Diabetes Mellitus
Reading File
Asking for Preferences
Everything
Finding Sources
Finding Sources
Searching PubMed
"diabetes mellitus"[MeSH Terms] AND "management"[MeSH Terms]
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Diabetes Mellitus - Comprehensive Review
Sources: Harrison's Principles of Internal Medicine 22E (2025), Guyton & Hall Textbook of Medical Physiology, Creasy & Resnik's Maternal-Fetal Medicine, Textbook of Family Medicine 9e, Tietz Textbook of Laboratory Medicine 7E, Tintinalli's Emergency Medicine
1. Definition & Overview
Diabetes mellitus (DM) is a group of metabolic diseases characterized by hyperglycemia resulting from defects in insulin secretion, insulin action, or both. Chronic hyperglycemia leads to long-term damage, dysfunction, and failure of multiple organ systems - especially the eyes, kidneys, nerves, heart, and blood vessels.
2. Pancreatic Anatomy & Normal Physiology
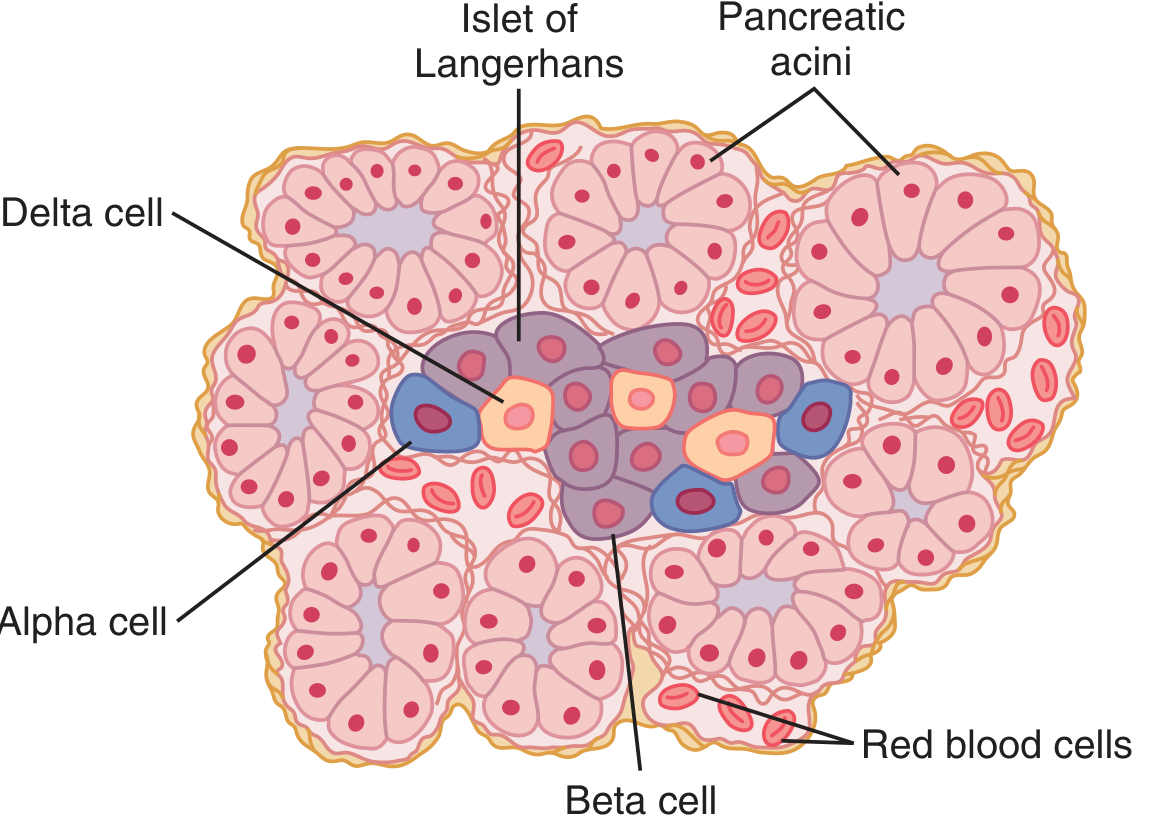
The human pancreas contains 1-2 million islets of Langerhans, each about 0.3 mm in diameter. Cell composition:
| Cell Type | Proportion | Hormone Secreted |
|---|---|---|
| Beta (B) cells | ~60% | Insulin + Amylin (IAPP) |
| Alpha (A) cells | ~25% | Glucagon |
| Delta (D) cells | ~10% | Somatostatin |
| PP cells | Small numbers | Pancreatic polypeptide |
Key regulatory interactions: insulin inhibits glucagon secretion; amylin inhibits insulin secretion; somatostatin inhibits both insulin and glucagon.
