cell surface, the corresponding antibody will be present in the plasma."
- These naturally occurring antibodies (isohemagglutinins) are IgM and appear without prior exposure (formed from gut bacterial antigens that share structure with blood group antigens)
B. ABO Blood Group System
| Blood Group | Antigen on RBC | Antibody in Plasma | Genotype |
|---|---|---|---|
| A | A antigen | Anti-B | AA or AO |
| B | B antigen | Anti-A | BB or BO |
| AB | A and B antigens | None | AB |
| O | None (H antigen) | Anti-A and Anti-B | OO |
Universal Donor: O (no antigens on RBC)
Universal Recipient: AB (no antibodies in plasma)
Compatibility for Transfusion:
- Donor O → can give to O, A, B, AB
- Donor A → can give to A, AB
- Donor B → can give to B, AB
- Donor AB → can only give to AB
C. Rh Blood Group System
- Rh antigen (D antigen) is the most important: present on RBC surface
- Rh positive: D antigen present (~85% of population)
- Rh negative: D antigen absent (~15% of population)
- Key difference from ABO: Anti-D antibodies do NOT occur naturally - they are only produced after exposure to Rh-positive blood (transfusion or pregnancy)
- Anti-D is IgG (can cross placenta, unlike ABO IgM)
D. Rh Incompatibility / Haemolytic Disease of the Newborn (HDN / Erythroblastosis Fetalis)
Mechanism:
- Rh-negative mother carries Rh-positive foetus (father Rh+)
- During delivery (or miscarriage/amniocentesis), foetal Rh+ RBCs leak into maternal circulation
- Mother produces anti-D IgG antibodies (sensitization - usually no problem in 1st pregnancy)
- In subsequent Rh+ pregnancies, anti-D IgG crosses placenta → attaches to foetal RBCs → haemolysis
- Consequences: Foetal anaemia, jaundice, oedema (hydrops fetalis), cardiac failure, kernicterus (bilirubin deposits in brain)
Protection - Rh Immune Globulin (RhIg / Anti-D / RhoGAM):
- Given to Rh-negative mother at 28 weeks and within 72 hours of delivery
- Masks fetal Rh antigens that entered maternal circulation → prevents sensitization
ABO Incompatibility vs Rh Incompatibility:
| Feature | ABO | Rh |
|---|---|---|
| First pregnancy affected | Yes (IgG already present in some O mothers) | No (sensitization needed first) |
| Antibody type | IgM (mainly) | IgG |
| Severity | Usually mild | Potentially severe |
| Prevention | Not possible | RhIg injection |
Q9. Blood Transfusion - Matched and Mismatched Reaction
Cross-matching
Before transfusion:
- ABO and Rh typing of donor and recipient
- Cross-match test:
- Major cross-match: Donor RBC + recipient serum (most important)
- Minor cross-match: Donor serum + recipient RBC
- Coombs test (DAT/IAT): Detects antibodies on RBC surface
Matched Transfusion
- Compatible blood given → smooth transfusion, no adverse reaction
- Patient monitored for first 15 minutes (most reactions occur early)
Mismatched (Incompatible) Transfusion Reaction
Acute Haemolytic Transfusion Reaction (most dangerous):
- Usually ABO incompatibility (clerical error is most common cause)
- Anti-A or anti-B antibodies + transfused RBC antigens → intravascular haemolysis
- Features (occur within minutes):
- Fever, chills, rigors
- Severe backache/loin pain (renal involvement)
- Haemoglobinuria (dark/red urine)
- Hypotension, shock
- DIC (disseminated intravascular coagulation)
- Acute renal failure
- Management: Stop transfusion immediately; IV fluids, maintain urine output; treat DIC; check blood bank for error
Other Transfusion Reactions:
| Reaction | Cause | Features | Management |
|---|---|---|---|
| Febrile non-haemolytic | Recipient antibodies to donor WBC antigens | Fever, chills (no haemolysis) | Antipyretics; leucocyte-depleted blood |
| Allergic/Urticarial | IgE reaction to plasma proteins | Urticaria, itching | Antihistamines |
| Anaphylaxis | Anti-IgA antibodies in IgA-deficient patients | Bronchospasm, hypotension | Epinephrine; IgA-free blood |
| Transfusion-related acute lung injury (TRALI) | Donor antibodies vs recipient WBCs | Acute respiratory distress, hypoxia | Supportive; avoid implicated donor |
| Delayed haemolytic | Anamnestic antibody response (IgG) days later | Anaemia, jaundice 3-10 days post-transfusion | Usually self-limiting |
| Volume overload (TACO) | Too rapid transfusion | Pulmonary oedema, hypertension | Slow rate, diuretics |
| Infections | Bacterial/viral contamination | Variable | Prophylaxis, screening |
Sources: Guyton & Hall Textbook of Medical Physiology; Ganong's Review of Medical Physiology, 26th Edition; Basic Medical Biochemistry, 6th Edition; Robbins & Kumar Basic Pathology; Bailey & Love's Short Practice of Surgery
Ready to continue with Chapter 3: Nerve Muscle Physiology whenever you are.
Continue and mark long questions short questions
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Chapter 3: Nerve Muscle Physiology
Legend: 🔵 LQ = Long Question (10-15 marks) | 🟡 SQ = Short Question (5 marks)
Q1. 🔵 LQ - Structure and Functions of a Neuron
Structure of a Neuron
A neuron is the structural and functional unit of the nervous system. It consists of:
1. Cell Body (Soma / Perikaryon)
- Contains the nucleus (large, vesicular, prominent nucleolus)
- Nissl bodies (rough ER + ribosomes) - site of protein synthesis; dispersed in axon hillock
- Golgi apparatus, mitochondria, neurofilaments, microtubules
- Axon hillock: cone-shaped origin of axon; lowest threshold for AP generation (spike-initiation zone)
2. Dendrites
- Multiple short, branching processes arising from the soma
- Increase receptive surface area
- Contain Nissl bodies and organelles
- Receive incoming signals (afferent input) from other neurons
- Site of most synaptic inputs; integrate signals through EPSPs and IPSPs
- May have dendritic spines (increase surface area for synaptic contacts)
3. Axon
- Single, long process arising from the axon hillock
- Conducts impulses away from soma (efferent output) - orthodromic direction
- Myelin sheath (in myelinated fibres) produced by Schwann cells (PNS) or oligodendrocytes (CNS)
- Nodes of Ranvier: gaps in myelin (~1-2 μm); site of AP regeneration in saltatory conduction
- Axon terminals (boutons/synaptic knobs): contain synaptic vesicles + mitochondria
- No Nissl bodies → cannot synthesize proteins locally (depends on axonal transport)
- Branching at terminal end = telodendria
Types of Neurons by Structure:
| Type | Structure | Example |
|---|---|---|
| Unipolar | One process only | Sensory neurons of dorsal root ganglion (pseudounipolar) |
| Bipolar | One axon, one dendrite | Retinal photoreceptors, cochlear neurons |
| Multipolar | Multiple dendrites, one axon | Motor neurons, interneurons |
Functions of a Neuron:
- Sensory (afferent): Receive stimuli from periphery, transmit to CNS
- Motor (efferent): Transmit commands from CNS to effectors (muscles, glands)
- Interneurons: Connect sensory and motor neurons; integration, modulation
- Integration: Sum up excitatory and inhibitory inputs at soma to decide firing
- Secretion: Neurosecretory neurons release hormones (hypothalamic neurons)
Q2. 🟡 SQ - Neuroglia
Definition: Neuroglia (glial cells) are non-neuronal supporting cells of the nervous system. They outnumber neurons by about 10:1.
CNS Neuroglia (4 types):
| Cell Type | Features | Functions |
|---|---|---|
| Astrocytes (Protoplasmic in grey matter; Fibrous in white matter) | Star-shaped; largest glia; form end-feet on blood vessels | Physical and metabolic support for neurons; form blood-brain barrier; regulate K+ and neurotransmitter concentration; repair after injury; glycogen storage; guide neuronal migration |
| Oligodendrocytes | Small, few processes; one cell myelinates multiple axons | Myelin formation in CNS (compare: Schwann cells in PNS); maintain axonal integrity |
| Microglia | Small, dark elongated nuclei; branching processes | Phagocytosis (CNS macrophages); surveillance; remove debris; neuroinflammation |
| Ependymal cells | Columnar ciliated cells lining ventricles and central canal | Line ventricles and central canal; produce and circulate CSF; act as barrier |
PNS Neuroglia:
- Schwann cells: Myelin formation and maintenance in PNS; guide nerve regeneration
- Satellite cells: Surround neuron cell bodies in sensory ganglia
Key Functions of Neuroglia:
- Structural support and scaffolding for neurons
- Myelin formation (saltatory conduction)
- Nutrient supply to neurons
- Regulate the extracellular environment (K+, neurotransmitters)
- Blood-brain barrier (astrocyte end-feet)
- Immune defense (microglia)
- CSF production and circulation (ependymal)
- Repair and regeneration guidance
Q3. 🔵 LQ - Types, Functions, and Properties of Nerve Fibres
Classification by Erlanger and Gasser (Based on conduction velocity):
| Fibre Type | Subtype | Diameter (μm) | Myelin | Velocity (m/s) | Function |
|---|---|---|---|---|---|
| A | Aα | 12-20 | Yes | 70-120 | Somatic motor (large motor neurons); proprioception (muscle spindle Ia) |
| A | Aβ | 5-12 | Yes | 30-70 | Touch, pressure, vibration |
| A | Aγ | 3-6 | Yes | 15-30 | Motor to intrafusal muscle fibres (muscle spindle) |
| A | Aδ | 1-5 | Thin | 5-30 | Fast/sharp pain (first pain); cold; touch |
| B | — | 1-3 | Thin | 3-15 | Preganglionic autonomic fibres |
| C | — | 0.2-1.5 | None | 0.5-2 | Slow/burning pain (second pain); warmth; postganglionic autonomic |
Mnemonic: Thicker = Faster; Myelinated > Unmyelinated
Lloyd's Classification (Based on sensory afferents only):
| Group | Corresponds to | Source |
|---|---|---|
| I (Ia, Ib) | Aα | Muscle spindle (Ia), Golgi tendon organ (Ib) |
| II | Aβ | Muscle spindle (secondary endings), skin receptors |
| III | Aδ | Skin pain and temperature |
| IV | C | Unmyelinated pain and temperature |
Properties of Nerve Fibres:
- All-or-None law: A nerve fibre either fires fully or not at all
- Threshold: Minimum stimulus to trigger an AP
- Refractory period: Absolute (no AP possible) and relative (stronger stimulus needed)
- Conductivity: Ability to transmit impulse along its length
- Excitability: Ability to respond to stimuli
- Accommodation: When a slowly rising stimulus is applied, the threshold rises so that the fibre does not fire - due to slow Na+ channel inactivation
- Conduction velocity depends on: fibre diameter, myelination, temperature
- Fatigue: Does not fatigue under physiological conditions (unlike synapses)
- Bidirectional conduction (though normal conduction is orthodromic)
- Metabolic dependency: Requires O2; blocked by hypoxia, ischaemia
Q4. 🟡 SQ - Degeneration and Regeneration in Peripheral Nerves
Classification of Nerve Injury (Seddon):
| Type | Description |
|---|---|
| Neuropraxia | Temporary conduction block; myelin damage only; axon intact; full recovery |
| Axonotmesis | Axon interrupted but endoneurium intact; Wallerian degeneration occurs; good recovery |
| Neurotmesis | Complete nerve transection; recovery poor without surgical repair |
Wallerian Degeneration (after axon is cut):
Distal stump (distal to injury):
- Axon and myelin degenerate within 24-48 hours
- Schwann cells proliferate, phagocytose myelin debris (form bands of Büngner)
- Macrophages invade and clear debris
- Endoneurial tubes persist as regeneration guides
Proximal stump (retrograde - up to nearest node of Ranvier):
- Brief retrograde degeneration to nearest node
- Cell body undergoes chromatolysis (Nissl substance disperses, nucleus moves to periphery) - indicates injury + increased protein synthesis for regeneration
Regeneration:
- Sprouting from proximal axon stump begins within days
- Axon grows along Schwann cell tubes (bands of Büngner) at 1-3 mm/day (~ 1 inch/month)
- Remyelination occurs as axon grows
- Target reinnervation - motor and sensory reinnervation
- Recovery better when endoneurial tubes intact (axonotmesis > neurotmesis)
Factors affecting regeneration:
- Distance to target
- Age (younger = better)
- Nutritional status
- Type of injury
- Surgical repair quality
Q5. 🟡 SQ - Saltatory Conduction
Definition: The mode of action potential propagation in myelinated nerve fibres where the impulse "jumps" from one node of Ranvier to the next, rather than travelling continuously along the membrane.
Basis:
- Myelin sheath acts as electrical insulator (high resistance, low capacitance)
- Voltage-gated Na+ channels are concentrated only at nodes of Ranvier (essentially absent under myelin)
- During AP: strong inward Na+ current at one node generates local circuit currents that jump to the next node, depolarising it to threshold
- The impulse effectively "leaps" from node to node (internodal distance: 0.2-2 mm)
Advantages over continuous conduction:
- Much faster: 70-120 m/s vs 0.5-2 m/s in unmyelinated fibres
- Energy efficient: Na+-K+ pump only needs to restore ion gradients at nodes (small area), not entire membrane
- Space efficient: Same conduction speed in a much thinner myelinated fibre than needed for an unmyelinated fibre
Clinical relevance:
- Multiple sclerosis (MS): Demyelination → loss of saltatory conduction → slowed or blocked conduction → neurological deficits
- Guillain-Barré syndrome: Acute demyelinating polyneuropathy
Q6. 🟡 SQ - Axonal Transport
Definition: The mechanism by which proteins, organelles, and other materials are moved along the axon between the cell body (soma) and the axon terminal, and vice versa.
Why needed: Axons lack ribosomes (no protein synthesis) → proteins must be made in soma and transported to terminals. Also, used material must return for recycling.
Types:
| Type | Direction | Speed | Cargo | Motor protein |
|---|---|---|---|---|
| Fast anterograde | Soma → Terminal | 200-400 mm/day | Synaptic vesicles, membrane proteins, mitochondria | Kinesin |
| Slow anterograde | Soma → Terminal | 1-5 mm/day | Cytoskeletal proteins (actin, tubulin, neurofilaments) | Kinesin |
| Retrograde | Terminal → Soma | 100-200 mm/day | Old organelles, neurotrophic factors (NGF), viruses (herpes, tetanus toxin), endosomes | Dynein |
Clinical relevance:
- Retrograde transport used by rabies virus, herpes simplex virus, tetanus toxin to reach CNS
- Disrupted axonal transport → neurodegeneration (Alzheimer's, ALS)
- Nerve growth factor (NGF) reaches soma by retrograde transport → signals neuron survival
Q7. 🔵 LQ - Structure of Neuromuscular Junction (NMJ)
Definition: The NMJ (motor end plate) is the specialized chemical synapse between a motor neuron (alpha motor neuron) and a skeletal muscle fibre.
