Glaucoma in detail
Reading File
Finding Sources
Searching PubMed
glaucoma diagnosis management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full detailed response.
Glaucoma - A Comprehensive Review
Definition
Glaucoma is a group of conditions that share a common endpoint: a chronic, progressive optic neuropathy causing characteristic morphological changes at the optic nerve head and retinal nerve fiber layer (RNFL), with progressive retinal ganglion cell (RGC) death and visual field loss. Intraocular pressure (IOP) is the key modifiable risk factor, though not a prerequisite - some patients develop identical changes with normal IOP (normal-tension glaucoma).
The goal of glaucoma treatment is to slow the rate of progression throughout a patient's lifetime to maintain visual function and quality of life, at a sustainable cost.
- Kanski's Clinical Ophthalmology, 10th ed.
Aqueous Humor Dynamics - The Foundation
Understanding glaucoma requires understanding aqueous humor flow:
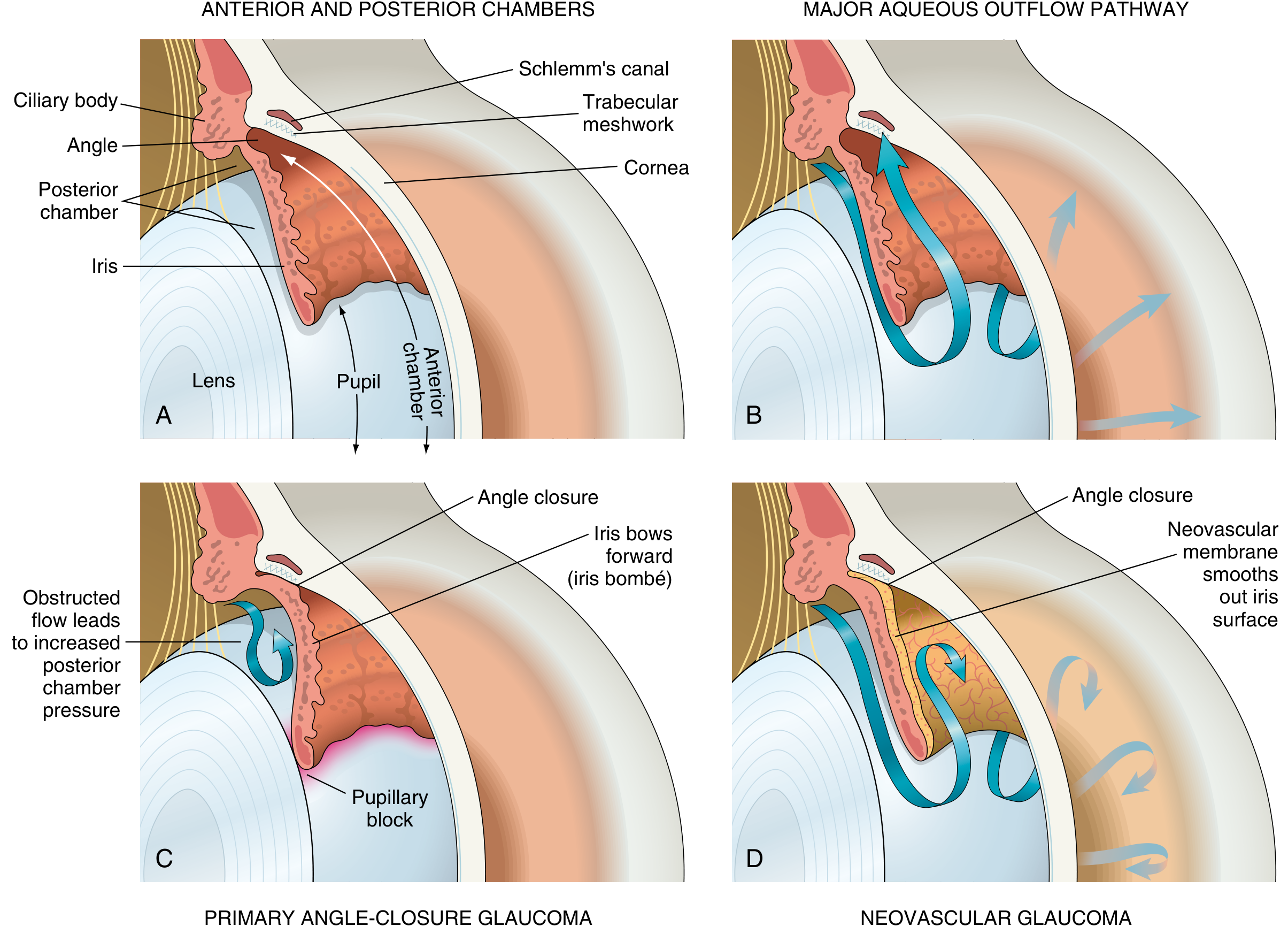
Fig. A: Normal eye anatomy; B: Normal aqueous flow through trabecular meshwork → Schlemm's canal; C: Primary angle-closure (iris bombé, pupillary block); D: Neovascular glaucoma (fibrovascular membrane occludes angle)
Aqueous humor is produced by the ciliary body epithelium and flows:
- Posterior chamber → through the pupil → anterior chamber
- Primary outflow (80-90%): Trabecular meshwork → Schlemm's canal → episcleral veins (conventional/pressure-sensitive)
- Secondary outflow (10-20%): Uveoscleral pathway (pressure-independent)
Normal IOP: 10-21 mmHg (statistical definition). IOP depends on the balance between aqueous production and outflow. Elevated IOP results from impaired drainage, not increased production, in the vast majority of cases.
Classification
1. By Mechanism
| Type | Angle | Primary | Secondary |
|---|---|---|---|
| Open-angle glaucoma | Open | POAG | Pseudoexfoliation, pigmentary, steroid-induced, uveitic, traumatic |
| Angle-closure glaucoma | Closed | PACG | Neovascular, phacomorphic, phacolytic, malignant |
| Developmental | - | Congenital/infantile | Associated with aniridia, Sturge-Weber, NF1 |