Insulin secretion is triggered by energy abundance (especially carbohydrate intake). Its metabolic effects include:
-
Stimulating glycogen synthesis in liver and muscle
-
Inhibiting hepatic gluconeogenesis and glycogenolysis
-
Promoting fatty acid synthesis and fat storage
-
Stimulating protein anabolism
-
Facilitating glucose uptake in peripheral tissues (muscle, fat) via GLUT4 transporters
-
Guyton & Hall Textbook of Medical Physiology, p. 965
3. Classification (ADA)
The ADA classifies DM into four main types:
Type 1 DM (T1DM)
- Due to autoimmune beta-cell destruction leading to absolute insulin deficiency
- Accounts for 5-10% of all DM
- Markers of autoimmune destruction: islet cell autoantibodies, anti-insulin antibodies, anti-GAD65 antibodies, anti-IA2 antibodies
- Genetically susceptible individuals + environmental trigger (enteroviruses implicated)
-
60 genetic loci identified, many implicating the immune system
- No sex difference in incidence
Type 2 DM (T2DM)
- Due to progressive loss of beta-cell insulin secretion on the background of insulin resistance
- Accounts for ~90-95% of all DM
- Strong genetic component; polygenic; influenced by obesity, physical inactivity, age
Gestational DM (GDM)
- Diabetes diagnosed in pregnancy that was not clearly overt diabetes prior to gestation
- Associated with polycystic ovary syndrome, preeclampsia, and pregnancy hypertension
Other Specific Types
-
Monogenic diabetes - MODY (maturity-onset diabetes of the young), neonatal diabetes
-
Exocrine pancreatic disease - cystic fibrosis, pancreatitis, pancreatic cancer
-
Drug/chemical-induced - glucocorticoids, HIV/AIDS treatment, post-organ transplantation
-
Creasy & Resnik's Maternal-Fetal Medicine; Harrison's Principles of Internal Medicine 22E
4. Pathophysiology
Type 1 DM
T1DM is a chronic autoimmune disease in which immune-mediated destruction of (or damage to) beta-cells results in insulin deficiency and hyperglycemia. The process involves T-cell mediated attack on the islets. Without insulin:
- Glycogenolysis and gluconeogenesis are unrestrained → hyperglycemia
- Lipolysis accelerates → free fatty acids → ketone bodies → diabetic ketoacidosis (DKA)
- Protein catabolism increases → wasting
Type 2 DM
Two central defects:
- Insulin resistance - peripheral tissues (muscle, liver, adipose) fail to respond normally to insulin
- Progressive beta-cell dysfunction - beta cells initially hypersecrete insulin to compensate, but eventually fail
Additional contributors include:
- Increased hepatic glucose production
- Impaired incretin effect (reduced GLP-1 response)
- Increased glucagon secretion from alpha cells
- Increased renal glucose reabsorption
- Lipotoxicity and glucotoxicity accelerating beta-cell apoptosis