Structural Components:
Presynaptic (nerve terminal):
- Large myelinated axon (Aα fibre) loses myelin and branches
- Axon terminal: swollen knob-like ending lying in a groove on muscle surface
- Contains:
- ~300,000 synaptic vesicles (each ~50 nm diameter) filled with acetylcholine (ACh)
- Mitochondria (ATP for ACh synthesis)
- Active zones: linear dense bars where vesicles dock; flanked by voltage-gated Ca2+ channels
- Covered by Schwann cell cap
Synaptic Cleft:
- Width: 20-30 nm (narrower than CNS synapses)
- Contains acetylcholinesterase (AChE) - destroys ACh rapidly
Postsynaptic (motor end plate):
- Muscle membrane (sarcolemma) folded into junctional folds / subneural clefts (increase surface area)
- Mouths of folds contain high density of nicotinic ACh receptors (nAChR) - pentameric structure (2α + β + δ + ε)
- Deeper in folds: voltage-gated Na+ channels (trigger action potential)
- After denervation: nAChRs spread over whole muscle surface (supersensitivity)
Q8. 🔵 LQ - Neuromuscular Transmission
Sequence of Events:
Step 1: Action potential travels down the alpha motor neuron → reaches axon terminal
Step 2: Depolarization of terminal membrane → opens voltage-gated Ca2+ channels at active zones → Ca2+ flows into terminal
Step 3: Ca2+ binds to synaptotagmin on synaptic vesicles → interacts with SNARE proteins (synaptobrevin + syntaxin + SNAP-25) → vesicle-membrane fusion → exocytosis of ACh into cleft
- ~125 vesicles released per action potential
Step 4: ACh diffuses across the 20-30 nm cleft
Step 5: ACh binds to nicotinic nAChRs (two ACh molecules per receptor) → ion channel opens → large Na+ influx (+ some K+ efflux) → End Plate Potential (EPP)
- EPP is always suprathreshold (safety factor ~5) → always generates muscle AP
Step 6: Muscle action potential propagates along sarcolemma → T-tubules → triggers Ca2+ release from SR → muscle contraction
Step 7: ACh is rapidly hydrolysed by AChE in the cleft into choline + acetate → choline taken back up into terminal (choline transporter) → resynthesized into ACh by choline acetyltransferase (ChAT)
Drugs affecting NMJ:
| Drug | Action | Effect |
|---|---|---|
| Neostigmine, pyridostigmine | Inhibit AChE | Prolongs ACh action; used in myasthenia gravis |
| Succinylcholine | Depolarising NMJ blocker | Persistent depolarization → flaccid paralysis |
| Vecuronium, atracurium | Non-depolarising NMJ blocker | Competitive antagonist at nAChR → flaccid paralysis |
| Botulinum toxin | Cleaves SNARE proteins | Prevents ACh release → flaccid paralysis |
| Hemicholinium | Blocks choline reuptake | Depletes ACh |
| Organophosphates | Irreversible AChE inhibitors | Excess ACh → spastic paralysis |
Q9. 🟡 SQ - Myasthenia Gravis
Definition: An acquired autoimmune neuromuscular disease characterised by muscle weakness and fatigability due to antibody-mediated destruction of nicotinic ACh receptors at the NMJ.
Pathophysiology:
- Autoantibodies against nAChRs (mainly directed at the α-subunit's main immunogenic region - MIR) in 85% of cases
- Also anti-MuSK antibodies (muscle-specific kinase) in 15%
- Antibodies + complement → receptor destruction + loss of junctional folds → reduced EPP amplitude → fails to reach threshold → muscle weakness
- Thymus plays key role: thymic hyperplasia (young women) or thymoma (older men); thymic myoid cells express nAChR → site of sensitisation
Clinical Features:
- Muscle weakness that worsens with activity, improves with rest (fatigability)
- Ptosis and diplopia (most common initial symptoms - extraocular muscles most vulnerable)
- Dysphagia, dysarthria (bulbar symptoms)
- Limb weakness (proximal > distal)
- Respiratory muscle involvement → myasthenic crisis (respiratory failure - medical emergency)
- Bimodal peak: Young women (20s) + older men (60s)
Diagnosis:
- Tensilon (edrophonium) test: Short-acting AChE inhibitor → dramatic but brief improvement
- Anti-AChR antibody titre
- Single-fibre EMG (most sensitive)
- CT chest (thymoma)
- Repetitive nerve stimulation → decremental response
Treatment:
- Pyridostigmine (AChE inhibitor) - symptomatic
- Immunosuppression: Corticosteroids, azathioprine, mycophenolate
- Thymectomy (especially in thymoma; improves 75%)
- Plasmapheresis / IVIG - acute crises
Q10. 🔵 LQ - Molecular Basis of Muscle Contraction in Skeletal and Smooth Muscle
A. Skeletal Muscle Contraction (Sliding Filament Theory - Huxley & Hanson)
Sarcomere structure:
- Thick filaments: Myosin (heavy chains + light chains); myosin heads have ATPase activity and actin-binding sites
- Thin filaments: Actin (F-actin) + Tropomyosin (blocks myosin binding sites at rest) + Troponin complex (TnT - binds tropomyosin; TnI - inhibitory; TnC - binds Ca2+)
- Z lines: Anchor thin filaments
- M line: Anchor thick filaments
- Titin: Elastic protein, connects M line to Z line; gives passive elasticity
Resting state: Tropomyosin covers actin binding sites → no cross-bridge formation
Steps in Skeletal Muscle Contraction (Cross-Bridge Cycle):
- AP → T-tubule → SR → Ca2+ release (via ryanodine receptor RyR1)
- Ca2+ binds TnC → conformational change in troponin → tropomyosin moves away → exposes myosin-binding sites on actin
- Myosin head (with ADP+Pi) attaches to actin → cross-bridge formed
- Power stroke: Pi released → myosin head pivots (rotates ~45°) → pulls actin toward M-line → thin filaments slide → sarcomere shortens; ADP released
- ATP binds myosin → cross-bridge detaches (if no ATP → rigor mortis)
- ATP hydrolysis by myosin ATPase → myosin head returns to cocked (high-energy) position → ready for next cycle
- Relaxation: Ca2+ pumped back into SR by Ca2+-ATPase (SERCA) → TnC releases Ca2+ → tropomyosin re-covers binding sites
Net effect: Actin filaments slide inward → Z lines come closer → sarcomere shortens → muscle contracts
B. Smooth Muscle Contraction
- No troponin; regulation via calmodulin
- Thin filaments lack troponin-tropomyosin system
Steps:
- Ca2+ enters via voltage-gated channels (or released from SR via IP3-gated channels)
- Ca2+ binds calmodulin (4 Ca2+ per calmodulin)
- Ca2+-calmodulin activates myosin light chain kinase (MLCK)
- MLCK phosphorylates myosin light chain (MLC) → activates myosin ATPase
- Phosphorylated myosin cross-bridges with actin → contraction
- Relaxation: MLCK inactivated (when Ca2+ falls) + myosin light chain phosphatase (MLCP) dephosphorylates MLC → relaxation
Key difference - skeletal vs smooth:
| Feature | Skeletal | Smooth |
|---|---|---|
| Ca2+ regulation | Troponin-C | Calmodulin-MLCK |
| Speed | Fast | Slow |
| Voluntary control | Yes | No (autonomic) |
| Source of Ca2+ | SR (ryanodine RyR1) | SR + extracellular |
| Fatigue | Yes | Resistant |
| Latch state | No | Yes (sustained contraction with less ATP) |
Q11. 🟡 SQ - Differences Between Isometric and Isotonic Muscle Contraction
| Feature | Isometric Contraction | Isotonic Contraction |
|---|---|---|
| Definition | Muscle develops tension without change in length | Muscle changes length while tension remains constant |
| Length | Unchanged | Shortens (concentric) or lengthens (eccentric) |
| Tension | Increases | Remains constant |
| Work done | No external work (force × displacement = 0) | External work done |
| Energy used | Heat produced | Mechanical work + heat |
| Example | Pushing against a wall; holding a weight still | Lifting a dumbbell; walking |
| Joint movement | No movement | Movement occurs |
| Clinical use | Rehabilitation (strengthening without joint stress) | Functional movement training |
Types of isotonic:
- Concentric: Muscle shortens while generating force (lifting)
- Eccentric: Muscle lengthens while generating force (lowering weight slowly)
Q12. 🟡 SQ - Strength Duration Curve
Definition: A graphical representation of the relationship between the strength (intensity) of an electrical stimulus and the duration required to just excite (threshold stimulation) an excitable tissue (nerve or muscle).
Key Terms:
| Term | Definition |
|---|---|
| Rheobase | The minimum strength (intensity) of stimulus of infinitely long duration required to excite the tissue |
| Chronaxie | The minimum duration of a stimulus at twice the rheobase intensity required to excite the tissue |
| Utilization time | Minimum time needed for a stimulus at rheobase strength to excite the tissue |
The Curve:
- As stimulus duration increases, the threshold intensity (strength) decreases
- At very short durations: very high intensity needed
- At longer durations: only rheobase intensity needed (curve becomes flat = asymptote)
- The curve is hyperbolic in shape
Strength (I)
|
2xRheobase -----*
| |
Rheobase -------+-----------___________
| |
| |
+-------------+-----> Duration (t)
Chronaxie
Clinical Applications:
- Chronaxie of nerve (0.1-0.3 ms) < Chronaxie of muscle (1-10 ms) → At short durations, nerves are more excitable than muscles
- Denervated muscle: curve shifts right (higher chronaxie) - used to diagnose denervation
- Used in electrodiagnosis of nerve/muscle injury
- Basis of electrical stimulation protocols in physiotherapy
- Determines pacemaker pulse parameters
Sources: Guyton & Hall Textbook of Medical Physiology; Neuroscience: Exploring the Brain, 5th Ed; Histology: A Text and Atlas (Mescher); Medical Physiology (Boron & Boulpaep); Bailey & Love's Surgery
Ready to continue with Chapter 4: Digestive System whenever you say so!
Continue
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Chapter 4: Digestive System
Legend: 🔵 LQ = Long Question (10-15 marks) | 🟡 SQ = Short Question (5 marks)
Q1. 🔵 LQ - Composition, Functions and Regulation of Saliva, Gastric, Pancreatic, and Bile Secretion
A. Saliva
Production: ~1–1.5 litres/day | Produced by parotid (serous), submandibular (mixed), sublingual (mainly mucous) glands
Composition:
- Water (99.5%), electrolytes (Na+, K+, Cl-, HCO3-)
- Salivary amylase (ptyalin): Begins starch digestion (cleaves α-1,4 glycosidic bonds)
- Mucin (mucus): Lubrication, bolus formation
- Lysozyme + IgA: Antibacterial protection
- Lingual lipase: Minor fat digestion
- pH: 6.2-7.4
Functions:
- Lubrication for chewing and swallowing (mucin)
- Initiates carbohydrate digestion (amylase)
- Dissolves food substances to enable taste
- Antimicrobial (lysozyme, IgA, lactoferrin)
- Dental hygiene (HCO3- neutralises acids, fluoride)
- Speech facilitation
- Excretion of urea, drugs (e.g., iodine, mercury)
Regulation:
- Neural (only) - no hormonal regulation
- Parasympathetic (dominant): Via chorda tympani (CN VII) and glossopharyngeal (CN IX) → ACh → muscarinic receptors → profuse watery saliva
- Sympathetic: Via cervical ganglia → NA → α receptors → thick, mucus-rich saliva
- Stimuli: Taste, smell, sight of food (conditioned reflex), chewing, nausea; inhibited by dehydration, sleep, fear
B. Gastric Secretion
Volume: ~2.5 litres/day | pH: 1.5-2.0 (HCl secreted)
Cells and Their Secretions:
| Cell | Location | Secretion |
|---|---|---|
| Parietal cells (oxyntic) | Fundus/body glands | HCl + Intrinsic Factor |
| Chief cells (peptic) | Fundus/body glands | Pepsinogen (→ Pepsin by HCl) + Gastric lipase |
| G cells | Antrum | Gastrin |
| D cells | Antrum + throughout | Somatostatin (inhibitory) |
| ECL cells | Fundus | Histamine (stimulated by gastrin) |
| Mucous neck cells | Gland neck | Mucus + HCO3- (mucosal protection) |
Mechanism of HCl Secretion (Parietal Cell):
- H+/K+-ATPase (proton pump) on apical membrane → pumps H+ into lumen in exchange for K+
- Stimulated by: Histamine (H2 receptors → cAMP), Gastrin (CCK-B receptors → Ca2+), ACh (M3 receptors → Ca2+)
- These three are synergistic → blocking one (e.g., H2 blocker) greatly reduces secretion
Phases of Gastric Secretion:
| Phase | Trigger | Mechanism | % of Total |
|---|---|---|---|
| Cephalic | Sight, smell, thought, taste of food | Vagus nerve → ACh → parietal cells + G cells | 30% |
| Gastric | Food in stomach, distension, proteins | Local reflexes + gastrin release | 60% |
| Intestinal | Chyme in duodenum (early stimulation, then inhibition) | Duodenal gastrin (stimulates); Secretin, CCK, GIP (inhibit) | 10% |
Inhibition of gastric secretion: Low pH in antrum (<2) inhibits G cells; secretin, GIP, CCK suppress acid secretion (enterogastric reflex)
C. Pancreatic Secretion
Volume: ~1,500 mL/day | pH: 8.0 (highly alkaline due to HCO3-)
Composition:
- Water + Electrolytes: High HCO3- (113 mEq/L vs 24 mEq/L plasma) - neutralises gastric acid in duodenum
- Enzymes (in zymogen granules):
| Enzyme | Precursor | Activated by | Substrate |
|---|---|---|---|
| Trypsin | Trypsinogen | Enterokinase (brush border) | Proteins |
| Chymotrypsin | Chymotrypsinogen | Trypsin | Proteins |
| Elastase | Proelastase | Trypsin | Proteins |
| Carboxypeptidase | Procarboxypeptidase | Trypsin | Proteins |
| Pancreatic lipase | Active | - | Triglycerides (with co-lipase) |
| Phospholipase A2 | Prophospholipase | Trypsin | Phospholipids |
| Pancreatic amylase | Active | - | Starch |
| DNase/RNase | Active | - | Nucleic acids |
Protection against autodigestion:
- Enzymes secreted as zymogens (inactive)
- Trypsin inhibitor secreted with juice
- Enterokinase (not in pancreas) activates trypsinogen only in duodenum
- In acute pancreatitis: premature activation of enzymes → autodigestion
Regulation:
- Secretin (S cells of duodenum; stimulus: low pH < 4.5 in duodenum) → ↑ HCO3- and water secretion (ductal cells)
- CCK (I cells of duodenum; stimulus: fatty acids, amino acids) → ↑ enzyme secretion (acinar cells)
- Vagus nerve (ACh): Stimulates both components (cephalic phase)
D. Bile Secretion
Production: 500-1,000 mL/day by hepatocytes | Stored and concentrated (5-20x) in gallbladder
Composition:
| Component | Function |
|---|---|
| Bile salts (bile acids) | Emulsify fats; form micelles for fat absorption |
| Bilirubin (conjugated) | Excretion of haem breakdown product; gives bile yellow colour |
| Cholesterol | Excretion route; precursor of bile acids |
| Phospholipids (lecithin) | Emulsification; keep cholesterol in solution |
| Water + electrolytes | HCO3- rich |
| Mucus | Protection |