Primary Open-Angle Glaucoma (POAG)
Epidemiology
- Most common form worldwide; affects ~3.5% of the global population >40 years
- Leading cause of irreversible blindness globally
- Risk factors: elevated IOP, positive family history, African/African-Caribbean ancestry, increasing age, myopia, thin corneal thickness (CCT), diabetes, systemic hypertension
- GWAS has identified >40 gene loci associated with POAG
Pathogenesis
The aqueous has complete physical access to the trabecular meshwork, but outflow resistance is abnormally elevated. The exact cause is unknown - theories include:
- Dysfunction of trabecular meshwork cells (decreased phagocytic activity, accumulation of extracellular debris)
- Loss of cellularity with aging
- Increased deposition of fibronectin, laminin, and other extracellular matrix proteins
- Genetic factors (MYOC, OPTN, TBK1 mutations)
Clinical Features
POAG is an insidious, asymptomatic disease until late stages. There is no pain. Visual field loss begins peripherally (nasal step, arcuate scotoma) and only threatens central vision late. By the time a patient notices vision loss, approximately 30-50% of RGCs may already be lost.
IOP Assessment
- Measured by Goldmann applanation tonometry (gold standard)
- Corrected for central corneal thickness (CCT): Thin corneas give falsely low readings; thick corneas give falsely high readings
- Normal CCT: 540-560 μm; CCT < 500 μm is an independent risk factor for POAG
- Diurnal variation of IOP (up to 5 mmHg over 24 hours) is relevant - IOP peaks in early morning
Optic Disc and RNFL Changes in Glaucoma
Glaucomatous damage produces characteristic findings at three sites:
1. Optic Nerve Head (ONH)
- Pathological cupping: Irreversible loss of nerve fibers, glia, and blood vessels → increased cup-to-disc ratio (CDR)
- Normal CDR: up to 0.5 (though this varies with disc size - large discs have larger physiological cups)
- Neuroretinal rim (NRR) thinning - typically follows the ISNT rule (Inferior > Superior > Nasal > Temporal in health). Glaucoma preferentially attacks inferior and superior poles first.