Insulin Actions on Specific Tissues
Liver:
- Inactivates liver phosphorylase → prevents glycogen breakdown
- Increases glucokinase activity → traps glucose inside hepatocytes
- Activates glycogen synthase → promotes glycogen storage
- Inhibits gluconeogenesis
- Excess glucose converted to fatty acids → VLDL → fat storage
Muscle:
- Increases glucose uptake via GLUT4
- Promotes glycogen synthesis
- Promotes protein synthesis, inhibits protein catabolism
Adipose:
- Promotes fat storage; inhibits hormone-sensitive lipase (lipolysis)
Brain:
-
Little effect on glucose uptake (insulin-independent); however, insulin affects feeding behavior and energy metabolism
-
Guyton & Hall Textbook of Medical Physiology, p. 965-970
5. Diagnosis
Diagnostic Criteria (ADA - Nonpregnant Adults)
| Test | Diabetes | Prediabetes |
|---|---|---|
| Fasting plasma glucose (FPG) | ≥126 mg/dL (7.0 mmol/L) | 100-125 mg/dL (IFG) |
| 2-hr plasma glucose (75g OGTT) | ≥200 mg/dL (11.1 mmol/L) | 140-199 mg/dL (IGT) |
| HbA1c | ≥6.5% (48 mmol/mol) | 5.7-6.4% |
| Random plasma glucose | ≥200 mg/dL + symptoms | - |
- In an asymptomatic patient, two abnormal tests are required to confirm the diagnosis.
- A single test suffices in a symptomatic patient with classic hyperglycemia symptoms.
Key Investigations
- HbA1c - reflects mean glucose over ~3 months; used for both diagnosis and monitoring
- C-peptide - distinguishes residual beta-cell function; low/absent in T1DM
- Autoantibodies (GAD65, IA2, insulin) - confirm autoimmune T1DM
- Fasting lipid profile - dyslipidemia common in T2DM
- Urinary albumin-to-creatinine ratio (UACR) - screening for nephropathy
- eGFR - assess renal function
- Fundoscopy / dilated eye exam - screening for retinopathy
Glycemic Targets
- HbA1c goal: <7% for most patients; individualized based on patient age, comorbidities, hypoglycemia risk
- Fasting glucose: 80-130 mg/dL
- Post-prandial glucose (<2h): <180 mg/dL
6. Management
Goals of Therapy (Harrison's 2025)
- Eliminate symptoms related to hyperglycemia
- Reduce/eliminate long-term microvascular and macrovascular complications
- Allow the patient to achieve as normal a lifestyle as possible
6a. Lifestyle Modifications (All Types)
- Medical nutrition therapy (MNT): reduce refined carbohydrates, increase fiber, limit saturated fats
- Regular aerobic exercise (≥150 min/week of moderate-intensity)
- Weight loss in overweight/obese patients (even 5-10% weight loss significantly improves insulin sensitivity)
- Smoking cessation
- Self-monitoring of blood glucose (SMBG) or continuous glucose monitoring (CGM)
6b. Type 1 DM - Insulin Therapy
Insulin replacement must mimic physiologic insulin secretion: basal + prandial (bolus) coverage.