Primary bile acids: Cholic acid, Chenodeoxycholic acid (made in liver from cholesterol)
Secondary bile acids: Deoxycholic acid, Lithocholic acid (formed by gut bacteria)
Bile salts: Conjugated with glycine or taurine to increase water solubility
Enterohepatic Circulation:
- 95% of bile salts reabsorbed in terminal ileum → portal vein → liver → re-secreted
- Only 5% lost in faeces → replaced by new synthesis from cholesterol
- Total bile salt pool: ~3 g, circulates 6-10 times/day
Regulation of Bile Release:
- CCK: Released by fat and proteins in duodenum → contracts gallbladder + relaxes sphincter of Oddi → bile flows into duodenum
- Secretin: Increases HCO3- secretion from bile ducts
- Vagus nerve: Stimulates gallbladder contraction
- Fasting: Sphincter of Oddi closed → bile stored in gallbladder
Functions of Bile:
- Emulsification of dietary fats (essential for fat digestion and absorption)
- Micellar solubilisation → absorption of fat-soluble vitamins (A, D, E, K)
- Excretion of bilirubin, cholesterol, heavy metals, drugs
- Neutralisation of gastric acid
- Bacteriostatic effect
Q2. 🟡 SQ - Movements of Small Intestine and Large Intestine
Small Intestinal Movements:
| Movement | Description | Function |
|---|---|---|
| Segmentation (mixing contractions) | Ring-like non-propulsive contractions at intervals; most common | Mixes chyme with digestive juices; increases contact with mucosa |
| Peristalsis | Coordinated wave of contraction and relaxation moving aborally | Propels chyme towards large intestine; Law of intestine |
| Migrating Motor Complex (MMC) | Cyclic contractions during fasting (every 90 min); "housekeeper waves" | Clears residual food, bacteria, debris between meals |
| Pendular movements | Swaying oscillation of intestinal segment | Mixes contents |
| Villi movements | Villus contraction and shortening (controlled by villikidin hormone) | Pumps lymph from lacteals; aids absorption |
Control: Myenteric plexus (Auerbach) is the primary controller; ACh (promotes) and Sympathetic NA (inhibits)
Large Intestinal Movements:
| Movement | Description | Function |
|---|---|---|
| Haustral churning (segmentation) | Slow back-and-forth movement in haustra | Mixing and absorption of water and electrolytes |
| Peristalsis | Slow, weak propulsion | Moves contents forward |
| Mass movements (mass peristalsis) | Strong, powerful propulsion of large segments; 1-3 times/day | Moves faeces toward rectum; triggered by gastrocolic reflex after meals |
Gastrocolic reflex: Distension of stomach after meal → reflex stimulation of colon → mass movements → urge to defaecate
Q3. 🟡 SQ - Deglutition (Swallowing) and Defaecation Reflex
A. Deglutition (Swallowing)
Three stages:
Stage 1 - Oral (Voluntary):
- Food chewed, mixed with saliva → bolus formed
- Tongue pushes bolus backward against hard palate into pharynx
- Voluntary, under conscious control
Stage 2 - Pharyngeal (Involuntary, Reflex):
- Swallowing centre in medulla oblongata activated
- Coordinated reflexes in <1 second:
- Soft palate elevates (closes nasopharynx)
- Larynx elevates and epiglottis closes (prevents aspiration)
- Vocal cords adduct (close glottis)
- Respiration momentarily inhibited
- Upper oesophageal sphincter relaxes
- Peristaltic wave carries bolus into oesophagus
- Involuntary, cannot be stopped once initiated
- Cranial nerves involved: V, VII, IX, X, XII
Stage 3 - Oesophageal (Involuntary):
- Primary peristalsis: Continuation of pharyngeal wave pushes bolus down oesophagus
- Secondary peristalsis: Triggered by distension if bolus remains; clears residue
- Lower oesophageal sphincter (LOS) relaxes to allow bolus into stomach
- Duration: ~8-10 seconds for solids; faster for liquids
B. Defaecation Reflex
Mechanism:
- Mass movements push faeces into rectum
- Rectal wall distension → stretch receptors activated
- Intrinsic reflex (via myenteric plexus): Peristaltic waves in descending colon + internal anal sphincter relaxes
- Parasympathetic reflex (via S2-S4 sacral cord): Amplifies peristalsis, further relaxes internal anal sphincter
- If conditions appropriate: voluntary relaxation of external anal sphincter (under somatic control via pudendal nerve) → defaecation
- Valsalva manoeuvre: Closure of glottis + contraction of abdominal muscles → raises intra-abdominal pressure → assists defaecation
Voluntary control: External anal sphincter (skeletal muscle) can contract to delay defaecation until appropriate
Q4. 🔵 LQ - Digestion and Absorption of Nutrients
A. Carbohydrates
Digestion:
- Mouth: Salivary amylase → cleaves starch at α-1,4 bonds → dextrins, maltose (inactivated by gastric acid)
- Small intestine: Pancreatic amylase → oligosaccharides, disaccharides
- Brush border enzymes: Maltase, sucrase, lactase → monosaccharides (glucose, fructose, galactose)
Absorption:
- Glucose and galactose: SGLT1 (Na+-glucose cotransporter) - active, secondary active transport
- Fructose: GLUT5 (facilitated diffusion)
- All exit basolateral membrane via GLUT2 into portal blood
Lactase deficiency → undigested lactose fermented by bacteria → gas, bloating, osmotic diarrhoea
B. Proteins
Digestion:
- Stomach: Pepsin (activated from pepsinogen by HCl; pH < 2) → polypeptides + some amino acids
- Small intestine: Trypsin, chymotrypsin, elastase, carboxypeptidase → oligopeptides + amino acids
Absorption:
- Amino acids: Carrier-mediated active transport (Na+-amino acid cotransporters) at brush border
- Di- and tri-peptides: PepT1 transporter → hydrolysed inside enterocytes
- Exit basolateral membrane via facilitated diffusion → portal blood
C. Fats (Lipids)
Digestion:
- Lingual + gastric lipase: minor initial hydrolysis
- Emulsification by bile salts: Large fat globules → tiny droplets (increases surface area)
- Pancreatic lipase + co-lipase: Hydrolyses triglycerides → monoglycerides + free fatty acids (FFAs)
- Micelle formation: Bile salts wrap around monoglycerides + FFAs → mixed micelles
Absorption:
- Micelles carry lipids to brush border membrane
- Monoglycerides + FFAs diffuse passively into enterocytes
- Inside enterocytes: re-esterified to triglycerides → combined with phospholipids + cholesterol + apolipoproteins → chylomicrons
- Chylomicrons secreted by exocytosis → lacteals (lymph) → thoracic duct → subclavian vein → systemic circulation
Fat-soluble vitamins (A, D, E, K): Absorbed with fat via micelles; malabsorbed in bile duct obstruction or fat malabsorption
Short- and medium-chain fatty acids: Absorbed directly into portal blood (do not need micelles)
D. Water and Electrolytes
- ~9 litres enters GI tract daily (food + secretions); only ~100-200 mL excreted in stool
- Most water absorbed in small intestine (osmotically following solute absorption)
- Na+ absorbed by: Na+-glucose/amino acid cotransport; Na+-H+ exchange; electrogenic Na+ channels (colon)
- Cl- absorbed by Cl--HCO3- exchange
- Iron: Absorbed as Fe2+ in duodenum; regulated by hepcidin; transferrin carries it in blood
- Calcium: Absorbed actively in duodenum (calbindin, vitamin D-regulated) and passively throughout
- Vitamin B12: Binds intrinsic factor (from parietal cells) → absorbed in terminal ileum
Q5. 🟡 SQ - GI Hormones and Their Actions
| Hormone | Source | Cell | Stimulus | Actions |
|---|---|---|---|---|
| Gastrin | Stomach antrum, duodenum | G cells | Vagal stimulation, gastric distension, amino acids, hypercalcaemia | ↑ HCl secretion (parietal); ↑ pepsinogen (chief); ↑ gastric motility; mucosal growth; ↑ intrinsic factor |
| Cholecystokinin (CCK) | Duodenum, jejunum | I cells | Fatty acids, amino acids in duodenum | Gallbladder contraction; ↑ pancreatic enzyme secretion; relaxes sphincter of Oddi; ↓ gastric emptying; satiety signal |
| Secretin | Duodenum, jejunum | S cells | Low pH (< 4.5) in duodenum; fatty acids | ↑ Pancreatic HCO3- + water; ↑ biliary HCO3-; ↓ gastric acid; ↓ gastric motility |
| GIP (Glucose-dependent Insulinotropic Peptide) | Duodenum, jejunum | K cells | Glucose, fat, protein | ↑ Insulin secretion; ↓ gastric acid; enterogastrone |
| Motilin | Duodenum, jejunum | Mo cells | Fasting, alkalinisation | Triggers MMC (housekeeper waves) during fasting; used clinically as erythromycin |
| Somatostatin | Stomach, pancreas, duodenum | D cells | Fat, protein, acid, CCK | Inhibits all GI hormones; ↓ gastric acid; ↓ pancreatic secretion; ↓ bile; ↓ motility; ↓ splanchnic blood flow |
| VIP (Vasoactive Intestinal Peptide) | GI neurons | — | Neural | ↑ Intestinal secretion; ↓ gastric acid; vasodilator; smooth muscle relaxation |
| Neurotensin | Ileum | N cells | Fat | ↑ Pancreatic secretion; ↑ intestinal motility; ↓ gastric secretion; trophic |
| Glucagon-like peptide-1 (GLP-1) | Ileum, colon | L cells | Fat, carbohydrate | ↑ Insulin; ↓ glucagon; slows gastric emptying; satiety (target of GLP-1 analogues in diabetes) |
Q6. 🟡 SQ - Gut-Brain Axis
Definition: The gut-brain axis is the bidirectional communication network between the gastrointestinal tract and the central nervous system, involving neural, hormonal, immunological, and microbial pathways.
Components:
- Central Nervous System (CNS): Brain + spinal cord; processes emotions, stress, cognition
- Enteric Nervous System (ENS): "Second brain" - 200-500 million neurons in Meissner (submucosal) and Auerbach (myenteric) plexuses; functions independently but communicates with CNS
- Autonomic Nervous System: Vagus nerve (80% afferent) is the main highway; sympathetic fibres
- HPA Axis (Hypothalamic-Pituitary-Adrenal): Stress hormones (cortisol) affect gut permeability and microbiome
- Gut Microbiome: Trillions of bacteria produce neurotransmitters (GABA, serotonin, short-chain fatty acids) that signal to brain
- Enteroendocrine cells: Release hormones (serotonin, CCK, GLP-1) that signal via vagus to brain
Key Signalling Molecules:
- Serotonin (5-HT): 95% of body's serotonin made in gut (enterochromaffin cells); regulates motility and mood
- Short-chain fatty acids (SCFAs): Made by gut bacteria; influence BBB integrity, glial function, neuroinflammation
- GABA: Produced by Lactobacillus; may reduce anxiety
Clinical Significance:
- IBS (Irritable Bowel Syndrome): Bidirectional dysfunction; stress worsens symptoms
- Depression/Anxiety: Gut dysbiosis linked to mental health disorders
- Parkinson's disease: α-synuclein pathology may start in ENS before brain
- Autism Spectrum Disorder: GI symptoms common; microbiome differences noted
- Probiotics targeting gut-brain axis being studied for psychiatric conditions
Q7. 🟡 SQ - Functions of Liver and Gallbladder
Functions of the Liver:
1. Metabolic Functions:
- Carbohydrate: Glycogen synthesis (glycogenesis), breakdown (glycogenolysis), gluconeogenesis; maintains blood glucose
- Protein: Synthesis of all plasma proteins except immunoglobulins (albumin, globulins, fibrinogen, coagulation factors, complement); urea synthesis (detoxifies NH3)
- Fat: Fatty acid oxidation (β-oxidation); ketone body synthesis; lipoprotein synthesis (VLDL, HDL); cholesterol synthesis and conversion to bile acids
2. Secretory/Excretory:
- Bile secretion (500-1000 mL/day)
- Bilirubin conjugation and excretion
- Excretion of drugs, heavy metals, hormones
3. Detoxification:
- Drug metabolism (CYP450 enzymes - Phase I: oxidation, reduction; Phase II: conjugation)
- Detoxification of ammonia → urea (urea cycle)
- Inactivation of hormones (oestrogen, aldosterone, insulin)
- Kupffer cells (liver macrophages): phagocytose bacteria from portal blood
4. Haematological:
- Synthesis of coagulation factors (I, II, V, VII, IX, X, XI, XII) and anticoagulants (Protein C, S, antithrombin)
- Site of foetal haemopoiesis
- Stores iron, vitamin B12, fat-soluble vitamins (A, D, E, K), copper
5. Immunological:
- Kupffer cells: phagocytose antigens from gut
- Synthesis of complement proteins and acute phase proteins
6. Endocrine:
- Produces IGF-1 (in response to GH)
- Converts T4 → T3
- Activates vitamin D (25-hydroxylation)
- Degrades hormones
Functions of the Gallbladder:
- Storage of bile (40-70 mL capacity)
- Concentration of bile (5-20 times) - absorbs water, Na+, Cl-
- Controlled release via CCK → gallbladder contraction + sphincter of Oddi relaxation
- Acidification of bile → precipitates calcium salts (prevents bile duct stones)
- Mucus secretion protects gallbladder wall
Q8. 🔵 LQ - Pathophysiology: Peptic Ulcer, GORD, Vomiting, Diarrhoea, Adynamic Ileus, Hirschsprung's Disease
A. Peptic Ulcer Disease (PUD)
Definition: Break in the gastroduodenal mucosa exposing submucosa, due to imbalance between aggressive (acid, pepsin, H. pylori, NSAIDs) and protective (mucus, HCO3-, prostaglandins, mucosal blood flow) factors.
Causes:
- H. pylori (70-80% of duodenal ulcers; 60% gastric) - disrupts mucus barrier
- NSAIDs - inhibit COX-1 → ↓ prostaglandins → ↓ mucus + HCO3- + mucosal blood flow
- Zollinger-Ellison syndrome - gastrinoma → massive hypersecretion of HCl
Features: Burning epigastric pain (DU relieved by food; GU worsened by food), nausea, bloating
Complications: Bleeding, perforation, obstruction, malignant transformation (GU)
Treatment: PPIs (omeprazole - inhibit H+/K+-ATPase), H2 blockers (ranitidine), H. pylori eradication (triple therapy), misoprostol (prostaglandin analogue for NSAID ulcers)
B. Gastro-Oesophageal Reflux Disease (GORD)
Pathophysiology: Failure of lower oesophageal sphincter (LOS) → acidic gastric contents reflux into oesophagus
- LOS normally maintained at 15-25 mmHg above gastric pressure
- Causes of LOS failure: fatty meals, alcohol, smoking, hiatus hernia, obesity, pregnancy, drugs (nitrates, CCBs)
- Repeated exposure to acid → oesophagitis → Barrett's oesophagus (metaplastic columnar epithelium replaces squamous) → risk of adenocarcinoma
Features: Heartburn, regurgitation, water brash, dysphagia
Treatment: Lifestyle modification, PPIs, antacids; surgical (Nissen fundoplication)
C. Vomiting
Definition: Forceful expulsion of gastric contents through the mouth, coordinated by the vomiting centre in the medulla (nucleus tractus solitarius region).