- NRR notching (focal loss) is the most specific sign
2. Disc Haemorrhages
- Small, flame-shaped haemorrhages at the NRR margin (most commonly inferotemporal)
- Highly significant - indicate active damage and predict progression
- More common in normal-tension glaucoma (NTG)
3. Four Morphological Glaucomatous Disc Patterns (Kanski):
- Focal ischaemic: Localized superior/inferior notching; arcuate field defects threatening fixation early
- Myopic disc with glaucoma: Tilted, obliquely inserted disc; temporal crescent; dense superior/inferior scotomas; younger males
- Sclerotic: Shallow saucerized cup; gently sloping NRR; associated with systemic vascular disease; older patients
- Concentrically enlarging: Uniform NRR thinning; diffuse visual field loss; significantly elevated IOP at presentation
4. RNFL Changes
- Detectable before visual field loss by approximately 5 years
- Localized wedge-shaped RNFL defects on red-free fundus photography
- Measured quantitatively by OCT (Optical Coherence Tomography) - now the standard imaging tool
Imaging in Glaucoma
Optical Coherence Tomography (OCT)
The current standard for structural monitoring. Measures:
- Peripapillary RNFL thickness (circumpapillary scan)
- Macular ganglion cell complex (GCC) thickness
- ONH parameters (rim area, CDR, disc area)
- Allows detection of pre-perimetric glaucoma (structural damage without field loss)
- Serial OCT enables detection of progression before functional testing
Visual Field Testing (Perimetry)
- Standard automated perimetry (SAP) using Humphrey Field Analyzer (HFA)
- 24-2 pattern - standard for glaucoma monitoring (tests within 24° temporally, 30° nasally)
- 10-2 pattern - detects central defects; used in advanced glaucoma with split fixation
- 30-2 pattern - alternative to 24-2
- Characteristic field defects:
- Nasal step (respects horizontal midline)
- Arcuate (Bjerrum) scotoma (arches from blind spot to nasal midline)
- Paracentral scotoma
- Altitudinal defect (superior > inferior)
- Tubular/central island (late stage)
Other Imaging
- Gonioscopy - direct visualization of the anterior chamber angle; essential to classify open vs. closed angle
- Ultrasound biomicroscopy (UBM) - images structures behind the iris (ciliary body); particularly useful for angle-closure glaucoma
- Anterior segment OCT - evaluates angle anatomy; useful for angle-closure subtypes; non-contact
- Stereo disc photography - historical gold standard; still valuable for qualitative documentation
Normal-Tension Glaucoma (NTG)
Definition
Glaucomatous optic neuropathy with IOP consistently ≤21 mmHg on diurnal testing, open angle, and no secondary cause. Depending on ethnicity, 30-65% of open-angle glaucoma patients may have normal IOP at initial presentation.
Pathogenesis
- IOP-independent vascular and mechanical factors are more prominent
- Proposed mechanisms: anomalies of local/systemic vascular regulation, structural optic nerve vulnerability, autoimmune processes
- Thin CCT accounts for a proportion of cases (falsely low tonometry)
Risk Factors
- Older age (tends to present later than POAG)
- Female sex
- Japanese ethnicity (more prevalent)
- Family history
- Nocturnal systemic hypotension (>20% BP dip) - especially in patients on antihypertensives
- Migraine, Raynaud phenomenon (vascular dysregulation)
- Obstructive sleep apnoea
- Low serum retinol
- OPTN gene mutations (optineurin)
Management
- IOP reduction remains the mainstay even in NTG (lowers risk of progression)
- Target IOP typically set 20-30% below baseline
- Consider systemic vascular risk factor management
- Calcium channel blockers (e.g., nifedipine) may have a neuroprotective role in NTG with vascular dysregulation
Primary Angle-Closure Glaucoma (PACG)
Epidemiology
More common in Asians (particularly Chinese), females, hyperopes, and older individuals. The mechanism involves pupillary block in anatomically predisposed eyes.