Insulin Preparations:
| Preparation | Onset | Peak | Duration |
|---|---|---|---|
| Rapid-acting (Aspart, Glulisine, Lispro) | <0.25 h | 0.5-1.5 h | 3-5 h |
| Short-acting (Regular) | 0.5-1.0 h | 2-3 h | 4-8 h |
| Inhaled human insulin | <0.25 h | 1-2 h | 3 h |
| Intermediate-acting (NPH) | 2-4 h | 4-10 h | 10-16 h |
| Long-acting (Glargine, Detemir) | 1-9 h | Flat/minimal | 20-24 h |
| Ultra-long-acting (Degludec) | 1-9 h | Flat | >42 h |
Delivery Systems:
- Multiple daily injections (MDI): most common
- Continuous subcutaneous insulin infusion (CSII/insulin pump)
- Sensor-augmented pump: integrates CGM; suspends infusion when glucose is low or predicted to drop
- Automated insulin delivery (AID/"closed-loop"): pump + CGM + algorithm adjusts basal rate in real time
6c. Type 2 DM - Pharmacotherapy
Step 1: Metformin (first-line, unless contraindicated)
- Mechanism: decreases hepatic glucose production (inhibits mitochondrial complex I), improves peripheral insulin sensitivity
- Benefits: weight-neutral or modest weight loss, low hypoglycemia risk, low cost, cardiovascular neutrality
- Contraindications: eGFR <30 mL/min (risk of lactic acidosis), iodinated contrast (hold temporarily)
Additional agents (based on comorbidities):
| Drug Class | Examples | Key Benefit | Key Risk |
|---|---|---|---|
| GLP-1 receptor agonists | Semaglutide, Liraglutide, Dulaglutide | CV & renal protection, weight loss | Nausea, pancreatitis risk |
| SGLT-2 inhibitors | Empagliflozin, Dapagliflozin, Canagliflozin | CV & renal protection, weight loss, heart failure benefit | UTI/genital infections, euglycemic DKA |
| DPP-4 inhibitors | Sitagliptin, Saxagliptin | Weight neutral, well tolerated | Moderate HbA1c lowering |
| Sulfonylureas | Glipizide, Glyburide, Glimepiride | Effective, inexpensive | Hypoglycemia, weight gain |
| Thiazolidinediones | Pioglitazone | Durable glucose control, NASH benefit | Weight gain, fluid retention, fracture risk, heart failure |
| Insulin | Various | Most potent glucose lowering | Hypoglycemia, weight gain |
| Alpha-glucosidase inhibitors | Acarbose | Post-prandial glucose | GI side effects |
2024 ACP Guideline update: Newer agents (GLP-1 RAs and SGLT-2i) are recommended for T2DM patients with established CVD or high CVD risk, CKD, or heart failure.
- Harrison's Principles of Internal Medicine 22E, p. 3248
7. Acute Complications
7a. Diabetic Ketoacidosis (DKA)
Primarily in T1DM (rarely T2DM, and as euglycemic DKA with SGLT-2 inhibitors).
Pathophysiology:
Relative/absolute insulin deficiency + counterregulatory hormone excess (glucagon, catecholamines, cortisol, GH):
- Glycogenolysis + gluconeogenesis → hyperglycemia
- Lipolysis → free fatty acids → beta-oxidation → ketone bodies (beta-hydroxybutyrate >> acetoacetate)
- Results in high anion-gap metabolic acidosis
Diagnostic Criteria:
- Serum glucose >250 mg/dL (>13.9 mmol/L)
- Ketonemia/ketonuria
- Metabolic acidosis: serum bicarbonate <15-18 mmol/L, pH 6.8-7.3, elevated anion gap
Clinical Features:
| Symptoms | Signs |
|---|---|
| Nausea/vomiting | Tachycardia |
| Thirst/polyuria | Hypotension |
| Abdominal pain | Kussmaul respirations |
| Weakness | Fruity breath (acetone) |
| Altered mental status | Dehydration |
Management:
- IV fluids (0.9% NaCl initially)
- Insulin infusion (regular insulin IV)
- Potassium replacement (hypokalemia risk as acidosis corrects)
- Bicarbonate only if pH <6.9
- Monitor glucose, electrolytes, anion gap
- Treat precipitating cause (infection is most common)
Note: Despite total-body K+ deficit, serum K+ at presentation may be normal/elevated due to acidosis driving K+ extracellularly. Must replace K+ before or with insulin to prevent life-threatening hypokalemia.