Pathways:
- Chemoreceptor Trigger Zone (CTZ): Area postrema (floor of 4th ventricle), outside BBB → detects toxins, drugs (morphine, chemotherapy), metabolic disturbances
- Vestibular apparatus (CN VIII): Motion sickness
- GI vagal afferents: Distension, irritants, gastroenteritis
- Higher CNS: Emotional, visual, olfactory triggers
Sequence of events:
- Nausea → hypersalivation (alkaline saliva neutralises acid)
- Deep inspiration → glottis closes
- Pylorus contracts, LOS relaxes
- Violent contraction of diaphragm + abdominal muscles → ↑ intragastric pressure → gastric contents expelled
Consequences of prolonged vomiting: Metabolic alkalosis (loss of HCl), hypokalaemia, dehydration
Antiemetics: Ondansetron (5-HT3 blocker), metoclopramide (D2 blocker), promethazine (H1 blocker), cyclizine
D. Diarrhoea
Definition: Passage of > 3 loose/watery stools per day or > 200g/day of stool.
Mechanisms:
| Type | Mechanism | Features | Stops with fasting? | Examples |
|---|---|---|---|---|
| Secretory | Active Cl- secretion into lumen (cAMP/cGMP mediated) | Large volume, watery; normal osmolar gap | No | Cholera (CT → ↑ cAMP), VIPoma |
| Osmotic | Non-absorbable solutes draw water into lumen | Stops with fasting; ↑ osmolar gap | Yes | Lactase deficiency, lactulose, Mg salts |
| Motility | Rapid transit → reduced absorption time | Variable | — | IBS, post-vagotomy, hyperthyroidism |
| Exudative/Inflammatory | Mucosal damage → protein + blood + pus | Blood/mucus in stool | No | IBD, dysentery, infectious colitis |
E. Adynamic (Paralytic) Ileus
Definition: Failure of normal intestinal peristalsis in the absence of mechanical obstruction, resulting in intestinal distension and inability to pass flatus/faeces.
Causes:
- Post-operative (most common) - handling of bowel triggers reflex inhibition
- Electrolyte imbalance (especially hypokalaemia)
- Retroperitoneal haematoma/inflammation (pancreatitis)
- Peritonitis, sepsis
- Drugs (opioids, anticholinergics)
- Spinal cord injury
Features: Abdominal distension, absent bowel sounds, constipation, nausea; X-ray shows gas-filled loops of bowel throughout
Treatment: Treat underlying cause; NBM; nasogastric tube; IV fluids; correct electrolytes; early mobilisation; neostigmine (refractory cases)
F. Hirschsprung's Disease (Congenital Megacolon)
Definition: Congenital absence of ganglion cells (myenteric and submucosal plexuses) in the distal colon, causing failure of peristalsis in the affected segment.
Pathophysiology:
- Failure of neural crest cell migration during embryonic development
- Aganglionic segment (always includes internal anal sphincter, extends proximally variable distance) → cannot relax → functional obstruction
- Proximal colon distends → megacolon
Genetics: Associated with RET proto-oncogene mutations; commoner in males
Features:
- Failure to pass meconium within 48 hours of birth (cardinal feature)
- Abdominal distension, bilious vomiting
- Explosive passage of faeces when PR exam performed (classic sign)
- Can present in older children as chronic constipation
Diagnosis: Rectal biopsy (absence of ganglion cells) - gold standard; barium enema shows transition zone; anorectal manometry
Treatment: Surgical - removal of aganglionic segment + pull-through procedure (Swenson, Soave, or Duhamel)
Sources: Ganong's Review of Medical Physiology 26th Ed; Mulholland & Greenfield's Surgery 7th Ed; Bailey & Love's Surgery 28th Ed; Yamada's Textbook of Gastroenterology
Ready to continue with Chapter 5: Cardiovascular System whenever you say so!
Continue
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Chapter 5: Cardiovascular System
Legend: 🔵 LQ = Long Question (10-15 marks) | 🟡 SQ = Short Question (5 marks)
Q1. 🔵 LQ - Conducting System of the Heart
The conducting system consists of specialised cardiac muscle cells that generate and transmit electrical impulses to coordinate the rhythmic contraction of the heart.
Components (in order of impulse travel):
1. Sinoatrial Node (SA Node) - The Pacemaker
- Location: Posterior wall of right atrium, near opening of superior vena cava, in the sulcus terminalis (Keith-Flack node)
- Size: ~10 mm long, spindle-shaped
- Intrinsic rate: 60-100 beats/min (dominant pacemaker)
- Function: Generates the cardiac impulse; sets heart rate
- Cell type: Nodal cells with unstable resting potential (pacemaker potential - "funny current" If); spontaneous diastolic depolarisation via slow Na+ influx then Ca2+ influx
- Blood supply: SA nodal artery (from RCA in 60%, LCX in 40%)
2. Internodal Pathways (Atrial Conduction)
- Three bundles transmit impulse from SA node to AV node:
- Anterior internodal tract (Bachmann's bundle) - also conducts to left atrium
- Middle internodal tract (Wenckebach)
- Posterior internodal tract (Thorel)
- Conduction velocity: ~1 m/s through atrial myocardium
- Causes P wave on ECG
3. Atrioventricular Node (AV Node)
- Location: Inferior interatrial septum, above coronary sinus opening, between tricuspid valve and coronary sinus (Aschoff-Tawara node)
- Size: ~5 mm long
- Intrinsic rate: 40-60 beats/min
- KEY FUNCTION: Introduces a delay of ~0.1 second between atrial and ventricular contraction (allows ventricles to fill completely before contracting)
- Conduction velocity: 0.05 m/s (slowest in the conducting system)
- Responsible for PR interval on ECG (0.12-0.20 s)
- Blood supply: AV nodal artery (from RCA in 90%)
- Site of AV block pathology
4. Bundle of His (Atrioventricular Bundle)
- Originates at AV node; penetrates fibrous skeleton of heart
- Only electrical connection between atria and ventricles (fibrous skeleton normally insulates them)
- Divides into right and left bundle branches at top of interventricular septum
5. Right and Left Bundle Branches
- Travel subendocardially down both sides of interventricular septum
- Right bundle branch: Single compact bundle to right ventricle
- Left bundle branch: Fans out into anterior and posterior fascicles to left ventricle
- Bundle branch block produces wide QRS complex on ECG
6. Purkinje Fibres (Subendocardial branches)
- Location: Spread throughout subendocardial surface of both ventricles
- Intrinsic rate: 25-40 beats/min (lowest; ventricular escape rhythm)
- Fastest conduction: 2-4 m/s
- Stimulate ventricular myocardium from apex upward → coordinated contraction ("wringing" motion)
- Responsible for QRS complex on ECG
Summary Table:
| Structure | Location | Intrinsic Rate | Conduction Velocity | ECG |
|---|---|---|---|---|
| SA Node | RA near SVC | 60-100/min | 0.05 m/s (nodal) | P wave |
| AV Node | Interatrial septum | 40-60/min | 0.05 m/s | PR interval |
| Bundle of His | IV septum | 40-60/min | 1 m/s | — |
| Bundle Branches | IV septum | 40-60/min | 2-4 m/s | — |
| Purkinje Fibres | Subendocardium | 25-40/min | 2-4 m/s | QRS |
Clinical Correlations:
- SA node disease: Sick sinus syndrome, sinus bradycardia/tachycardia
- 1st degree AV block: Prolonged PR interval (> 0.20 s)
- 2nd degree AV block: Some P waves not conducted (Mobitz I - Wenckebach; Mobitz II)
- 3rd degree (complete) AV block: No P waves conducted to ventricles; ventricular escape rhythm
- Bundle branch block: Wide QRS (> 0.12 s) - LBBB or RBBB
Q2. 🟡 SQ - Properties of Cardiac Muscle
Cardiac muscle has unique properties that distinguish it from skeletal and smooth muscle:
1. Autorhythmicity (Automaticity)
- Cardiac muscle generates its own impulses without external neural input
- Due to unstable resting membrane potential (pacemaker potential) in nodal cells
- "Funny current" (If) - slow Na+ influx → gradual depolarisation → threshold → spontaneous AP
- SA node dominates due to highest intrinsic rate (overdrive suppression of lower centres)
2. Conductivity
- Impulse spreads rapidly across cardiac muscle via gap junctions (intercalated discs)
- Intercalated discs contain: desmosomes (structural) + gap junctions/connexons (electrical coupling)
- Heart behaves as a functional syncytium (all-or-none contraction of the whole heart)
3. Contractility (Inotropy)
- Strength of contraction depends on intracellular Ca2+ concentration
- Regulated by: SNS (↑), PSNS (↓ in atria), Frank-Starling mechanism, drugs (digoxin ↑, β-blockers ↓)
- Cardiac muscle cannot go onto descending limb of length-tension curve under physiological conditions
4. Rhythmicity
- Heart beats regularly and rhythmically under SA node control
- Rhythm is maintained precisely; arrhythmias = abnormal rhythms
5. Excitability
- Responds to adequate stimulation with an AP
- Absolute refractory period is very long (250-300 ms) - nearly as long as the contraction itself
- This prevents tetanic contraction (which would be fatal)
- All-or-None Law: Cardiac muscle either contracts fully or not at all (for a given physiological state)
6. Tonicity (Tonus)
- Heart maintains slight resting tone; never completely relaxes (unlike smooth muscle)
Cardiac AP vs Skeletal Muscle AP:
| Feature | Cardiac Muscle | Skeletal Muscle |
|---|---|---|
| Duration of AP | 200-300 ms | 1-2 ms |
| Plateau phase | Yes (phase 2, Ca2+ influx) | No |
| Refractory period | Long (prevents tetany) | Short |
| Source of Ca2+ | SR + extracellular (Ca2+-induced Ca2+ release) | SR only |
| Pacemaker potential | SA/AV nodes only | None |
Q3. 🔵 LQ - Cardiac Cycle
Definition: The sequence of mechanical and electrical events occurring during one complete heartbeat, from the beginning of one contraction to the beginning of the next. At 75 bpm, one cycle = 0.8 seconds.
Phases of the Cardiac Cycle:
Phase 1 - Ventricular Filling (Diastole) - 0.5 sec
(a) Rapid filling (early diastole):
- AV valves (mitral, tricuspid) open → blood rushes from atria into relaxed ventricles
- Accounts for ~70% of ventricular filling
- Produces S3 sound in some conditions (pathological in adults >40)
(b) Slow filling / Diastasis (mid-diastole):
- Continued gradual filling; pressures equalise
- ECG: P wave begins at end of this phase
(c) Atrial contraction ("atrial kick") (late diastole):
- Atria contract (P wave on ECG) → final 20-30% of ventricular filling
- End-Diastolic Volume (EDV) = 120-130 mL
- Loss of atrial kick (e.g., AF) reduces CO by up to 30%
Phase 2 - Isovolumetric Contraction (0.05 sec)
- Ventricles start contracting (QRS on ECG)
- AV valves close → S1 heart sound ("lub")
- Ventricular pressure rises rapidly but all valves closed → no change in volume
- This phase ends when ventricular pressure exceeds aortic/pulmonary pressure → semilunar valves open
Phase 3 - Ventricular Ejection (0.3 sec)
(a) Rapid ejection (early systole):
- Aortic and pulmonary valves open; blood ejected rapidly
- Peak ventricular pressure: left ~120 mmHg, right ~25 mmHg
(b) Slow ejection (late systole):
- Ventricular volume decreases; ejection continues
- End-Systolic Volume (ESV) = ~50 mL
- Stroke Volume = EDV - ESV = 120 - 50 = 70 mL
- Ejection Fraction (EF) = SV/EDV = 70/120 = ~58% (normal >55%)
Phase 4 - Isovolumetric Relaxation (0.08 sec)
- Ventricles relax → pressure falls below aortic/pulmonary → semilunar valves close → S2 heart sound ("dub")
- All valves closed → ventricular pressure falls rapidly with no change in volume
- Ends when ventricular pressure falls below atrial pressure → AV valves open → new cycle begins
Summary of Cardiac Cycle:
Diastole (filling) → Isovolumetric Contraction → Ejection (Systole) → Isovolumetric Relaxation
S1 (AV closes) S2 (Semilunar closes)
Wiggers Diagram (pressure-volume events at a glance):
| Event | ECG | Heart Sound | Valves |
|---|---|---|---|
| Atrial contraction | P wave | (A4) | AV open |
| Isovolumetric contraction | QRS | S1 | AV closes |
| Rapid ejection | ST segment | — | Semilunar opens |
| Slow ejection | T wave | — | Semilunar open |
| Isovolumetric relaxation | After T | S2 | Semilunar closes |
| Rapid filling | — | (S3) | AV opens |
Q4. 🔵 LQ - Electrocardiogram (ECG)
Definition: A graphical recording of the electrical activity (action potentials) of the heart as recorded from the body surface.
Standard ECG Waves and Intervals:
| Wave/Interval | Represents | Normal Duration |
|---|---|---|
| P wave | Atrial depolarisation (SA node → atria) | < 0.12 s; amplitude < 2.5 mm |
| PR interval | Conduction from SA node → ventricular muscle (AV node delay) | 0.12-0.20 s |
| QRS complex | Ventricular depolarisation | 0.06-0.10 s (< 0.12 s) |
| ST segment | Plateau of ventricular AP (isovolumetric contraction + ejection) | Isoelectric (on baseline) |
| T wave | Ventricular repolarisation | Positive in most leads |
| QT interval | Total ventricular electrical activity (depolarisation + repolarisation) | 0.36-0.44 s (rate-corrected QTc) |
| U wave | Purkinje fibre repolarisation (or papillary muscle) | Small, follows T |
Note: Atrial repolarisation (Ta) is hidden within the QRS complex.
Standard Leads:
Limb leads (frontal plane):
- Bipolar: I (RA-LA), II (RA-LF), III (LA-LF)
- Augmented unipolar: aVR, aVL, aVF
- Einthoven's triangle: Leads I, II, III form a triangle; Lead I + aVF used for axis determination
Precordial (chest) leads (horizontal plane):
- V1-V6: right to left across precordium
Normal cardiac axis: -30° to +90° (QRS predominantly positive in I and aVF)
Clinical Applications:
| ECG Change | Clinical Significance |
|---|---|
| Wide P wave (> 0.12 s) | Left atrial enlargement (P mitrale) |
| Tall peaked P wave | Right atrial enlargement (P pulmonale) |
| Prolonged PR | AV block (1st degree) |
| Short PR + delta wave | Wolff-Parkinson-White (WPW) syndrome |
| Wide QRS (> 0.12 s) | Bundle branch block, ventricular beats |
| ST elevation | Acute MI (STEMI), pericarditis |
| ST depression | Ischaemia, posterior MI, digoxin effect |
| T wave inversion | Ischaemia, ventricular hypertrophy, PE |
| Prolonged QTc | Risk of torsades de pointes (drugs, hypokalaemia, congenital) |
| Delta wave | Pre-excitation (WPW) |
Q5. 🔵 LQ - Blood Pressure: Definition, Factors Regulating It, Hypertension, Hypotension
Definition
Blood Pressure (BP): The lateral pressure exerted by the blood on the walls of the blood vessel per unit area. Measured in mmHg.