Anatomy
Predisposing features: small eye, shallow anterior chamber, anteriorly positioned iris-lens diaphragm, short axial length.
Mechanism (see diagram above)
- Iris apposition to the lens at the pupil margin blocks aqueous flow from posterior to anterior chamber
- Pressure builds in the posterior chamber → iris bows forward (iris bombé)
- Peripheral iris occludes the trabecular meshwork
- IOP rises dramatically → acute angle-closure crisis
Acute Angle-Closure Crisis (AACC)
Emergency - vision-threatening!
- Sudden onset of severe ocular pain (periorbital), headache, nausea/vomiting
- Blurred vision with coloured halos around lights
- Red eye
- Markedly elevated IOP (often 40-70 mmHg)
- Corneal oedema (hazy, steamy cornea)
- Fixed, mid-dilated (4-6 mm), oval pupil
- Shallow anterior chamber
- Ciliary injection
Emergency management:
- Immediate IOP reduction: acetazolamide 500 mg IV/oral + topical beta-blocker + topical steroid
- Pilocarpine 2-4% (once IOP < 40 mmHg, as ischaemic iris is unresponsive at higher pressures)
- Laser peripheral iridotomy (LPI) - definitive treatment; creates a hole in the peripheral iris to bypass pupillary block; also performed prophylactically in the fellow eye
- Systemic hyperosmotic agents if needed (glycerol, mannitol)
Chronic Angle-Closure Glaucoma
Repeated episodes of iridotrabecular contact → peripheral anterior synechiae (PAS) → gradually elevated IOP without dramatic symptoms.
Secondary Glaucomas
Pseudoexfoliation Glaucoma (PXG)
- Most common identifiable cause of secondary open-angle glaucoma worldwide
- White fibrillar material (pseudoexfoliative material) deposits on the lens capsule, zonules, corneal endothelium, and trabecular meshwork
- Associated with fibrillin gene (FBN1) and LOXL1 mutations
- Significantly higher IOP, more asymmetric, worse prognosis than POAG
- Higher rate of vitreous loss during cataract surgery (zonular weakness)
Pigmentary Glaucoma
- Predominantly young myopic males
- Iris transillumination defects (radial spoke-like pattern at mid-peripheral iris)
- Pigment deposits on corneal endothelium (Krukenberg spindle) and trabecular meshwork
- IOP rises after exercise or pupillary dilation (pigment release)
- May "burn out" with age as iris pigment is exhausted
Steroid-Induced Glaucoma
- Topical, periocular, systemic, or intravitreal steroids
- Mechanism: steroids increase glycosaminoglycan deposition in the trabecular meshwork → reduced outflow
- ~35% of the general population are "steroid responders"
- IOP typically normalizes after discontinuing steroids
Neovascular Glaucoma (NVG)
- New abnormal blood vessels (rubeosis iridis) grow over the trabecular meshwork
- Common causes: diabetic retinopathy, central retinal vein occlusion, ocular ischaemic syndrome
- Fibrovascular membrane contracts → peripheral anterior synechiae → completely closed angle
- Treatment: anti-VEGF + panretinal photocoagulation (PRP) to address the ischaemic stimulus + glaucoma surgery
Inflammatory (Uveitic) Glaucoma
- Trabeculitis, trabecular meshwork blockage by inflammatory cells/debris
- Posterior synechiae → pupillary block → "seclusio pupillae" → iris bombé
- Secondary angle closure from extensive PAS
- Treatment: treat underlying uveitis + IOP lowering (avoid prostaglandins in active inflammation; avoid miotics if posterior synechiae)
Traumatic Glaucoma
- Angle recession glaucoma: Tear between the circular and longitudinal ciliary muscle fibres after blunt trauma. Long-latent (years). Requires lifelong monitoring.