7b. Hyperglycemic Hyperosmolar State (HHS)
- Primarily in T2DM, older adults
- Extreme hyperglycemia (often >600 mg/dL), severe dehydration, hyperosmolality (>320 mOsm/kg)
- No significant ketoacidosis (enough residual insulin to suppress ketogenesis)
- Higher mortality than DKA
- Treatment: aggressive fluid replacement, insulin, electrolyte management
7c. Hypoglycemia
- Most common acute complication in treated diabetes
- Symptoms: sweating, tremor, palpitations (adrenergic); confusion, seizures (neuroglycopenic)
- Severe hypoglycemia threshold: glucose <54 mg/dL with symptoms
- Hypoglycemia unawareness: repeated hypoglycemia blunts counterregulatory epinephrine response; common with long-standing DM and autonomic neuropathy
- Treatment: 15-15 rule (15g fast-acting carbs, recheck in 15 min); glucagon kit for severe/unconscious patients
8. Chronic Complications
Diabetes-related complications affect many organ systems. Microvascular complications generally appear after the second decade of hyperglycemia; macrovascular complications (ASCVD) may precede clinical diagnosis.
8a. Microvascular Complications
Diabetic Retinopathy
- Leading cause of new blindness in adults in the USA
- Stages:
- Non-proliferative diabetic retinopathy (NPDR): microaneurysms, hard exudates, dot/blot hemorrhages, cotton-wool spots
- Proliferative diabetic retinopathy (PDR): neovascularization (new vessel formation) - high risk of vitreous hemorrhage and retinal detachment
- Diabetic macular edema (DME): most common cause of visual loss
- Prevention: tight glycemic control, blood pressure control
- Treatment: laser photocoagulation, anti-VEGF injections (bevacizumab, ranibizumab), vitrectomy
Diabetic Nephropathy
- Leading cause of end-stage renal disease (ESRD)
- Pathological hallmark: Kimmelstiel-Wilson nodules (glomerular nodular sclerosis)
- Stages: microalbuminuria (UACR 30-300 mg/g) → macroalbuminuria → declining GFR → ESRD
- Prevention/treatment: tight glycemic control, ACE inhibitors or ARBs (reduce proteinuria and progression), SGLT-2 inhibitors (have independent renoprotective effect), blood pressure control
- 2024 data: Semaglutide shown to reduce progression of CKD in T2DM patients (FLOW trial, NEJM 2024)
Diabetic Neuropathy
- Present in ~50% of individuals with long-standing T1DM or T2DM
- Risk factors: duration of DM, poor glycemic control, higher BMI, smoking, ASCVD, hypertriglyceridemia, hypertension
Forms:
- Distal symmetric polyneuropathy (DSPN) - most common; numbness, tingling, burning starting in feet, spreading proximally ("stocking-glove" distribution); worse at night; on exam: loss of protective sensation (10-g monofilament), reduced vibration sense, absent ankle reflexes
- Autonomic neuropathy: cardiovascular (resting tachycardia, orthostatic hypotension, QTc prolongation, sudden death risk), GI (gastroparesis, diabetic diarrhea), genitourinary (bladder dysfunction, erectile dysfunction), sudomotor (hyperhidrosis upper extremities, anhidrosis feet)
- Mononeuropathy: sudden-onset, single nerve involvement (CN III palsy with pupil sparing, carpal tunnel, femoral neuropathy)
- Polyradiculopathy: Diabetic amyotrophy - severe pain, weakness in thigh and hip muscles
Screening: annually, starting 5 years post-T1DM diagnosis; at time of T2DM diagnosis.
8b. Macrovascular Complications
- Coronary heart disease (CHD): most common cause of death; DM confers 2-4x increased risk
- Peripheral arterial disease (PAD): claudication, critical limb ischemia; major contributor to lower-extremity amputations
- Cerebrovascular disease: stroke risk 2-4x higher
- Heart failure: DM is an independent risk factor; diabetic cardiomyopathy occurs even without coronary disease
Key fact: Women with DM lose their cardioprotective female sex advantage - their CVD rates equal those of diabetic men, and women with DM have a sixfold greater risk of dying from CVD compared to non-diabetic women.