- Systolic BP (SBP): Peak pressure during ventricular systole. Normal: 100-120 mmHg
- Diastolic BP (DBP): Lowest pressure during ventricular diastole. Normal: 60-80 mmHg
- Pulse pressure = SBP - DBP = ~40 mmHg
- Mean Arterial Pressure (MAP) = DBP + 1/3 pulse pressure ≈ 93 mmHg
MAP = Cardiac Output × Total Peripheral Resistance
Factors Regulating Blood Pressure:
A. Short-term Regulation (seconds to minutes):
1. Baroreceptor Reflex (most important):
- Location: Carotid sinus (CN IX) + Aortic arch (CN X)
- ↑ BP → stretch baroreceptors → ↑ firing → vasomotor centre in medulla → ↓ sympathetic + ↑ parasympathetic → ↓ HR + ↓ SVR → BP falls back
- ↓ BP → reverse (baroreceptors inhibited → sympathetic activation)
- Reset upward in hypertension (baroreceptor "resetting")
2. Chemoreceptor Reflex:
- Peripheral (carotid + aortic bodies): ↓ pO2, ↑ pCO2, ↓ pH → vasoconstriction + ↑ HR
- Central (medullary): ↑ CO2/H+ → ↑ sympathetic → ↑ BP
3. CNS Ischaemic Response (Cushing Reflex):
- Extreme ↑ intracranial pressure → brain ischaemia → massive sympathetic discharge → severe hypertension (last-resort BP defence)
B. Intermediate Regulation (minutes to hours):
4. Renin-Angiotensin-Aldosterone System (RAAS):
- ↓ BP/renal perfusion → juxtaglomerular cells release renin → angiotensinogen → angiotensin I → ACE → angiotensin II → vasoconstriction + stimulates aldosterone
- Aldosterone (adrenal cortex) → ↑ Na+ and water reabsorption → ↑ blood volume → ↑ BP
5. Vasopressin (ADH):
- Released by posterior pituitary in response to ↑ osmolality or ↓ BP
- Vasoconstriction (V1 receptors) + water reabsorption (V2 receptors) → ↑ blood volume → ↑ BP
6. Capillary fluid shift:
- ↓ BP → capillary hydrostatic pressure falls → interstitial fluid absorbed into blood → expands plasma volume
C. Long-term Regulation:
7. Renal pressure-natriuresis (most important long-term):
- ↑ BP → ↑ GFR + ↓ tubular Na+ reabsorption → ↑ Na+ and water excretion → ↓ blood volume → ↓ BP
- Kidney sets the "long-term set point" for BP; chronic hypertension requires a shift in this curve
8. Aldosterone and ADH: Long-term control of blood volume
Hypertension
Definition: Persistently elevated BP ≥ 130/80 mmHg (AHA 2017) or ≥ 140/90 mmHg (JNC 7 / most guidelines)
Classification:
| Grade | SBP | DBP |
|---|---|---|
| Normal | < 120 | < 80 |
| Elevated | 120-129 | < 80 |
| Stage 1 (Grade 1) | 130-139 | 80-89 |
| Stage 2 (Grade 2) | ≥ 140 | ≥ 90 |
| Hypertensive crisis | > 180 | > 120 |
Types:
- Essential (Primary) hypertension (90-95%): No identifiable cause; multifactorial (genetics, salt intake, obesity, stress, sedentary lifestyle)
- Secondary hypertension (5-10%): Identifiable cause
- Renal: Chronic kidney disease, renal artery stenosis
- Endocrine: Hyperaldosteronism (Conn's), phaeochromocytoma, Cushing's, hyperthyroidism
- Drugs: OCPs, NSAIDs, steroids, sympathomimetics
Complications (End-organ damage - "CHADS"):
- Cardiac: LVH, angina, MI, heart failure
- Hypertensive encephalopathy, stroke, cerebral haemorrhage
- Aorta: Aortic dissection, aneurysm
- Dementia
- Stroke + renal damage (nephrosclerosis, proteinuria, CKD)
Treatment: Lifestyle (weight loss, salt restriction, exercise, reduce alcohol) + ACE inhibitors, ARBs, CCBs, thiazide diuretics, beta-blockers
Hypotension
Definition: SBP < 90 mmHg or > 40 mmHg fall from baseline
Types:
- Orthostatic (postural) hypotension: ≥ 20 mmHg fall in SBP on standing; causes: dehydration, autonomic neuropathy (diabetes, Parkinson's), antihypertensives, prolonged bed rest
- Neurally mediated (vasovagal) syncope: Paradoxical bradycardia + vasodilation; triggered by pain, emotion, prolonged standing
Q6. 🔵 LQ - Cardiac Output: Definition, Factors Regulating It, Methods to Measure
Definition
Cardiac Output (CO): Volume of blood pumped by one ventricle per minute.
CO = Stroke Volume (SV) × Heart Rate (HR)
Normal: SV ≈ 70 mL; HR ≈ 72 bpm → CO ≈ 5,000 mL/min (5 L/min)
Cardiac Index (CI) = CO / Body Surface Area = 2.5-4.0 L/min/m2
Stroke Volume (SV) = End-diastolic volume (EDV) - End-systolic volume (ESV) = 120 - 50 = 70 mL
Ejection Fraction (EF) = SV/EDV × 100% = ~58% (normal > 55%)
Factors Regulating Cardiac Output:
1. Heart Rate (Chronotropy)
- ↑ HR → ↑ CO (up to ~150-160 bpm; above this, diastolic filling time too short → SV falls)
- Increased by: Sympathetic (β1), adrenaline, fever, hypoxia, exercise, anxiety, hyperthyroidism
- Decreased by: Parasympathetic (M2, via vagus), β-blockers, complete heart block, hypothyroidism
2. Stroke Volume (determined by 3 factors):
a) Preload (Ventricular filling pressure / EDV):
- = Force stretching the ventricle before contraction = EDV
- ↑ Preload → ↑ fibre length → ↑ force of contraction → ↑ SV (Frank-Starling Law)
- Frank-Starling Law: "The energy of contraction is proportional to the initial length of the cardiac muscle fibre"
- Increased by: ↑ venous return, bradycardia (more filling time), recumbent position, fluid loading
- Decreased by: haemorrhage, dehydration, venodilators (nitrates), tachycardia
b) Afterload (Resistance against which ventricle ejects):
- = Aortic diastolic pressure / Total Peripheral Resistance (TPR) for LV
- ↑ Afterload → ↑ wall tension → ventricle works harder → ↑ O2 consumption; in healthy heart, slight ↑; in failing heart, ↑ afterload → ↓ SV
- Increased by: hypertension, aortic stenosis, vasoconstriction
- Decreased by: vasodilators, aortic regurgitation
c) Contractility (Inotropy) - intrinsic myocardial force at a given preload:
- Independent of preload and afterload; reflects myocardial Ca2+ availability
- Positive inotropes (↑ contractility): Sympathetic/catecholamines (β1 → ↑ cAMP → ↑ Ca2+), digoxin (inhibits Na+-K+ ATPase → ↑ intracellular Na+ → ↑ Ca2+ via NCX), exercise
- Negative inotropes (↓ contractility): β-blockers, CCBs (verapamil, diltiazem), acidosis, hypoxia, heart failure
Methods to Measure Cardiac Output:
| Method | Principle | Notes |
|---|---|---|
| Fick's Principle (gold standard) | CO = O2 consumption / (arterial O2 - venous O2 content) | Requires arterial + pulmonary artery sampling |
| Thermodilution | CO = Volume of cold saline × ΔT constant / area under temperature-time curve (Stewart-Hamilton) | Requires pulmonary artery catheter (Swan-Ganz); most common clinical method |
| Dye dilution | CO = Injected dye / area under concentration-time curve | Indocyanine green dye |
| Echocardiography (Doppler) | SV = cross-sectional area × velocity time integral; CO = SV × HR | Non-invasive; widely used |
| Impedance cardiography | Change in thoracic electrical impedance with pulsatile blood flow | Non-invasive; less accurate |
Q7. 🟡 SQ - Heart Sounds
| Sound | Cause | Timing | Best Heard | Notes |
|---|---|---|---|---|
| S1 ("lub") | Closure of mitral + tricuspid valves at start of ventricular systole | Beginning of systole | Apex (mitral area) | Loud in mitral stenosis; soft in MR, heart failure |
| S2 ("dub") | Closure of aortic + pulmonary valves at end of ventricular systole | End of systole | Left sternal edge (pulmonary) + right 2nd ICS (aortic) | Split on inspiration (A2 before P2); fixed split in ASD; paradoxical split in LBBB/AS |
| S3 (ventricular gallop) | Rapid early ventricular filling | Early diastole | Apex | Normal in children/young adults and pregnancy; pathological in adults → heart failure, dilated cardiomyopathy |
| S4 (atrial gallop) | Atrial contraction against stiff ventricle | Late diastole | Apex | Always pathological → LVH (hypertension, aortic stenosis), acute MI, hypertrophic cardiomyopathy |
Murmurs = turbulent blood flow; graded I-VI (Levine scale)
Q8. 🟡 SQ - Coronary Circulation
- Right coronary artery (RCA): Supplies SA node (60%), AV node (90%), right ventricle, inferior/posterior LV, posterior interventricular septum
- Left coronary artery (LCA):
- Left anterior descending (LAD): Anterior LV wall, anterior IV septum (bundle branches), apex - "artery of sudden death"
- Left circumflex (LCx): Lateral and posterior LV; SA node (40%)
- Dominance: RCA dominant in ~80% (supplies posterior descending artery); LCA dominant in ~10%; co-dominant 10%
Characteristics of coronary blood flow:
- Total flow: ~250 mL/min at rest (~5% of CO)
- Flow occurs mainly during diastole (LV compresses vessels during systole)
- Highest O2 extraction of any organ (~75%; can only ↑ flow, not extraction, during ↑ demand)
- Autoregulation: 60-140 mmHg perfusion pressure range; vasodilator reserve (adenosine, NO, prostacyclin)
- Angina = demand > supply; coronary steal (vasodilators divert blood)
Q9. 🟡 SQ - Cardiac Failure
Definition: Inability of the heart to pump sufficient blood to meet the metabolic demands of the body at normal filling pressures.
Types:
- Left heart failure: ↓ CO + pulmonary congestion → breathlessness, orthopnoea, PND, basal crepitations
- Right heart failure: Systemic venous congestion → peripheral oedema, raised JVP, hepatomegaly
- Congestive cardiac failure (CCF): Both sides involved
- Systolic failure: ↓ EF (< 40%); dilated, weak ventricle; HFrEF
- Diastolic failure: Normal EF but stiff ventricle (impaired filling); HFpEF; e.g., LVH, restrictive cardiomyopathy
Compensatory Mechanisms (initially helpful, later harmful):
- Frank-Starling mechanism: ↑ EDV → ↑ SV (limited; eventually ventricle dilates)
- Tachycardia: ↑ HR → maintains CO
- RAAS activation: ↑ Angiotensin II + Aldosterone → Na+ and water retention → ↑ blood volume → ↑ preload
- Sympathetic activation: ↑ HR + contractility + vasoconstriction
- Ventricular hypertrophy/remodelling: Initially maintains CO; eventually fibrosis + dysfunction
Clinical Features:
- Left failure: Dyspnoea on exertion → orthopnoea → PND → pulmonary oedema; S3 gallop, basal crepitations
- Right failure: Peripheral pitting oedema, ↑ JVP, hepatomegaly, ascites
- Both: Fatigue, reduced exercise tolerance, cool peripheries
Treatment:
- Diuretics (↓ preload/congestion), ACE inhibitors/ARBs (↓ afterload + RAAS), β-blockers (reduce remodelling), aldosterone antagonists (spironolactone), SGLT2 inhibitors, sacubitril-valsartan; CRT, ICD, transplant in severe cases
Q10. 🟡 SQ - Shock
Definition: A state of acute circulatory failure leading to inadequate tissue perfusion and cellular hypoxia, with the potential for multi-organ failure.
Classification:
| Type | Cause | CO | SVR | CVP | Example |
|---|---|---|---|---|---|
| Hypovolemic | ↓ blood/fluid volume | ↓ | ↑ | ↓ | Haemorrhage, burns, severe dehydration |
| Cardiogenic | Pump failure | ↓ | ↑ | ↑ | MI, severe arrhythmia, valve failure |
| Distributive | Maldistribution of blood flow | ↑/N | ↓ | ↓ | Septic shock, anaphylaxis, neurogenic |
| Obstructive | Obstruction to flow | ↓ | ↑ | ↑ | Cardiac tamponade, tension pneumothorax, massive PE |
Stages of Shock:
- Compensated (early): Compensatory mechanisms maintain BP; tachycardia, peripheral vasoconstriction, cool clammy skin
- Decompensated (progressive): Mechanisms fail; ↓ BP, confusion, oliguria
- Irreversible (terminal): Multi-organ failure; cell death irreversible despite treatment
Septic Shock:
- Endotoxins → systemic inflammatory response → vasodilation (↓ SVR) → maldistribution of flow → cellular hypoxia despite normal or high CO
- Features: ↑ CO, ↓ SVR, warm peripheries (early), fever/hypothermia, DIC
Treatment Principles:
- Restore tissue perfusion: IV fluids (hypovolemic), vasopressors (noradrenaline in septic/distributive), treat cause
- Monitor: MAP ≥ 65 mmHg, urine output ≥ 0.5 mL/kg/hr, serum lactate
Sources: Color Atlas of Human Anatomy Vol 2 (Thieme); Medical Physiology (Boron & Boulpaep); Costanzo Physiology 7th Ed; Katzung's Pharmacology 16th Ed; Robbins & Kumar Basic Pathology
Ready to continue with Chapter 6: Respiratory System whenever you say so!
Continue
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Chapter 6: Respiratory System
Legend: 🔵 LQ = Long Question (10-15 marks) | 🟡 SQ = Short Question (5 marks)
Q1. 🔵 LQ - Lung Volumes and Capacities
Lung volumes and capacities describe the amount of air in the lungs at different points of the respiratory cycle.