- Ghost cell glaucoma: Red blood cell ghosts (degenerated RBCs) clog trabecular meshwork after vitreous haemorrhage
- Lens-related: Phacolytic (lens proteins leak from hypermature cataract), phacomorphic (intumescent lens causes angle closure)
Developmental (Congenital) Glaucoma
Primary Congenital Glaucoma
- Trabeculodysgenesis (Barkan's membrane or abnormal trabecular development)
- Presents at birth to age 3 years
- Classic triad: Epiphora, photophobia, blepharospasm
- Buphthalmos (enlarged globe) - corneal diameter >13 mm; Haab's striae (horizontal breaks in Descemet's membrane)
- Treatment: goniotomy or trabeculotomy (primary surgical; medical treatment only temporizing)
- AR inheritance in ~10%; CYP1B1 gene mutations are most common
Glaucoma in Phacomatoses
- Sturge-Weber syndrome: Glaucoma in ~30% of cases ipsilateral to facial haemangioma. Infants may develop buphthalmos (trabeculodysgenesis). Older patients: elevated episcleral venous pressure from episcleral haemangioma. Medical or surgical (combined trabeculotomy-trabeculectomy) treatment; risk of choroidal effusion.
- Neurofibromatosis type 1: Rare unilateral congenital glaucoma; ~50% have plexiform neurofibroma of the upper eyelid on the same side.
Pharmacological Treatment
Step 1 (First-line): Prostaglandin Analogues (PGAs)
Currently first-line agents due to once-daily dosing, potent IOP lowering (25-33%), and low systemic side effect profile.
Drugs: Latanoprost (0.005%), bimatoprost (0.03%), travoprost (0.004%), tafluprost, latanoprostene bunod
Mechanism: Act at FP receptors (Gα₁₁-PLC-IP₃-Ca²⁺ pathway) → increase uveoscleral outflow (and possibly trabecular outflow via matrix metalloproteinase release). Latanoprostene bunod additionally donates nitric oxide → relaxes trabecular meshwork cytoskeleton → enhances conventional outflow.
Side effects (local):
- Irreversible darkening of iris (brown pigmentation)
- Hypertrichosis (increased eyelash length/pigmentation)
- Periorbital fat atrophy (deepened upper lid sulcus)
- Conjunctival hyperaemia
- Cystoid macular oedema (rare; use with caution in aphakia/pseudophakia)
- Reactivation of uveitis/herpes - use cautiously
Step 2: Beta-Adrenergic Antagonists (Beta-Blockers)
Drugs: Timolol (0.25%, 0.5%), levobunolol, carteolol (non-selective); betaxolol (β₁-selective)
Mechanism: Reduce aqueous humor production by blocking β₂ receptors on ciliary body epithelium → decrease cAMP-PKA pathway activation
IOP reduction: ~20-25%
Systemic side effects (significant):
- Bradycardia, heart block
- Bronchoconstriction (avoid in asthma/COPD)
- Masking of hypoglycaemia symptoms
- CNS effects (depression, fatigue)
- Betaxolol (β₁-selective) is safer in respiratory disease but less efficacious
Contraindications: Asthma, COPD, 2nd/3rd degree heart block, decompensated heart failure, bradycardia
Step 3: Alpha-2 Adrenergic Agonists
Drugs: Brimonidine (0.1-0.2%), apraclonidine
Mechanism: Reduce aqueous production (presynaptic α₂ activation) + enhance uveoscleral outflow; may have a direct neuroprotective effect (brimonidine crosses blood-brain barrier)
IOP reduction: ~20-25%
Side effects: Allergic conjunctivitis (common, ~15%), dry mouth, fatigue; CNS sedation in infants (contraindicated in children < 2 years - apnoea risk)
Step 4: Carbonic Anhydrase Inhibitors (CAIs)
Topical drugs: Dorzolamide (2%), brinzolamide (1%)
Systemic drugs: Acetazolamide (oral/IV), methazolamide