8c. Other Complications
| System | Complication |
|---|---|
| Gastrointestinal | Gastroparesis (delayed gastric emptying), diabetic diarrhea |
| Genitourinary | Neurogenic bladder, erectile dysfunction, recurrent UTIs |
| Dermatologic | Necrobiosis lipoidica, acanthosis nigricans, diabetic dermopathy, poor wound healing |
| Musculoskeletal | Charcot neuroarthropathy (Charcot joint), frozen shoulder, Dupuytren's contracture |
| Foot | Diabetic foot ulcers, osteomyelitis, gangrene, amputation |
| Infection | Increased susceptibility; malignant otitis externa, rhinocerebral mucormycosis, emphysematous pyelonephritis |
9. Diabetic Foot
- Results from neuropathy + peripheral vascular disease + infection
- Loss of protective sensation (from DSPN) leads to unrecognized trauma and ulceration
- Anhidrosis causes dry, cracked skin - portal of entry for infection
- Annual foot exams essential; patient education on foot care
- Offloading (total contact cast) for plantar ulcers
- Revascularization for ischemic ulcers
10. Monitoring & Targets
| Parameter | Target |
|---|---|
| HbA1c | <7% (individualized) |
| Fasting glucose | 80-130 mg/dL |
| Post-prandial glucose | <180 mg/dL |
| Blood pressure | <130/80 mmHg |
| LDL cholesterol | <70 mg/dL (high-risk) |
| Urine albumin/creatinine | <30 mg/g |
Monitoring tools:
- HbA1c: every 3 months if not at target; every 6 months if stable
- SMBG: finger-stick glucose monitoring
- CGM (Continuous Glucose Monitoring): real-time interstitial glucose; time-in-range (TIR) >70% is the current quality metric target
11. Special Populations
Gestational DM (GDM)
- Screening: all pregnant women at 24-28 weeks with 75g OGTT (or 1-hour 50g screen followed by 3-hour diagnostic test)
- Risks: macrosomia, shoulder dystocia, neonatal hypoglycemia, preeclampsia
- Treatment: diet/exercise first; if glucose targets not met, insulin (first-line pharmacotherapy in pregnancy); metformin and glyburide are alternatives but cross the placenta
Type 1 DM in Pregnancy (Pre-gestational)
- Risk of congenital malformations is 2-3x higher; strongly correlated with first-trimester glycemic control (HbA1c)
- Target HbA1c <6.5% pre-conception; <7% during pregnancy
12. Screening & Prevention
- T2DM screening: all adults ≥35 years; younger if overweight/obese + risk factors (family history, GDM history, hypertension, dyslipidemia, PCOS, high-risk ethnicity)
- Prevention of T2DM in prediabetes:
- Intensive lifestyle intervention (Diabetes Prevention Program): reduces T2DM incidence by ~58%
- Metformin: reduces incidence by ~31% (especially effective in <60 years, BMI ≥35, history of GDM)
- Weight loss is the single most effective intervention
Key Summary Table
| Feature | Type 1 DM | Type 2 DM |
|---|---|---|
| Pathogenesis | Autoimmune beta-cell destruction | Insulin resistance + beta-cell dysfunction |
| Age of onset | Usually <30 years | Usually >40 (but increasingly in youth) |
| Body habitus | Usually lean | Usually overweight/obese |
| Ketosis | Prone | Resistant (usually) |
| Insulin required | Always | Eventually |
| Autoantibodies | Present | Absent |
| C-peptide | Low/absent | Normal or elevated (early) |
| First-line Rx | Insulin | Metformin + lifestyle |
| Acute emergency | DKA | HHS |
References: Harrison's Principles of Internal Medicine 22E (2025), Chapter 416-417 | Guyton & Hall Textbook of Medical Physiology, Chapter 79 | Creasy & Resnik's Maternal-Fetal Medicine, Chapter 59 | Textbook of Family Medicine 9e, Chapter 20 | Tintinalli's Emergency Medicine, Chapter on DKA
This is a shared conversation. Sign in to Orris to start your own chat.