A. Lung Volumes (4 primary, non-overlapping):
| Volume | Definition | Normal Value |
|---|---|---|
| Tidal Volume (TV / VT) | Volume of air inspired or expired in one normal quiet breath | 500 mL |
| Inspiratory Reserve Volume (IRV) | Maximum additional volume that can be inspired above normal tidal inspiration | 3,000 mL |
| Expiratory Reserve Volume (ERV) | Maximum additional volume that can be expired beyond normal tidal expiration | 1,200 mL |
| Residual Volume (RV) | Volume remaining in lungs after maximal forced expiration; cannot be measured by spirometry | 1,200 mL |
B. Lung Capacities (combinations of volumes):
| Capacity | Formula | Normal Value | Clinical Significance |
|---|---|---|---|
| Inspiratory Capacity (IC) | TV + IRV | 3,500 mL | Max breath from resting expiratory level |
| Functional Residual Capacity (FRC) | ERV + RV | 2,400 mL | Volume at end of normal expiration; equilibrium lung volume; ↑ in emphysema, ↓ in fibrosis |
| Vital Capacity (VC) | IRV + TV + ERV | 4,700 mL | Max volume that can be expelled after maximal inspiration; decreases with lung disease, age |
| Total Lung Capacity (TLC) | VC + RV | 5,900 mL | Total volume in lungs at maximal inspiration; ↑ in emphysema, ↓ in restrictive disease |
Note: RV, FRC, and TLC cannot be measured by spirometry alone (need helium dilution or body plethysmograph)
C. Spirometric Measurements:
| Parameter | Definition | Normal | Significance |
|---|---|---|---|
| FVC | Forced Vital Capacity - total air exhaled with max forced effort | ~4.7 L | ↓ in both obstructive and restrictive |
| FEV1 | Volume expired in first second of forced expiration | ~3.5 L (75-80% of FVC) | ↓↓ in obstructive; mildly ↓ in restrictive |
| FEV1/FVC ratio | > 0.70 (70%) | < 70% = obstructive; normal or ↑ in restrictive | |
| PEFR | Peak Expiratory Flow Rate | ~600 L/min in adult males | Used in asthma monitoring |
| FEF 25-75% | Mid-expiratory flow rate | — | Sensitive for early small airway disease |
Pattern Recognition:
| Disease | FVC | FEV1 | FEV1/FVC | TLC | RV |
|---|---|---|---|---|---|
| Obstructive (asthma, COPD) | N or ↓ | ↓↓ | ↓ (< 70%) | ↑ | ↑ |
| Restrictive (fibrosis, obesity) | ↓ | ↓ | N or ↑ | ↓ | ↓ or N |
Q2. 🔵 LQ - Mechanics of Breathing, Surfactant, and Compliance
A. Mechanics of Breathing
Quiet Inspiration (active process):
- Diaphragm contracts (descends 1-10 cm) - primary muscle of inspiration (innervated by phrenic nerve C3,4,5)
- External intercostal muscles contract → ribs elevated + outward (bucket-handle movement)
- Thoracic volume increases → intrathoracic pressure falls below atmospheric → air flows IN
- Pleural pressure: -5 cmH2O at rest → -8 cmH2O during inspiration
Quiet Expiration (passive process):
- Diaphragm + intercostals relax
- Elastic recoil of lungs + chest wall drives air out
- No active muscle contraction needed
Forced Expiration (active):
- Internal intercostals contract
- Abdominal muscles contract (rectus abdominis, obliques) → increases intra-abdominal pressure → forces diaphragm upward
Accessory muscles of inspiration:
- Scalene muscles (raise first 2 ribs)
- Sternocleidomastoid (raises sternum)
- Used in severe dyspnoea / respiratory distress
Muscles of forced expiration:
- Internal intercostals
- Abdominal muscles (rectus abdominis, external/internal obliques, transversus)
B. Surfactant
Composition: Dipalmitoyl phosphatidylcholine (DPPC, lecithin) - 70%; other phospholipids + apoproteins (SP-A, SP-B, SP-C, SP-D)
Site of production: Type II pneumocytes (alveolar type II cells); secreted into alveolar surface
Function (LaPlace's Law: P = 2T/r):
- Surfactant reduces surface tension of alveolar fluid
- This is critical because small alveoli (small radius r) would otherwise have very high collapsing pressure
- Without surfactant: small alveoli collapse (atelectasis) + large alveoli overdistend
- Surfactant increases compliance, reduces work of breathing, and stabilises alveoli of different sizes by reducing surface tension more in smaller alveoli (where molecules are closer together)
Clinical significance:
- Neonatal Respiratory Distress Syndrome (NRDS / Hyaline Membrane Disease): Premature infants lack surfactant (adequate surfactant production requires 34-36 weeks gestation; induced by cortisol) → alveolar collapse at birth → severe respiratory distress
- Prevention: Antenatal corticosteroids to mother; postnatal surfactant replacement therapy
- Surfactant also has immune functions via SP-A and SP-D (opsonisation, innate immunity)
C. Compliance
Definition: The change in lung volume produced per unit change in pressure (distending pressure).
C = ΔV / ΔP (mL/cmH2O)
- Normal lung compliance: ~200 mL/cmH2O
Types:
- Static compliance: Measured when no airflow; reflects elastic properties alone
- Dynamic compliance: Measured during airflow; affected by airway resistance
Factors increasing compliance (easier to inflate):
- Emphysema (destruction of elastic tissue)
- Aging
- Surfactant
Factors decreasing compliance (stiffer, harder to inflate):
- Pulmonary fibrosis (increased collagen)
- NRDS (surfactant deficiency)
- Pulmonary oedema
- Atelectasis
Hysteresis: During inflation and deflation, different pressure-volume curves are traced. The area between them represents work done against surface tension and tissue viscosity.
Q3. 🟡 SQ - Dead Space and Alveolar Ventilation
Minute Ventilation (VE) = VT × RR = 500 mL × 12 = 6,000 mL/min
Dead Space:
- Anatomic dead space: Conducting airways (nose → bronchioles, no gas exchange) = 150 mL
- Physiologic dead space: Anatomic + functional (alveoli ventilated but not perfused; e.g., pulmonary embolism); in healthy lungs ≈ anatomic dead space
- Bohr equation for physiologic dead space: VD = VT × (PaCO2 - PECO2) / PaCO2
Alveolar Ventilation (VA) = (VT - VD) × RR = (500 - 150) × 12 = 4,200 mL/min
Only alveolar ventilation participates in gas exchange; dead space ventilation is wasted
Clinical significance: Increased dead space (pulmonary embolism, COPD, positive pressure ventilation) → CO2 retention unless RR or VT compensates
Q4. 🔵 LQ - Gas Exchange and Transport of O2 and CO2
A. Gas Exchange at Alveoli and Tissues
Dalton's Law: Total pressure = sum of partial pressures of each gas
Atmospheric pressure: 760 mmHg; inspired air composition:
- pO2 in atmosphere: 160 mmHg (21% of 760)
- pO2 in alveoli (PAO2): ~100 mmHg (diluted by CO2 + water vapour)
- pCO2 in alveoli (PACO2): ~40 mmHg
Alveolar Gas Equation:
PAO2 = PiO2 - (PaCO2 / RQ) = 150 - (40/0.8) = 100 mmHg
Fick's Law of Diffusion: Rate of diffusion ∝ (surface area × ΔP × solubility) / (thickness × MW)
- Large surface area of alveoli (~70 m2) + thin membrane (0.3-0.5 μm) → rapid diffusion
- CO2 diffuses ~20x faster than O2 (despite lower partial pressure gradient) due to higher solubility
Partial Pressures at Key Sites:
| Gas | Alveolar air | Arterial blood | Venous blood | Tissues |
|---|---|---|---|---|
| O2 (pO2) | 100 mmHg | 95-100 mmHg | 40 mmHg | 20-40 mmHg |
| CO2 (pCO2) | 40 mmHg | 40 mmHg | 46 mmHg | 45-50 mmHg |
B. Oxygen Transport
1. Dissolved O2: Only 1.5% of total O2 (0.003 mL/100 mL blood per mmHg pO2)
2. Bound to Haemoglobin (HbO2): 98.5% of total O2
- Each gram of Hb carries 1.34 mL O2 when fully saturated
- At Hb 15 g/dL: O2 carrying capacity = 15 × 1.34 = 20.1 mL/100 mL blood
- O2 Content (CaO2) = (Hb × 1.34 × SaO2) + (0.003 × PaO2)
O2-Haemoglobin Dissociation Curve (sigmoid shape):
- Sigmoid due to cooperative binding (allosteric mechanism)
- P50 = partial pressure at which Hb is 50% saturated = 26-27 mmHg
Right shift (↓ O2 affinity = ↑ O2 unloading to tissues) = Bohr Effect:
- ↑ CO2 (↑ H+, acidosis), ↑ temperature, ↑ 2,3-DPG
- Beneficial in exercising tissues (unloads more O2)
Left shift (↑ O2 affinity = ↓ O2 unloading) = Haldane Effect:
- ↓ CO2, alkalosis, ↓ temperature, ↓ 2,3-DPG, HbF (foetal Hb - facilitates O2 transfer from mother to foetus), CO poisoning
C. Carbon Dioxide Transport
CO2 is transported in three forms:
| Form | % of total |
|---|---|
| Dissolved in plasma | 5-10% |
| Carbaminohaemoglobin (CO2 bound to Hb and other proteins) | 20-25% |
| Bicarbonate (HCO3-) - most important form | 60-70% |
Bicarbonate formation (in RBCs):
CO2 + H2O → H2CO3 → (carbonic anhydrase) → H+ + HCO3-
- H+ buffered by deoxyhaemoglobin (Haldane effect)
- HCO3- exits RBC in exchange for Cl- (chloride shift / Hamburger phenomenon)
At the lungs: All reactions reverse; CO2 expelled
Q5. 🟡 SQ - Ventilation/Perfusion (V/Q) Ratio
Normal V/Q ratio: ~0.8 (VA = 4.2 L/min; Q = 5 L/min)
Regional differences in normal upright lung:
- Apex: V/Q > 0.8 (high) - both ventilation and perfusion are lower but perfusion reduced more; apex relatively over-ventilated
- Base: V/Q < 0.8 (low) - both higher but perfusion increases more than ventilation; base relatively over-perfused
V/Q Mismatch (Causes of Hypoxaemia):
| V/Q State | Description | V/Q ratio | Cause | pO2 | pCO2 |
|---|---|---|---|---|---|
| Ideal | Normal match | ~0.8 | — | 100 | 40 |
| Dead space | Ventilated, not perfused | → ∞ | Pulmonary embolism | ~150 (alveolar air) | ~0 |
| High V/Q | Over-ventilated relative to perfusion | > 0.8 | Reduced blood flow | ↑ | ↓ |
| Low V/Q | Under-ventilated relative to perfusion | < 0.8 | Mucus plugging, bronchospasm | ↓ | ↑ |
| Shunt | Perfused, not ventilated | → 0 | Atelectasis, consolidation, AV fistula | Very low | ↑ |
Key difference - V/Q mismatch vs shunt:
- V/Q mismatch: Correctable by giving supplemental O2 (↑ PAO2 corrects hypoxaemia)
- True shunt: NOT correctable by supplemental O2 alone (deoxygenated blood bypasses ventilated alveoli)
Hypoxic vasoconstriction: When PAO2 falls locally → arteriolar vasoconstriction → blood diverted to better-ventilated regions → optimises V/Q matching (opposite of systemic circulation)
Q6. 🔵 LQ - Control of Respiration
Breathing is regulated by respiratory centres in the brainstem that integrate sensory inputs and generate rhythmic motor output.
A. Respiratory Centres (in brainstem):
1. Medullary Respiratory Centres (primary):
- Dorsal Respiratory Group (DRG) - nucleus tractus solitarius: primarily inspiratory neurons; sets basic rhythm; receives afferents from peripheral chemoreceptors + vagus
- Ventral Respiratory Group (VRG) - contains pre-Bötzinger complex (rhythm generator) + Bötzinger complex (expiratory); mainly expiratory but recruits during forced breathing
2. Pontine Centres (modulate medullary rhythm):
- Pontine Respiratory Group (PRG) / Pneumotaxic centre - upper pons: controls rate and depth; inhibits inspiration → smooth cycling; lesion = apneusis (prolonged inspiration)
- Apneustic centre - lower pons: stimulates and prolongs inspiration; normally inhibited by pneumotaxic centre
B. Chemical Control (most important):
1. Central Chemoreceptors (dominant in normal breathing):
- Location: Ventral surface of medulla (separate from respiratory centres)
- Stimulus: ↑ H+ (↓ pH) in CSF - indirectly from ↑ PaCO2 (CO2 crosses BBB, forms H+ in CSF via carbonic anhydrase)
- Response: CO2 ↑ by 1 mmHg → VE increases by ~2 L/min
- NOT directly sensitive to PaO2
2. Peripheral Chemoreceptors:
- Location: Carotid bodies (main; CN IX) + Aortic bodies (CN X)
- Stimulus: ↓ PaO2 (below 60 mmHg - dominant stimulus), ↑ PaCO2, ↓ pH
- Respond rapidly (within seconds) to hypoxaemia
- In chronic hypercapnia (COPD), central receptors desensitise → patient depends on hypoxic drive via peripheral chemoreceptors (danger of giving high-flow O2)
3. Response Summary:
| Stimulus | Receptor | Response |
|---|---|---|
| ↑ PaCO2 (↑ H+ in CSF) | Central | ↑ VE (most powerful normal driver) |
| ↓ PaO2 < 60 mmHg | Peripheral | ↑ VE |
| ↓ pH (metabolic acidosis) | Peripheral | ↑ VE (compensatory hyperventilation) |
C. Other Afferent Inputs:
Hering-Breuer Reflex:
- Lung stretch receptors (slowly adapting) in airways → via vagus to DRG → inhibit inspiration when lungs fully inflated
- Prevents over-inflation; important in neonates; minor role in adults at tidal volumes
Juxtapulmonary (J) receptors (C-fibres):
- Located near pulmonary capillaries; stimulated by pulmonary oedema, emboli, chemicals
- Cause rapid shallow breathing, cough, bronchoconstriction
Irritant (rapidly adapting) receptors:
- In airway epithelium; stimulated by dust, smoke, noxious gases → cough, bronchoconstriction
Proprioceptors in muscles and joints:
- Stimulate ventilation during exercise (fast response before blood gas changes occur)
Q7. 🟡 SQ - Hypoxia: Types and Classification
Definition: Hypoxia is inadequate O2 delivery to or utilisation by the tissues.
Classification:
| Type | Mechanism | pO2 (arterial) | O2 Content | O2 Saturation | Examples |
|---|---|---|---|---|---|
| Hypoxic (Hypoxaemic) hypoxia | ↓ PaO2 - inadequate O2 loading in lungs | ↓ | ↓ | ↓ | High altitude, V/Q mismatch, hypoventilation, shunt, diffusion impairment |
| Anaemic hypoxia | Normal PaO2 but reduced O2-carrying capacity (↓ Hb or dysfunctional Hb) | Normal | ↓ | Normal | Anaemia, CO poisoning (COHb), methaemoglobinaemia |
| Stagnant (Ischaemic) hypoxia | Normal O2 content but inadequate blood flow to tissues | Normal | Normal | Normal | Heart failure, shock, peripheral arterial disease, local ischaemia |
| Histotoxic hypoxia | Cells cannot utilise O2 despite adequate delivery (mitochondrial blockade) | Normal | Normal | Normal | Cyanide poisoning (blocks cytochrome oxidase), carbon monoxide (high dose) |
Additional types:
- Demand hypoxia: Excessive tissue demand exceeds delivery (e.g., sepsis, hyperthyroidism)
- Affinity hypoxia: Hb has such high O2 affinity it won't release O2 to tissues (carbon monoxide - left shift)
Cyanosis
Definition: Bluish discolouration of skin and mucous membranes due to ≥ 5 g/dL of deoxygenated (reduced) Hb in capillary blood (not a % - absolute amount matters).
