You are an expert neuroscience educator. Create a logical, step-by-step learning curriculum for a medical student who wants to go from basic brain anatomy to deeply understanding complex cognitive functions (like real-time gaming thinking, strategic reasoning in chess/coding, muscle memory, intuition, and the effects of short-form media on dopamine). The output should be a numbered list of 15-20 topics, arranged from foundational to most advanced. Each topic must be a specific, concrete heading (e.g., “Ion channels and the Action Potential”). Do not explain the topics yet—only list them in order.
- Gross Brain Anatomy: Lobes, Landmarks, and Major Divisions
- Cellular Architecture: Neurons, Glia, and Synaptic Structure
- Ion Channels and the Action Potential
- Synaptic Transmission: Neurotransmitters, Receptors, and Signal Termination
- Neural Circuits: From Reflex Arcs to Local Networks
- Brain Development and Neuroplasticity: Hebbian Learning and Synaptic Pruning
- The Motor System: Cortex, Basal Ganglia, Cerebellum, and Spinal Pathways
- Sensory Processing and Perceptual Encoding: From Receptors to Cortex
- The Limbic System: Emotion, Memory Consolidation, and the Hippocampus
- The Dopaminergic System: Reward Circuitry, Motivation, and Prediction Error
- Attention and Executive Function: The Prefrontal Cortex and Top-Down Control
- Working Memory and Cognitive Load: Capacity, Chunking, and Neural Substrates
- Procedural Learning and Muscle Memory: Striatum, Cerebellum, and Motor Consolidation
- Pattern Recognition and Intuition: The Neuroscience of Expert Heuristics
- The Default Mode Network and Mind-Wandering: Rest, Self-Reference, and Insight
- Real-Time Decision-Making Under Pressure: Neural Speed, Predictive Coding, and Flow States
- Strategic and Abstract Reasoning: Chess, Coding, and Prefrontal-Parietal Networks
- Dopamine Dysregulation and Short-Form Media: Intermittent Reinforcement and Attentional Fragmentation
- Sleep, Memory Consolidation, and Cognitive Performance Optimization
- Metacognition and Conscious Awareness: The Neuroscience of Knowing How You Think
You are an expert neuroanatomist and medical educator. Your task is to teach the gross anatomy of the human brain to a medical student who will later study deep cognitive functions (decision-making, memory, dopamine systems, and high-speed reasoning). Teach from first principles, as if the student has never seen a brain before. Rules: - Explain each structure's location, major landmarks, and key functional role at a high level. - Use text-based diagrams (ASCII or simple lines) where they aid spatial understanding. - Connect each region to a simple "clinical pearl" or a real-life example of what happens when it's damaged. - Do not skip any major division. Explain "why" a structure is located where it is (embryological or evolutionary logic) only if sure; otherwise state "The exact reason is still debated." - If you are uncertain about a fine detail, say so clearly. Structure your response exactly as follows: 1. **Major Divisions** – Cerebrum, Cerebellum, Brainstem, Diencephalon. Define each and their relative positions. 2. **Cerebral Lobes** – For each lobe (Frontal, Parietal, Temporal, Occipital, Insula, Limbic), describe: - Boundaries and key gyri/sulci (e.g., central sulcus, lateral fissure). - One-sentence primary functions (e.g., "Frontal lobe: executive function, motor control"). - A memorable functional hint (e.g., parietal lobe = "where" and "how" pathway). 3. **Deep Gray Matter Structures** – Briefly introduce Basal Ganglia, Thalamus, Hypothalamus, and Hippocampus with location and high-level role (these will be expanded in later lectures). 4. **White Matter Tracts** – Name the corpus callosum, internal capsule, and arcuate fasciculus; explain what they connect and why they matter. 5. **Ventricular System** – What it is, where it sits, and its basic function. 6. **Blood Supply Overview** – Circle of Willis, anterior/middle/posterior cerebral arteries, and which lobe each primarily supplies. 7. **A Clinical Anchor** – End with a brief description of a classic stroke syndrome (e.g., MCA stroke) and how it manifests, tying together the anatomy you just taught. Use simple, precise language. Avoid heavy jargon unless defined. Your goal is to build a mental 3D map the student can refer back to throughout the entire curriculum.