Mechanism: Inhibit carbonic anhydrase II and IV in ciliary body epithelium → reduce bicarbonate formation → reduce aqueous humor production
IOP reduction: ~15-20%
Topical side effects: Bitter taste, corneal toxicity (avoid with corneal endothelial disease)
Systemic side effects of acetazolamide: Metabolic acidosis, hypokalaemia, paraesthesiae, nephrolithiasis, aplastic anaemia (rare), sulphonamide hypersensitivity
Contraindication: Sulphonamide allergy, severe renal impairment, sickle cell disease
Step 5: Rho-Kinase (ROCK) Inhibitors (Newer Class)
Drug: Netarsudil (0.02%)
Mechanism: Inhibit Rho-kinase → relax trabecular meshwork cells → increase conventional outflow. Also reduce episcleral venous pressure and aqueous production.
Combination: Netarsudil/latanoprost (Rocklatan) - additive effects via complementary mechanisms
Side effects: Conjunctival hyperaemia (common), cornea verticillata (reversible whorl-like corneal deposits), subconjunctival haemorrhage
Miotics (Cholinergic Agents)
Drug: Pilocarpine (1-4%)
Mechanism: Contracts the ciliary muscle → opens trabecular meshwork pores → increases conventional outflow; also contracts the sphincter pupillae (miosis)
Use now: Mainly in angle-closure (acute and chronic) and as adjunct; rarely used long-term due to side effects
Side effects: Brow ache (ciliary spasm), myopia (accommodation), dim vision (miosis), retinal detachment risk (lattice degeneration), systemic cholinergic effects
Fixed Combination Drops
- Latanoprost/timolol (Xalacom)
- Dorzolamide/timolol (Cosopt)
- Brimonidine/timolol (Combigan)
- Bimatoprost/timolol (Ganfort)
- Netarsudil/latanoprost (Rocklatan)
Improve adherence; no preservative washout between drops needed.
Surgical and Laser Treatment
Laser
- Laser Peripheral Iridotomy (LPI): Definitive treatment for angle-closure (pupillary block); creates an aqueous bypass channel through the peripheral iris using Nd:YAG laser
- Selective Laser Trabeculoplasty (SLT): Applies 532 nm laser to trabecular meshwork; stimulates macrophage-mediated trabecular remodelling; IOP reduction ~25%; repeatable; now considered a first-line option (equal to medical therapy in the LiGHT trial); no thermal damage to meshwork
- Argon Laser Trabeculoplasty (ALT): Older; causes coagulative damage to meshwork; less favoured than SLT
- Diode laser cyclodestruction (cycloablation): Destroys ciliary body epithelium; used in refractory cases or poor surgical candidates
Filtration Surgery
- Trabeculectomy: Gold standard incisional surgery; creates a guarded fistula (bleb) allowing aqueous to drain under the conjunctiva; antimetabolites (Mitomycin-C, 5-Fluorouracil) enhance bleb survival by reducing fibrosis
- Complications: Bleb failure, bleb-related endophthalmitis, hypotony maculopathy, cataract, malignant glaucoma
- Combined trabeculectomy-trabeculotomy: Used in developmental glaucoma
Glaucoma Drainage Devices (Tubes)
- Baerveldt, Ahmed, Molteno implants
- Route aqueous to a posterior equatorial plate via a tube in the anterior chamber
- Used in refractory cases, uveitic glaucoma (better success than trabeculectomy per recent meta-analysis), previous failed trabeculectomy, aniridia
- A 2024 systematic review (PMID 39293570) comparing trabeculectomy vs. tube shunts in uveitic glaucoma found comparable IOP control but different complication profiles
Minimally Invasive Glaucoma Surgery (MIGS)