Types:
- Central cyanosis: Affects tongue + mucous membranes + periphery; due to arterial hypoxaemia (V/Q mismatch, hypoventilation, shunt, lung disease, high altitude)
- Peripheral cyanosis: Affects extremities only; tongue normal; due to ↑ O2 extraction in cold/slow-moving blood (cold exposure, heart failure, Raynaud's)
Note: Anaemic patients cannot become cyanotic easily (not enough Hb to accumulate 5 g/dL deoxyHb); polycythaemic patients may appear cyanotic at relatively mild hypoxaemia.
Q8. 🔵 LQ - Pulmonary Function Tests and Respiratory Diseases
A. Pulmonary Function Tests (PFTs)
Spirometry:
- FVC, FEV1, FEV1/FVC, PEFR, FEF 25-75% (see Q1 for values)
- Obstructive pattern (FEV1/FVC < 70%): COPD, asthma, bronchiectasis
- Restrictive pattern (FVC ↓, FEV1/FVC normal/↑): pulmonary fibrosis, pleural effusion, chest wall deformity
Flow-volume loop:
- Obstructive: Scooped-out (concave) expiratory limb
- Restrictive: Small loop (reduced volumes), normal shape
Diffusing Capacity for CO (DLCO / TLCO):
- Measures gas transfer across alveolar-capillary membrane
- ↓ DLCO: Emphysema (↓ surface area), pulmonary fibrosis (thickened membrane), pulmonary oedema
- ↑ DLCO: Pulmonary haemorrhage (extra Hb available), polycythaemia, post-exercise
Peak Expiratory Flow Rate (PEFR):
- Cheap, portable monitoring of obstructive disease
- Used for asthma monitoring and severity classification
B. Asthma
Definition: Chronic inflammatory airway disease characterised by reversible airflow obstruction, bronchial hyperresponsiveness, and airway inflammation.
Pathophysiology:
- Trigger (allergen, exercise, cold air, aspirin) → mast cell degranulation → histamine, leukotrienes, prostaglandins
- Bronchospasm: Smooth muscle contraction → airway narrowing
- Mucus hypersecretion → plugging
- Inflammation + oedema → airway wall thickening
- Chronic changes: Airway remodelling (smooth muscle hypertrophy, goblet cell hyperplasia, fibrosis)
Features: Wheeze, breathlessness, chest tightness, cough (especially nocturnal/early morning); diurnal variation
PFTs: Obstructive pattern; reversible with bronchodilator (FEV1 ↑ >12% + >200 mL)
Treatment: Stepwise - SABA (salbutamol) → ICS (budesonide) → LABA + ICS → add-ons; biologics (omalizumab for severe allergic asthma)
C. COPD (Chronic Obstructive Pulmonary Disease)
Definition: Preventable and treatable disease characterised by persistent airflow limitation that is not fully reversible, associated with abnormal inflammatory response to noxious particles/gases.
Two main types:
- Chronic Bronchitis: "Blue bloater" - productive cough >3 months/year for >2 consecutive years; ↑ mucus glands (Reid index > 0.5), mucus hypersecretion; hypoxaemia + hypercapnia; cyanosis + oedema
- Emphysema: "Pink puffer" - permanent destructive enlargement of air spaces distal to terminal bronchioles; ↓ elastic recoil; barrel chest; hyperinflation; pursed-lip breathing; mainly hypoxic but retain CO2 less
Risk factors: Cigarette smoking (#1), air pollution, occupational dust, α1-antitrypsin deficiency (emphysema), recurrent infections
Pathophysiology of Emphysema: Smoking → neutrophils/macrophages → elastase (protease) release → destroys alveolar walls (elastin/collagen) → air trapping + ↓ elastic recoil + ↓ alveolar surface → PFT: ↑ TLC, ↑ RV, ↓ FEV1, ↓ DLCO
Treatment: Smoking cessation (#1), SABA/LAMA bronchodilators, ICS in frequent exacerbations, pulmonary rehabilitation, LTOT (long-term O2 therapy if PaO2 < 55 mmHg), surgery (bullectomy, lung volume reduction)
D. Respiratory Failure
Type 1 (Hypoxaemic): PaO2 < 60 mmHg with normal or ↓ PaCO2
- Mechanism: V/Q mismatch, shunt, diffusion impairment
- Causes: Pneumonia, pulmonary oedema, ARDS, PE, asthma attack
- Treatment: Supplemental O2 (responds well)
Type 2 (Hypercapnic / Ventilatory): PaO2 < 60 mmHg AND PaCO2 > 45 mmHg
- Mechanism: Alveolar hypoventilation (pump failure)
- Causes: COPD exacerbation, respiratory muscle weakness (MG, GBS), CNS depression (opioids), chest wall deformity
- Treatment: Treat cause; NIV (BiPAP); controlled O2 (avoid hypercapnia); intubation if severe
Q9. 🟡 SQ - Oxygen Dissociation Curve (Summary)
The O2-Haemoglobin Dissociation Curve is a sigmoid (S-shaped) curve plotting %Hb saturation against PO2.
Key points on the curve:
- At PaO2 = 100 mmHg (arterial blood): SaO2 = 98% (plateau region - loading in lungs)
- At PO2 = 40 mmHg (mixed venous): SaO2 = 75% (steep region - unloading in tissues)
- At P50 = 26-27 mmHg: SaO2 = 50%
Physiological significance of sigmoid shape:
- Flat upper portion: Loading of O2 in lungs is maintained even if PaO2 drops to ~60 mmHg (SaO2 still 90%) - provides safety margin at altitude/lung disease
- Steep lower portion: Small drop in tissue PO2 → large O2 unloading → tissues can extract more O2 during exercise
Factors causing Right Shift (↓ affinity - more O2 released):
- ↑ CO2, ↑ H+ (↓ pH) = Bohr effect
- ↑ Temperature
- ↑ 2,3-DPG (produced by RBCs in chronic hypoxia, anaemia, high altitude)
Factors causing Left Shift (↑ affinity - less O2 released):
- ↓ CO2, ↓ H+ (↑ pH)
- ↓ Temperature
- ↓ 2,3-DPG
- Foetal Hb (HbF) - binds 2,3-DPG less; allows placental O2 transfer
- Carboxyhaemoglobin (COHb) - CO binds Hb 250x more avidly than O2; also causes left shift; cherry-red colour; treated with 100% O2
Sources: Costanzo Physiology 7th Edition; Murray & Nadel's Textbook of Respiratory Medicine; Tintinalli's Emergency Medicine; Harrison's Principles of Internal Medicine 22nd Edition
Ready to continue with Chapter 7: Renal System whenever you say so!
Continue
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Chapter 7: Renal System
Legend: 🔵 LQ = Long Question (10-15 marks) | 🟡 SQ = Short Question (5 marks)
Q1. 🟡 SQ - Functions of the Kidney
The kidneys are paired retroperitoneal organs (each ~150 g) performing multiple homeostatic functions:
Excretory Functions:
- Excretion of metabolic waste products: Urea (protein catabolism), creatinine (muscle metabolism), uric acid (purine catabolism), bilirubin metabolites
- Excretion of foreign chemicals: Drugs, toxins, food additives, pesticides
Regulatory Functions:
- Water and osmolality regulation: Adjusts urine osmolality between 50-1200 mOsm/kg to maintain plasma osmolality ~290 mOsm/kg
- Electrolyte balance: Regulates Na+, K+, Cl-, HCO3-, Ca2+, Mg2+, PO4-
- Acid-base balance: Excretes H+ and regenerates HCO3-; maintains arterial pH 7.35-7.45
- Blood pressure regulation: Via sodium balance, volume status, and RAAS (renin-angiotensin-aldosterone system)
Endocrine Functions:
- Erythropoietin (EPO): Secreted by interstitial cells of cortex in response to hypoxia → stimulates RBC production in bone marrow
- Renin: Secreted by juxtaglomerular cells of afferent arteriole → activates RAAS → angiotensin II → vasoconstriction + aldosterone release
- 1,25-Dihydroxycholecalciferol (Calcitriol / Active Vitamin D): Kidney converts 25-OH-D3 → 1,25-(OH)2-D3 via 1α-hydroxylase → promotes intestinal Ca2+ absorption
- Prostaglandins: Vasodilatory PGE2 and PGI2 locally regulate glomerular blood flow
Gluconeogenesis:
- Kidneys contribute ~20% of total gluconeogenesis (especially during prolonged fasting)
Q2. 🔵 LQ - Glomerular Filtration and GFR
A. The Nephron (Functional Unit)
Each kidney contains ~1 million nephrons. A nephron consists of:
- Renal corpuscle = glomerulus + Bowman's capsule
- Proximal convoluted tubule (PCT)
- Loop of Henle (descending thin limb, ascending thin limb, thick ascending limb)
- Distal convoluted tubule (DCT)
- Collecting duct (CD) - connects to renal pelvis
B. Glomerular Filtration
Definition: The process by which plasma is filtered across the glomerular capillary membrane into Bowman's capsule to form the ultrafiltrate.
GFR (Glomerular Filtration Rate):
- Normal: 125 mL/min (~180 L/day); only ~1.5 L excreted as urine
- Filtration fraction = GFR / Renal plasma flow = 125/625 = ~20%
Starling forces governing filtration:
The Net Filtration Pressure (NFP) = (PGC + πBS) - (PBS + πGC)
| Force | Value | Effect |
|---|---|---|
| Glomerular hydrostatic pressure (PGC) | 60 mmHg | Favours filtration |
| Colloid osmotic pressure of plasma proteins (πGC) | 32 mmHg | Opposes filtration |
| Bowman's space hydrostatic pressure (PBS) | 18 mmHg | Opposes filtration |
| Bowman's space oncotic pressure (πBS) | ~0 | Negligible |
| NFP | +10 mmHg | → Filtration |
Filtration membrane (3 layers):
- Glomerular capillary endothelium (fenestrated, pores 60-100 nm) - charge + size barrier
- Glomerular basement membrane (GBM) - negative charge barrier (type IV collagen, laminin, heparan sulphate)
- Podocyte foot processes with slit diaphragms (nephrin, podocin) - final size barrier
Permselectivity:
- Freely filtered: Water, glucose, amino acids, urea, creatinine, uric acid, electrolytes (MW < 7,000)
- Partially restricted: Albumin (MW 69,000; negative charge repelled by GBM)
- Not filtered: RBCs, WBCs, platelets, large plasma proteins
C. Measurement of GFR
Renal Clearance (C):
C = (U × V) / P (mL/min)
- U = urine concentration of substance (mg/mL)
- V = urine flow rate (mL/min)
- P = plasma concentration (mg/mL)
Ideal GFR marker requirements: Freely filtered, not reabsorbed, not secreted, not metabolised by kidney, non-toxic
Inulin clearance (Gold standard): Meets all criteria exactly; exogenous polysaccharide
- GFR = Uinulin × V / Pinulin = 125 mL/min
Creatinine clearance (Clinical standard): Endogenous, freely filtered; slightly secreted by proximal tubule → overestimates GFR by ~10-15%; still widely used
- Normal: 90-130 mL/min/1.73 m2
Para-aminohippuric acid (PAH) clearance: Used to measure Effective Renal Plasma Flow (ERPF) - freely filtered + completely secreted by proximal tubule on first pass
- ERPF = CPAH = UPAH × V / PPAH = 625 mL/min
eGFR (Estimated GFR): Calculated from serum creatinine + age + sex + race using CKD-EPI or MDRD equation; used clinically for CKD staging
D. Regulation of GFR
1. Autoregulation (intrinsic - operates over MAP 80-180 mmHg):
- Myogenic mechanism: ↑ BP → stretch of afferent arteriole wall → vasoconstriction → maintained GFR
- Tubuloglomerular feedback (TGF): ↑ NaCl delivery to macula densa cells of juxtaglomerular apparatus → release of adenosine (and TXA2) → constrict afferent arteriole → ↓ GFR (negative feedback)
2. Hormonal/Neural Regulation:
| Factor | Effect on GFR | Mechanism |
|---|---|---|
| Angiotensin II | ↓ GFR (net) | Constricts efferent > afferent; ↓ Kf |
| ANP (Atrial Natriuretic Peptide) | ↑ GFR | Dilates afferent, constricts efferent; ↑ Kf |
| Sympathetic nerves (high level) | ↓ GFR | Constrict afferent arteriole |
| Prostaglandins (PGE2, PGI2) | Maintain GFR | Dilate afferent arteriole (important in low-flow states) |
| ADH (AVP) | Minor ↑ GFR | ↑ Kf |
| Dopamine (low dose) | ↑ GFR | Renal vasodilation |
Q3. 🔵 LQ - Tubular Reabsorption and Secretion
A. Overview
Of the 180 L filtered daily, ~178.5 L is reabsorbed and only ~1.5 L excreted.
- PCT reabsorbs ~65-67% of filtered Na+, water, glucose, amino acids, HCO3-
- Loop of Henle: ~25% Na+ reabsorption
- DCT and CD: Fine-tuning of Na+, K+, water, acid-base balance
B. Proximal Convoluted Tubule (PCT)
Reabsorbs 65% of filtered Na+, water, glucose, amino acids, HCO3-, urea, Cl-
Mechanisms:
- Na+ enters cell via Na+-glucose cotransporter (SGLT2), Na+-amino acid cotransporter, Na+/H+ exchanger (NHE3) on apical membrane
- Na+ exits basolaterally via Na+/K+-ATPase (primary active transport)
- Water follows osmotically through aquaporin 1 (AQP1) channels (iso-osmotic reabsorption)
- Glucose: reabsorbed by SGLT2 (PCT) and SGLT1 (late PCT); transport maximum (Tm) = 375 mg/min; threshold ~200 mg/dL; glucosuria above this
- HCO3-: reabsorbed as CO2 (not directly); Na+/H+ exchanger secretes H+ → H+ + HCO3- → H2CO3 → CO2 + H2O (carbonic anhydrase) → CO2 diffuses in → reformed to HCO3- intracellularly
Secretion by PCT:
- Organic acids: uric acid, bile salts, prostaglandins, creatinine (small amount)
- Organic bases: choline, histamine
- Drugs: penicillin, salicylates, PAH, thiazides, furosemide, probenecid (secreted via OAT transporters)
C. Loop of Henle
Thin descending limb: Water permeable, NOT solute permeable → water moves OUT (into hypertonic medulla) → tubular fluid becomes concentrated (up to 1200 mOsm)
Thin ascending limb: Impermeable to water; some passive NaCl efflux
Thick ascending limb (TAL - "diluting segment"):
- Impermeable to water
- Active NaCl reabsorption via Na+-K+-2Cl- (NKCC2) cotransporter on apical membrane - site of action of loop diuretics
- K+ recycled back into lumen (generating lumen-positive potential driving paracellular Ca2+, Mg2+ reabsorption)
- Dilutes tubular fluid → generates hypotonic fluid entering DCT (~100 mOsm)
D. Distal Convoluted Tubule (DCT)
- Reabsorbs Na+ via NCC (Na+-Cl- cotransporter) - site of action of thiazide diuretics
- Reabsorbs Ca2+ (regulated by PTH and calcitriol) via TRPV5 channel
- Reabsorbs Mg2+
- Aldosterone stimulates Na+ reabsorption here and in cortical collecting duct
E. Collecting Duct (CD)
Principal cells:
- Na+ reabsorption via ENaC (epithelial Na+ channel) - regulated by aldosterone (increases ENaC expression + Na+/K+-ATPase activity)
- K+ secretion into lumen (via ROMK channel) - explains aldosterone → hypokalaemia
- Water reabsorption via AQP2 - regulated by ADH/AVP
Intercalated cells:
- Type A (α): Secrete H+ (H+-ATPase) + reabsorb HCO3-; active in acidosis
- Type B (β): Secrete HCO3-, reabsorb H+; active in alkalosis
Q4. 🔵 LQ - Concentration and Dilution of Urine (Countercurrent Mechanism)
A. Overview
Kidneys can produce urine ranging from 50 to 1200 mOsm/kg, depending on the body's hydration status. This is achieved by the countercurrent system.