brain lobes cerebral cortex anatomy lateral view
ventricular system brain lateral ventricle third fourth ventricle
circle of Willis anterior middle posterior cerebral artery blood supply
Lecture 1: Gross Anatomy of the Human Brain
Building Your 3D Mental Map
1. Major Divisions
SUPERIOR (top)
┌────────────────────────────────────┐
│ CEREBRUM │ ← newest, outermost
│ (left hemisphere | right hemi) │
│ │
│ DIENCEPHALON (buried inside) │ ← thalamus + hypothalamus
│ │
│ BRAINSTEM │ ← midbrain → pons → medulla
│ │
│ CEREBELLUM (posterior) │ ← hangs off the back
└────────────────────────────────────┘
INFERIOR (toward spinal cord)
| Division | Location | One-line Role |
|---|---|---|
| Cerebrum | Outermost, fills the skull | Higher cognition, voluntary movement, sensation, language |
| Diencephalon | Buried at the core, between cerebrum and brainstem | Relay station (thalamus) and homeostasis hub (hypothalamus) |
| Brainstem | Base of the brain, continuous with spinal cord | Vital autonomic functions (breathing, heart rate, arousal), cranial nerve nuclei |
| Cerebellum | Posterior, tucked under the occipital lobe | Coordination, balance, fine-tuning of movement |
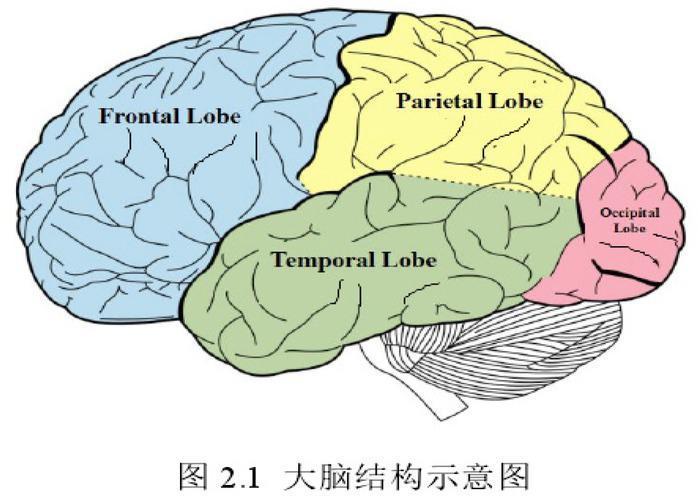
2. Cerebral Lobes
Key Boundary Landmarks (memorize these two first)
Lateral view of one hemisphere:
FRONTAL PARIETAL OCCIPITAL
┌──────────┐ │ ┌──────────┐ ┌──────────┐
│ precentral│ │ │postcentral│ │ │
│ gyrus │ │ │ gyrus │ │ visual │
└──────────┘ │ └──────────┘ │ cortex │
Central sulcus └──────────┘
(boundary Frontal/Parietal)
════════════════════════
Lateral fissure (Sylvian)
════════════════════════
TEMPORAL LOBE (below)
The lateral fissure (Sylvian fissure) runs horizontally and separates frontal/parietal above from temporal below. Deep inside this fissure sits the insula, hidden from surface view.
Frontal Lobe
- Boundaries: Anterior to the central sulcus; above the lateral fissure
- Key gyri: Precentral gyrus (primary motor cortex), superior/middle/inferior frontal gyri; Broca's area (inferior frontal gyrus, left hemisphere)
- Primary function: Executive function, voluntary motor control, working memory, impulse control, language production
- Functional hint: Think of the frontal lobe as the CEO — it plans, initiates, and inhibits
- Clinical pearl: Damage to the prefrontal cortex (front of the frontal lobe) causes personality change and loss of impulse control. Phineas Gage, who survived an iron rod through his frontal lobe in 1848, became impulsive and unable to plan — the first documented evidence of frontal lobe function. Damage to Broca's area (left side) causes Broca's aphasia: the patient understands speech but can only produce halting, effortful words
Parietal Lobe
- Boundaries: Behind the central sulcus, above the lateral fissure; separated from occipital lobe by the parieto-occipital sulcus (visible mainly on the medial surface)
- Key gyri: Postcentral gyrus (primary somatosensory cortex), supramarginal gyrus, angular gyrus
- Primary function: Somatosensory processing (touch, position, pain), spatial awareness, integrating sensory information for action, reading/calculation
- Functional hint: The parietal lobe answers "where is it?" and "how do I interact with it?" — essential for spatial navigation and tool use
- Clinical pearl: Damage to the right parietal lobe causes hemispatial neglect — the patient ignores everything on their left side, even their own left arm. They may shave only the right half of their face or draw a clock with all numbers on the right side
Temporal Lobe
- Boundaries: Below the lateral fissure; extends posteriorly toward occipital lobe
- Key gyri: Superior temporal gyrus (primary auditory cortex + Wernicke's area), hippocampus and parahippocampal gyrus (medial temporal, deep surface), fusiform gyrus (face recognition)
- Primary function: Auditory processing, language comprehension, memory formation, face and object recognition