- Performed at the time of cataract surgery or as standalone
- Targets include: Schlemm's canal (iStent inject, Hydrus microstent), suprachoroidal space (CyPass, iStent Supra), subconjunctival space (XEN gel stent)
- Lower risk profile than trabeculectomy but moderate IOP reduction (~20-30%)
- Best suited for mild-moderate glaucoma
Optic Nerve Neuroprotection
The optic nerve damage in glaucoma involves two key mechanisms:
- Mechanical: Direct compression of axons and vessels at the lamina cribrosa by elevated IOP
- Vascular: Impaired ocular blood flow, reduced perfusion, ischaemia of the optic nerve head
Glaucomatous RGC death follows an apoptotic pathway. Despite much research, no neuroprotective agent beyond IOP lowering has been proven effective in clinical trials. Areas of active research include:
- NMDA receptor antagonists (memantine - failed in phase III trial)
- Neurotrophic factors (BDNF, CNTF)
- Mitochondrial protection
- Stem cell therapy
Monitoring and Targets
| Parameter | Method | Frequency |
|---|---|---|
| IOP | Goldmann applanation tonometry | 3-6 monthly when stable |
| Optic disc | Stereo photography / OCT | 6-12 monthly |
| RNFL/GCC | OCT | 6-12 monthly |
| Visual fields | SAP 24-2 / 10-2 | At least 2x/year in early; 2-3x/year when unstable |
Target IOP is set individually based on:
- Baseline IOP and level of damage
- Rate of progression
- Patient age and life expectancy
- As a general rule: 30% reduction from baseline for POAG; lower targets (8-12 mmHg) for NTG or advanced damage
The EMGT, AGIS, CNTGS, and OHTS trials collectively established that IOP reduction reduces the risk of glaucoma onset and progression. Every 1 mmHg reduction in IOP reduces the risk of progression by approximately 10%.
Malignant Glaucoma (Aqueous Misdirection)
A rare but serious complication, most commonly after filtration surgery in hyperopic eyes. Aqueous is misdirected posteriorly into or behind the vitreous → pushes the lens-iris diaphragm forward → very shallow anterior chamber + raised IOP. Distinct from pupillary block (LPI does not help). Treatment: cycloplegics (atropine), aqueous suppressants; Nd:YAG laser disruption of the anterior vitreous face; vitrectomy in resistant cases.
Key Summary Table
| Feature | POAG | PACG | NTG |
|---|---|---|---|
| IOP | Elevated (but can be normal) | Markedly elevated acutely | ≤21 mmHg |
| Angle | Open | Closed | Open |
| Symptoms | None (insidious) | Acute: severe pain, red eye, nausea | None (insidious) |
| Optic disc | Classic glaucomatous cupping | As per POAG | Disc haemorrhages more common |
| Visual field | Arcuate/nasal step | Rapid loss if untreated | Same pattern, often denser near fixation |
| First-line Rx | PGA drops / SLT | LPI (laser iridotomy) | IOP reduction ± vascular Rx |
| Prevalence | Most common | High in Asians | Up to 65% of OAG in Japanese |
Sources used:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed. - Primary reference throughout
- Robbins & Kumar Basic Pathology and Robbins, Cotran & Kumar Pathologic Basis of Disease - Pathogenesis and morphology
- Goodman & Gilman's The Pharmacological Basis of Therapeutics - Drug mechanisms
- Katzung's Basic and Clinical Pharmacology, 16th ed. - Prostaglandin analogues and beta-blockers
- Recent evidence: Trabeculectomy vs. tube shunts in uveitic glaucoma (2024, PMID 39293570)
This is a shared conversation. Sign in to Orris to start your own chat.