B. Countercurrent Multiplier (Loop of Henle)
Purpose: Creates a hyperosmotic medullary interstitium (gradient from ~300 mOsm at cortex to ~1200 mOsm at papilla).
Mechanism (step-by-step):
- Thick ascending limb (TAL) actively pumps NaCl into medullary interstitium (via NKCC2) BUT is impermeable to water → solute accumulates in interstitium
- This creates a hyperosmotic interstitium → draws water OUT of the thin descending limb (which is water-permeable, solute-impermeable) → descending tubular fluid becomes concentrated
- Concentrated fluid turns the hairpin bend and enters the ascending limb, which pumps more NaCl out
- Each cycle multiplies the osmotic gradient → tip of loop reaches ~1200 mOsm
- Urea recycling: In the presence of ADH, inner medullary collecting duct (IMCD) is permeable to urea → urea moves out into medulla → urea enters thin descending limb of loop → recycled → contributes ~400 mOsm to papillary tip gradient
C. Countercurrent Exchanger (Vasa Recta)
- Vasa recta = hairpin-shaped capillaries that parallel loop of Henle
- Blood entering descending vasa recta gains solute (NaCl, urea) as it descends into hypertonic medulla; loses water
- Blood leaving ascending vasa recta loses solute, gains water back
- Net effect: Solutes remain trapped in medulla; medullary interstitium osmolarity maintained
- Without vasa recta countercurrent exchange, the gradient would be washed out by blood flow
D. Role of ADH (Antidiuretic Hormone / Arginine Vasopressin - AVP)
Source: Synthesised in paraventricular (PVN) and supraoptic nuclei (SON) of hypothalamus; stored and released from posterior pituitary
Stimulus for release:
- ↑ plasma osmolality (>280 mOsm) detected by osmoreceptors in hypothalamus
- ↓ blood volume/pressure detected by baroreceptors (carotid sinus, aortic arch, atria)
- Nausea, pain, stress, nicotine → ↑ ADH
- Alcohol, ANP → suppress ADH
Mechanism of action:
- ADH binds V2 receptors on basolateral membrane of collecting duct principal cells
- → Gs protein → ↑ cAMP → PKA activation → phosphorylation → insertion of AQP2 water channels into apical membrane
- → Water reabsorption from collecting duct lumen into hypertonic medullary interstitium → concentrated urine
Summary:
| ADH Status | Urine Osmolality | Urine Volume | Condition |
|---|---|---|---|
| High ADH | Up to 1200 mOsm | ~500 mL/day | Dehydration, haemorrhage |
| Low ADH | ~50-100 mOsm | Up to 20 L/day | Diabetes Insipidus |
Diabetes Insipidus:
- Central DI: ↓ ADH production (head injury, tumour, surgery) → dilute polyuria; treated with desmopressin (DDAVP)
- Nephrogenic DI: Kidney unresponsive to ADH (V2 receptor or AQP2 mutation, hypercalcaemia, lithium toxicity) → treated with thiazides + low-salt diet
Q5. 🔵 LQ - Renal Regulation of Acid-Base Balance
A. Normal Blood Gas Values:
- Arterial pH: 7.35-7.45
- PaCO2: 35-45 mmHg
- HCO3-: 22-26 mEq/L
- Henderson-Hasselbalch equation: pH = 6.1 + log ([HCO3-] / 0.03 × PaCO2)
B. Renal Mechanisms for H+ Excretion:
1. HCO3- Reabsorption (PCT - 80-90% of filtered load):
- H+ secreted by NHE3 → combines with filtered HCO3- → H2CO3 → CO2 + H2O (carbonic anhydrase IV on brush border) → CO2 diffuses into PCT cells → carbonic anhydrase II converts back to H+ + HCO3- → H+ recycled, HCO3- exits into blood via NBC (Na+/HCO3- cotransporter)
- This process "reabsorbs" HCO3- (doesn't actually secrete net H+)
2. Titratable Acid Excretion (distal nephron):
- H+ pumped into tubular lumen by H+-ATPase (type A intercalated cells) combines with HPO4²- (dibasic phosphate, pKa 6.8) → H2PO4- (monobasic phosphate) excreted
- Phosphate acts as a "buffer" for H+ → each H2PO4- excreted represents one new HCO3- generated
3. Ammonium (NH4+) Excretion (most important in chronic acidosis):
- Glutamine enters PCT → glutaminase → NH4+ + HCO3- regenerated
- NH4+ secreted into tubular lumen (substitutes for K+ on NKCC2 in TAL, reabsorbed then secreted again)
- In acidosis, NH3 diffusion trapping: NH3 diffuses into collecting duct lumen → H+ + NH3 → NH4+ trapped (lipid-insoluble) → excreted
- Each NH4+ excreted = one new HCO3- entering blood
- NH4+ excretion increases 10-fold in chronic acidosis (major compensation)
C. Acid-Base Disorders:
| Disorder | Primary Change | Compensation | Examples |
|---|---|---|---|
| Respiratory Acidosis | ↑ PaCO2 | Renal: ↑ HCO3- reabsorption + NH4+ excretion (days) | COPD, hypoventilation, opioids |
| Respiratory Alkalosis | ↓ PaCO2 | Renal: ↓ HCO3- reabsorption (days) | Hyperventilation, anxiety, altitude |
| Metabolic Acidosis | ↓ HCO3- | Respiratory: hyperventilation (↓ PaCO2) - minutes; Kussmaul breathing | DKA, diarrhoea, lactic acidosis, renal failure |
| Metabolic Alkalosis | ↑ HCO3- | Respiratory: hypoventilation (↑ PaCO2) - minutes | Vomiting (HCl loss), excessive diuretics, Conn's syndrome |
Anion Gap = Na+ - (Cl- + HCO3-) = 8-12 mEq/L
- High anion gap metabolic acidosis (MUDPILES): Methanol, Uraemia, DKA, Paraldehyde, Isoniazid, Lactic acidosis, Ethylene glycol, Salicylates
- Normal anion gap (hyperchloraemic) acidosis: Diarrhoea, renal tubular acidosis, IV saline
Q6. 🟡 SQ - Micturition Reflex
Micturition = the act of voluntary urination; a spinal reflex under voluntary (cortical) control.
Anatomy:
- Detrusor muscle: Smooth muscle of bladder wall (parasympathetic, S2-S4 → contract = voiding)
- Internal urethral sphincter: Smooth muscle; sympathetic (L1-L2) keeps closed during storage
- External urethral sphincter: Skeletal muscle; voluntary (pudendal nerve, S2-S4 → contracts = continence)
Storage Phase:
- Sympathetic (L1-L2): Relaxes detrusor (β3-AR), contracts internal sphincter (α-AR) → urine stored
- External sphincter voluntarily contracted
- First urge to void: ~150 mL; fullness sensation: 400-500 mL
- Cortical/supraspinal centres continuously inhibit the voiding reflex
Voiding Phase:
- Voluntary decision → cortex releases inhibition → pontine micturition centre (PMC) activated
- PMC inhibits external sphincter (Onuf's nucleus) → external sphincter relaxes
- PMC activates sacral parasympathetic (S2-S4) → pelvic nerve → acetylcholine on M3 receptors → detrusor contracts
- Internal sphincter relaxes passively (coordinated with detrusor)
- Urine enters posterior urethra → stretch receptors → positive feedback → sustained voiding
Neurological lesions:
| Lesion | Effect |
|---|---|
| Spinal cord transection above S2 | Initial: spinal shock + urinary retention; Later: spastic (automatic) bladder - uninhibited reflex voiding |
| Sacral cord/peripheral nerve damage | Flaccid bladder (atonic); retention + overflow incontinence |
| Cortical lesion (frontal lobe) | Uninhibited detrusor contractions - urge incontinence |
Q7. 🔵 LQ - Renal Failure and Diuretics
A. Acute Kidney Injury (AKI)
Definition: Abrupt decline in GFR over hours-days; rise in serum creatinine ≥ 0.3 mg/dL in 48h or ≥ 1.5x baseline in 7 days; or urine output < 0.5 mL/kg/hr for 6h.
Classification:
| Type | Pre-renal | Intrinsic (Renal) | Post-renal |
|---|---|---|---|
| Mechanism | ↓ Renal perfusion (kidney structurally intact) | Kidney parenchyma damaged | Urinary tract obstruction |
| Causes | Dehydration, haemorrhage, heart failure, sepsis, NSAIDs | ATN (ischaemia/nephrotoxins), glomerulonephritis, AIN, vasculitis | BPH, renal stones, stricture, tumour |
| Urine osmolality | > 500 mOsm (kidney tries to conserve) | ~300 mOsm (isosthenuria) | Variable |
| Urine Na+ | < 20 mEq/L (avidly reabsorbed) | > 40 mEq/L (can't reabsorb) | Variable |
| FENa | < 1% | > 2% | Variable |
| Urine | Concentrated, no casts | Granular "muddy brown" casts (ATN), RBC casts (GN) | May have crystals |
| Treatment | IV fluids, treat cause | Identify + stop nephrotoxin; supportive | Relieve obstruction (catheter, stenting) |
ATN (Acute Tubular Necrosis) - Most common intrinsic AKI:
- Phases: Initiation → Oliguric (↓ urine < 400 mL/day; ↑ K+, ↑ urea, ↑ creatinine) → Polyuric (tubules recover, urine ↑ but can't concentrate) → Recovery
- Mechanism: Ischaemia or nephrotoxins (contrast, aminoglycosides, cisplatin) → tubular cell necrosis → cast formation → tubular obstruction + backleak
B. Chronic Kidney Disease (CKD)
Definition: Abnormalities of kidney structure or function present for > 3 months (GFR < 60 mL/min and/or markers of kidney damage).
GFR-based staging:
| Stage | eGFR (mL/min/1.73 m²) | Description |
|---|---|---|
| G1 | ≥ 90 | Normal or high GFR + kidney damage marker |
| G2 | 60-89 | Mildly decreased |
| G3a/3b | 30-59 | Moderately decreased |
| G4 | 15-29 | Severely decreased |
| G5 | < 15 | Kidney failure (dialysis/transplant) |
Consequences of CKD (due to ↓ nephron mass):
- ↑ urea, creatinine → uraemia (encephalopathy, pericarditis, platelet dysfunction)
- ↓ EPO → normocytic anaemia
- ↓ 1α-hydroxylase → ↓ calcitriol → ↓ Ca2+ absorption → hypocalcaemia → ↑ PTH → renal osteodystrophy
- ↑ K+ → hyperkalaemia (cardiac arrhythmias)
- ↓ H+ excretion → metabolic acidosis
- Na+/water retention → hypertension + oedema
- ↑ phosphate → hyperphosphataemia → ectopic calcification
C. Diuretics
Definition: Drugs that increase urine output by inhibiting tubular reabsorption of Na+ (and water follows).
| Class | Drug Examples | Site of Action | Mechanism | Clinical Uses | Side Effects |
|---|---|---|---|---|---|
| Osmotic | Mannitol | PCT + descending loop | Freely filtered, not reabsorbed → osmotic drag of water | ↑ ICP, ↑ IOP, ARF oliguric phase | Volume expansion, pulmonary oedema |
| Carbonic Anhydrase Inhibitors | Acetazolamide | PCT | Inhibit CA → ↓ H+ secretion → ↓ HCO3- reabsorption → NaHCO3 loss | Glaucoma, altitude sickness, metabolic alkalosis | Metabolic acidosis, hypokalaemia |
| Loop diuretics | Furosemide, bumetanide, torasemide | Thick ascending Loop of Henle | Block NKCC2 cotransporter → ↓ NaCl reabsorption; abolish medullary gradient | Pulmonary oedema, heart failure, hypertension, hypercalcaemia | Hypokalaemia, hyponatraemia, ototoxicity, hyperuricaemia, metabolic alkalosis |
| Thiazides | Hydrochlorothiazide, bendroflumethiazide, indapamide | DCT | Block NCC cotransporter → ↓ NaCl reabsorption; ↑ Ca2+ reabsorption | Hypertension (#1 choice), nephrogenic DI (paradox), idiopathic hypercalciuria, heart failure | Hypokalaemia, hyponatraemia, hyperuricaemia, hyperglycaemia, hypercalcaemia, metabolic alkalosis |
| K+-sparing | Spironolactone, eplerenone (aldosterone antagonists); Amiloride, triamterene (ENaC blockers) | Collecting duct | Spironolactone blocks aldosterone receptor → ↓ ENaC expression; Amiloride directly blocks ENaC | Conn's syndrome, heart failure (add-on), combined with loop/thiazide to prevent K+ loss, ascites | Hyperkalaemia, gynaecomastia (spironolactone), metabolic acidosis |
Loop diuretic mechanism detail: Furosemide blocks NKCC2 → ↓ Na+, K+, Cl- reabsorption → ↓ lumen-positive potential → ↓ paracellular Ca2+/Mg2+ reabsorption → hypercalciuria (therapeutic in hypercalcaemia). Also abolishes medullary interstitial gradient → collecting duct cannot concentrate urine even with ADH.
Furosemide acute effect in pulmonary oedema: Before diuresis begins, furosemide causes venodilation (releases vasodilatory prostaglandins) → reduces preload rapidly within minutes → used IV in acute pulmonary oedema.
Sources: Guyton and Hall Textbook of Medical Physiology; Medical Physiology (Boron & Boulpaep); Braunwald's Heart Disease; Brenner and Rector's The Kidney
Ready to continue with Chapter 8: Endocrine System - just say "continue"!
Continue
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.