- Functional hint: The temporal lobe is the brain's "what is it?" lobe — it identifies things by sound, face, and meaning
- Clinical pearl: Damage to Wernicke's area (posterior superior temporal gyrus, left hemisphere) causes Wernicke's aphasia: fluent but meaningless speech ("word salad") — the patient speaks easily but the words are nonsensical. Bilateral medial temporal damage (hippocampus) causes anterograde amnesia — new memories cannot form (as in H.M., the famous amnesiac patient)
Occipital Lobe
- Boundaries: Posterior pole of the hemisphere; no sharp surface boundary anteriorly on the lateral surface (use parieto-occipital sulcus medially as a guide)
- Key gyri: Calcarine sulcus (primary visual cortex, V1, lies along its banks on the medial surface)
- Primary function: Visual processing — from basic edges and motion to complex object recognition
- Functional hint: "Occipital = optical" — destroy it and you go cortically blind, even with intact eyes
- Clinical pearl: A stroke in the posterior cerebral artery (which feeds the occipital lobe) causes homonymous hemianopia — loss of the same visual field in both eyes (e.g., both left visual fields). The patient may not notice initially because the intact side compensates
Insula (Insular Lobe)
- Boundaries: Hidden deep inside the lateral fissure; only visible when the frontal and temporal lobes are pulled apart
- Key gyri: Short and long insular gyri
- Primary function: Interoception (awareness of internal body states — heartbeat, hunger, pain, nausea), taste, empathy, addiction circuitry
- Functional hint: The insula tells you how your body feels from the inside — it's why you feel disgust, craving, or physical discomfort
- Clinical pearl: Insular damage is found in some cases of sudden cardiac death after stroke (it modulates cardiac autonomic activity). It is also a key node in addiction — cravings and the urge to smoke have been dramatically reduced by insular lesions
Limbic Lobe (Limbic System)
- Boundaries: A ring of cortex on the medial surface of each hemisphere, encircling the corpus callosum
- Key structures: Cingulate gyrus (above corpus callosum), parahippocampal gyrus, hippocampus (technically buried in medial temporal), amygdala
- Primary function: Emotion, motivation, memory encoding, olfaction; connects primitive drives with higher cognition
- Functional hint: The limbic system is the bridge between "I feel" and "I think" — it tags experiences with emotional valence so you remember what matters
- Clinical pearl: Bilateral amygdala damage (Urbach-Wiethe disease) causes fearlessness — patients cannot recognize fearful faces and do not feel fear even when threatened, demonstrating the amygdala's role in emotional learning
3. Deep Gray Matter Structures
Coronal cross-section (looking from the front):
Left hemisphere Right hemisphere
┌──────────────────────────────────────┐
│ Cortex Cortex │
│ │
│ Caudate ┐ ┌ Caudate │
│ Putamen ├ BASAL GANGLIA ├ Putamen │
│ Globus ┘ └ Globus │
│ pallidus THALAMUS pallidus │
│ ┌──────────┐ │
│ │ 3rd vent │ │
│ │ THALAMUS │ │
│ └──────────┘ │
│ HYPOTHALAMUS (below) │
└──────────────────────────────────────┘
| Structure | Location | High-Level Role |
|---|---|---|
| Basal Ganglia (caudate, putamen, globus pallidus, subthalamic nucleus, substantia nigra) | Deep in each cerebral hemisphere, flanking the thalamus | Motor control, habit formation, reward processing, procedural learning — the "action selector" of the brain |
| Thalamus | Dead center of the brain, two egg-shaped masses flanking the 3rd ventricle | The grand relay station — nearly all sensory information (except smell) passes through here before reaching cortex |
| Hypothalamus | Below the thalamus, above the pituitary stalk | Master regulator of homeostasis: hunger, thirst, temperature, circadian rhythm, hormones via the pituitary |
| Hippocampus | Curved, seahorse-shaped structure buried in the medial temporal lobe | New memory formation (converts short-term to long-term memory), spatial navigation |
These four will each get their own dedicated lectures. For now, anchor them spatially: thalamus and hypothalamus = deep center; basal ganglia = flanking the thalamus; hippocampus = medial temporal
4. White Matter Tracts
Top-down view (axial):
LEFT HEMISPHERE ←────── CORPUS CALLOSUM ──────→ RIGHT HEMISPHERE
(connects them)
Frontal cortex
│
│ INTERNAL CAPSULE
│ (like a bottleneck)
▼
Brainstem / Spinal cord
(motor and sensory fibers pass here)
Broca's area ←──── ARCUATE FASCICULUS ────→ Wernicke's area
(connects language areas)
Corpus Callosum
- What it is: The brain's largest white matter commissure — a thick band of ~200 million axons bridging the two hemispheres
- Why it matters: Every time your left hand and right brain need to cooperate, the corpus callosum carries the message. Severing it (split-brain surgery for epilepsy) creates two semi-independent hemispheres — patients can literally not say the name of an object shown only to their left visual field
Internal Capsule
- What it is: A dense, V-shaped bundle of fibers compressed between the basal ganglia and thalamus; the main highway connecting cortex to spinal cord (and vice versa)
- Why it matters: Motor fibers from the entire cortex converge here. A tiny stroke in the posterior limb of the internal capsule (a region the size of a grape) can paralyze an entire side of the body — contralateral hemiplegia
Arcuate Fasciculus
- What it is: A curved white matter tract connecting Broca's area (frontal, language production) to Wernicke's area (temporal, language comprehension) in the left hemisphere
- Why it matters: Damage here causes conduction aphasia — the patient can understand speech and can produce fluent speech, but cannot repeat words accurately, because the connection between understanding and production is severed
5. Ventricular System
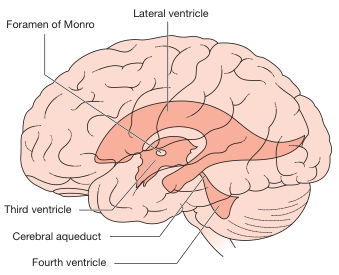
CSF Flow Path:
LATERAL VENTRICLES (×2, in each hemisphere)
│
▼ Foramen of Monro
3RD VENTRICLE (between the two thalami)
│
▼ Cerebral Aqueduct (of Sylvius, through midbrain)
4TH VENTRICLE (between pons/medulla and cerebellum)
│
▼ Foramina of Luschka & Magendie
SUBARACHNOID SPACE (surrounds entire brain & spinal cord)
│
▼ Arachnoid granulations
VENOUS SINUSES (CSF reabsorbed)
6. Blood Supply Overview
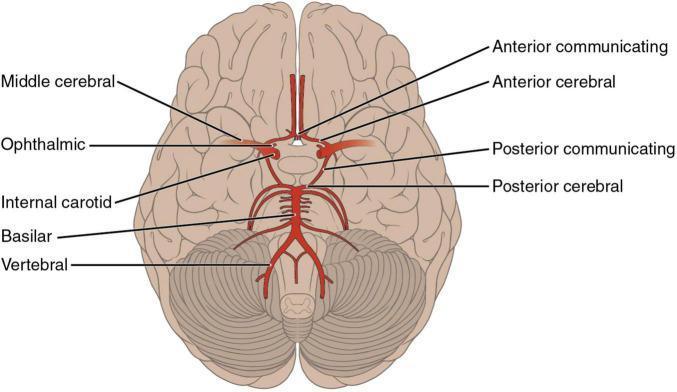
The Circle of Willis
- Anterior circulation (from Internal Carotid Arteries, ICA): feeds ~80% of the brain
- Posterior circulation (from Vertebral → Basilar artery): feeds brainstem, cerebellum, occipital and inferior temporal lobes
- Communicating arteries (anterior and posterior): the "safety bridges" that allow collateral flow if one artery is blocked
ACA ──── ACA
| |
ICA ── ACoA ──── ACoA ── ICA
| |
MCA MCA
| |
PCoA ──────── PCoA
| |
PCA PCA
│
Basilar
│
Vertebrals (×2)
The Three Main Territories
| Artery | Territory | What you lose if blocked |
|---|---|---|
| ACA (Anterior Cerebral Artery) | Medial surface of frontal and parietal lobes | Contralateral weakness predominantly of the leg (the leg's motor/sensory cortex is medial); personality/behavioral changes |
| MCA (Middle Cerebral Artery) | Lateral surface of frontal, parietal, temporal lobes; deep structures via lenticulostriate branches | Contralateral weakness of face and arm > leg; aphasia (left MCA); neglect (right MCA); gaze deviation toward the lesion |
| PCA (Posterior Cerebral Artery) | Occipital lobe, medial temporal, thalamus | Contralateral homonymous hemianopia; memory loss (medial temporal); thalamic syndromes |
7. Clinical Anchor: The MCA Stroke
Scenario
Anatomy Unpacked
| Finding | Structure damaged | Why |
|---|---|---|
| Right arm and face weakness (not leg) | Left MCA → lateral motor cortex (precentral gyrus) — arm/face representation is lateral; leg is medial | The cortical homunculus maps body parts; MCA covers lateral cortex |
| Aphasia (cannot speak or comprehend) | Left hemisphere MCA supplies Broca's (frontal) and Wernicke's (temporal) areas | Language is left-lateralized in ~95% of right-handed people |
| Eye deviation to the left (toward lesion) | Frontal eye fields (in left frontal lobe) destroyed; unopposed right side pushes gaze left | The frontal eye fields drive the eyes contralaterally; losing the left field leaves gaze driven right-ward — wait, correction: eyes deviate toward the side of the lesion because the intact contralateral frontal eye fields push the eyes toward the damaged side |
| Right face droop (lower face only) | Upper motor neuron lesion to the facial motor cortex | The upper face has bilateral cortical representation; only the lower face shows contralateral UMN weakness |
Summary Stroke Map
Summary: Your 3D Mental Map
CEREBRUM (outermost)
├── Frontal: CEO, motor, language output (Broca's)
├── Parietal: Where/how, touch, space
├── Temporal: What, hearing, memory, language input (Wernicke's)
├── Occipital: Vision
├── Insula: Body feelings, craving
└── Limbic: Emotion, memory tagging
DEEP STRUCTURES (buried inside)
├── Basal Ganglia: Action selection, habits, reward
├── Thalamus: Relay gate for all senses
├── Hypothalamus: Body homeostasis
└── Hippocampus: New memory formation
WHITE MATTER HIGHWAYS
├── Corpus callosum: Left ↔ Right
├── Internal capsule: Cortex ↔ Spinal cord (BOTTLENECK)
└── Arcuate fasciculus: Broca's ↔ Wernicke's
BLOOD SUPPLY
├── ACA → medial surfaces (leg)
├── MCA → lateral surfaces (arm, face, language)
└── PCA → occipital + thalamus (vision, memory)
BRAINSTEM + CEREBELLUM (below all of the above)
├── Brainstem: Life support, cranial nerves
└── Cerebellum: Movement tuning, coordination
You are an expert neurophysiologist and medical educator. Your task is to teach the cellular architecture of the brain and the action potential in a single integrated lecture. Build on the previous lecture's anatomy, and now go microscopic. Rules: - Start with the neuron: its parts (soma, dendrites, axon, axon hillock, terminals) and explain *why* each part's structure serves its function (e.g., why dendrites have spines, why axon hillock is the decision point). - Then explain the resting membrane potential: ionic gradients (Na+, K+, Cl-, Ca2+), the Na+/K+ pump, leak channels, and the concept of equilibrium potential. Use the Nernst equation conceptually (no need for calculation, just explain what it means). - Explain the action potential step-by-step: threshold, rising phase (Na+ influx), falling phase (K+ efflux), after-hyperpolarization, back to resting. Link each phase to specific voltage-gated ion channel states (closed, open, inactivated). - Cover absolute and relative refractory periods, and why they ensure unidirectional propagation and limit firing rate. - Describe saltatory conduction and the role of myelin (oligodendrocytes in CNS, Schwann cells in PNS) and nodes of Ranvier. - Introduce glial cells (astrocytes, microglia, oligodendrocytes/Schwann cells) and their roles: tripartite synapse, blood-brain barrier, immune defense, myelination. - For each concept, give a clinical or real-world pearl: e.g., multiple sclerosis and demyelination, local anesthetics (lidocaine) blocking voltage-gated Na+ channels, hyperkalemia's effect on resting potential. - Connect back to the gross anatomy from the last lecture: e.g., white matter = myelinated axons, gray matter = cell bodies and synapses. - Use text-based diagrams if you cannot display images. But visual markers are allowed if you can generate them. - At the end, ask one integrative question for the student to test their understanding (do not give the answer). Depth: Go as deep as possible without becoming speculative. If a mechanism is debated, say "Some evidence suggests..." and give the mainstream view.
neuron anatomy soma dendrite axon hillock axon terminal structure
action potential graph voltage gated sodium potassium channel phases
myelinated axon saltatory conduction nodes of Ranvier oligodendrocyte