Biomechanics of knee joint
Reading File
Finding Sources
Finding Sources
Searching the Web
knee joint biomechanics anatomy stability mechanisms
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Biomechanics of the Knee Joint
The knee is the largest synovial joint in the body. It consists of two articulations - the tibiofemoral joint and the patellofemoral joint - and functions in 6 degrees of freedom (3 translational, 3 rotational), though its primary motion is in the sagittal plane.
1. Bony Geometry and Axes
The femur has distinct anatomical and mechanical axes because of the offset at the hip. In a normal tibia, these axes are identical. The medial and lateral femoral condyles differ in their radii of curvature - the medial condyle is larger than the lateral. This asymmetry has profound kinematic consequences.
Range of Motion (Miller's Review of Orthopaedics, 9th Ed.):
| Motion | Average Range | Functional Range |
|---|---|---|
| Flexion | 145° | 90° (117° to squat; 110° to rise from chair post-TKA) |
| Extension | -3° (hyperextension) | 0° |
| Internal rotation (at 90° flexion) | 30° | - |
| External rotation (at 90° flexion) | 45° | - |
2. Tibiofemoral Kinematics
Rolling and Sliding
Knee flexion/extension involves a combination of rolling and sliding of the femur on the tibia - not pure rotation. The instant center of rotation traces a J-shaped curve about the femoral condyle and moves posteriorly with increasing flexion.
Four-Bar Linkage Model
The interplay of the cruciate ligaments models the knee as a four-bar linkage system. As the knee flexes, the center of joint rotation (the intersection of the ACL and PCL) moves posteriorly, causing characteristic rolling-gliding at the articulating surfaces. All four major ligaments (ACL, PCL, MCL, LCL) must be intact for normal femoral rollback kinematics. - Miller's Review of Orthopaedics, 9th Ed.
Posterior Femoral Rollback
As the knee flexes, the tibiofemoral contact point moves posteriorly. This posterior rollback increases maximum knee flexion by preventing impingement of the posterior soft tissues. It is governed primarily by the PCL - normal rollback is compromised by PCL sacrifice (e.g., in cruciate-sacrificing TKA).
The "Screw-Home" Mechanism
During the last 15 degrees of extension, the femur internally rotates (or equivalently, the tibia externally rotates) to lock the knee into full extension. This is the "screw-home" mechanism. It occurs because:
- The medial femoral condyle has a larger radius of curvature than the lateral condyle
- The medial condyle continues to roll after the lateral condyle has finished
- The surrounding musculature (particularly the popliteus unlocks it on flexion)
- The ACL guides tibial rotation during this mechanism; the PCL acts as the axis of rotation
Bailey & Love's Short Practice of Surgery, 28th Ed. | Miller's Review of Orthopaedics, 9th Ed.
3. Patellofemoral Biomechanics
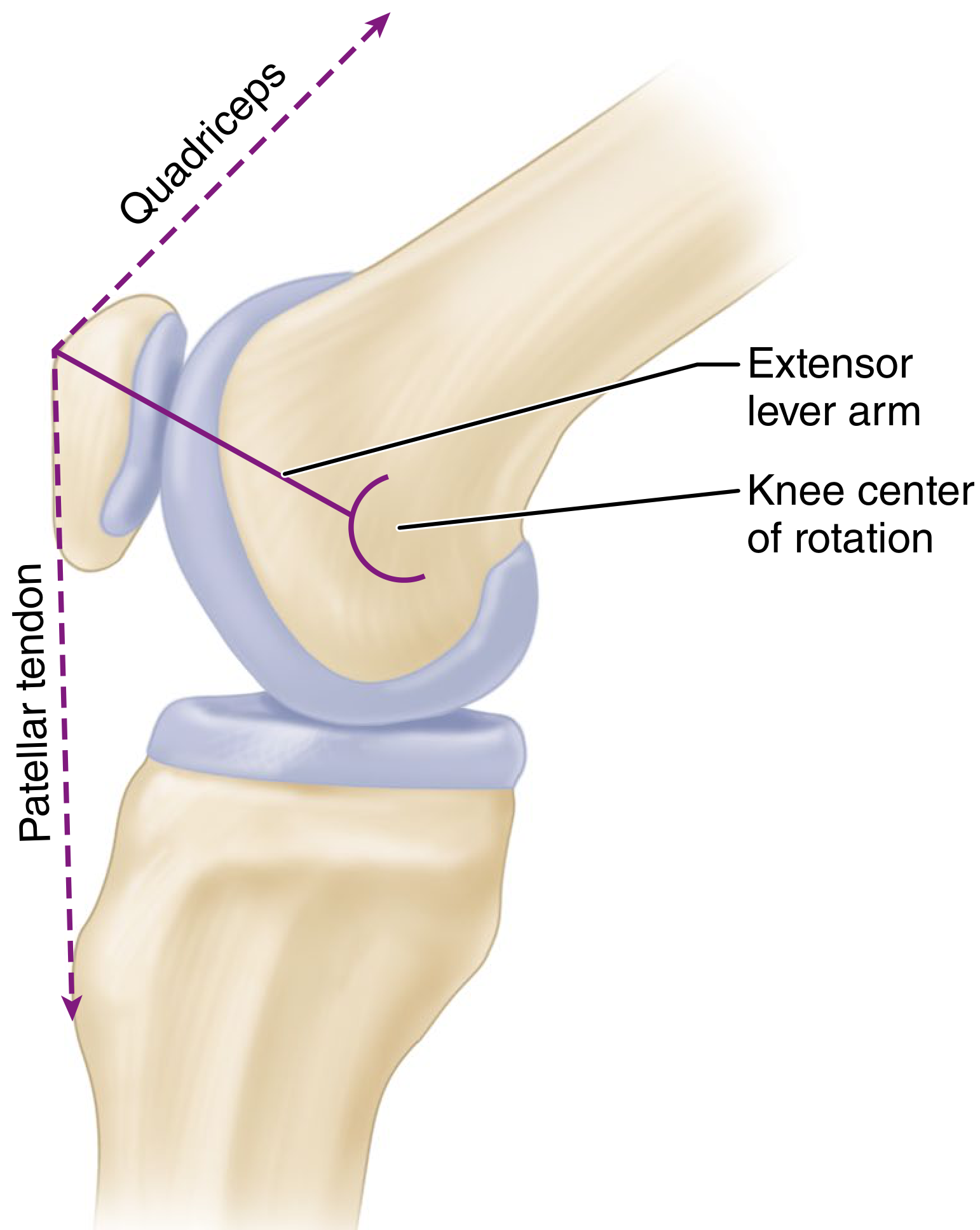
The patella displaces the quadriceps force vector anteriorly, lengthening the extensor lever arm. (Campbell's Operative Orthopaedics, 15th Ed.)
The patella functions as a pulley (sesamoid bone) for the extensor mechanism. Its thickness displaces the force vectors of the quadriceps and patellar tendons anteriorly, away from the center of rotation - this increases the extensor lever arm and improves the mechanical efficiency of quadriceps contraction.
Key patellofemoral facts:
- The extensor lever arm is greatest at 20-30° of flexion
- Quadriceps force required increases sharply in the last 20° of extension as less of the patella contacts the trochlear groove
- The patella slides 7 cm caudally with full knee flexion
- It bears loads up to 20x body weight during jumping
- It contains the thickest articular cartilage in the body
Q Angle
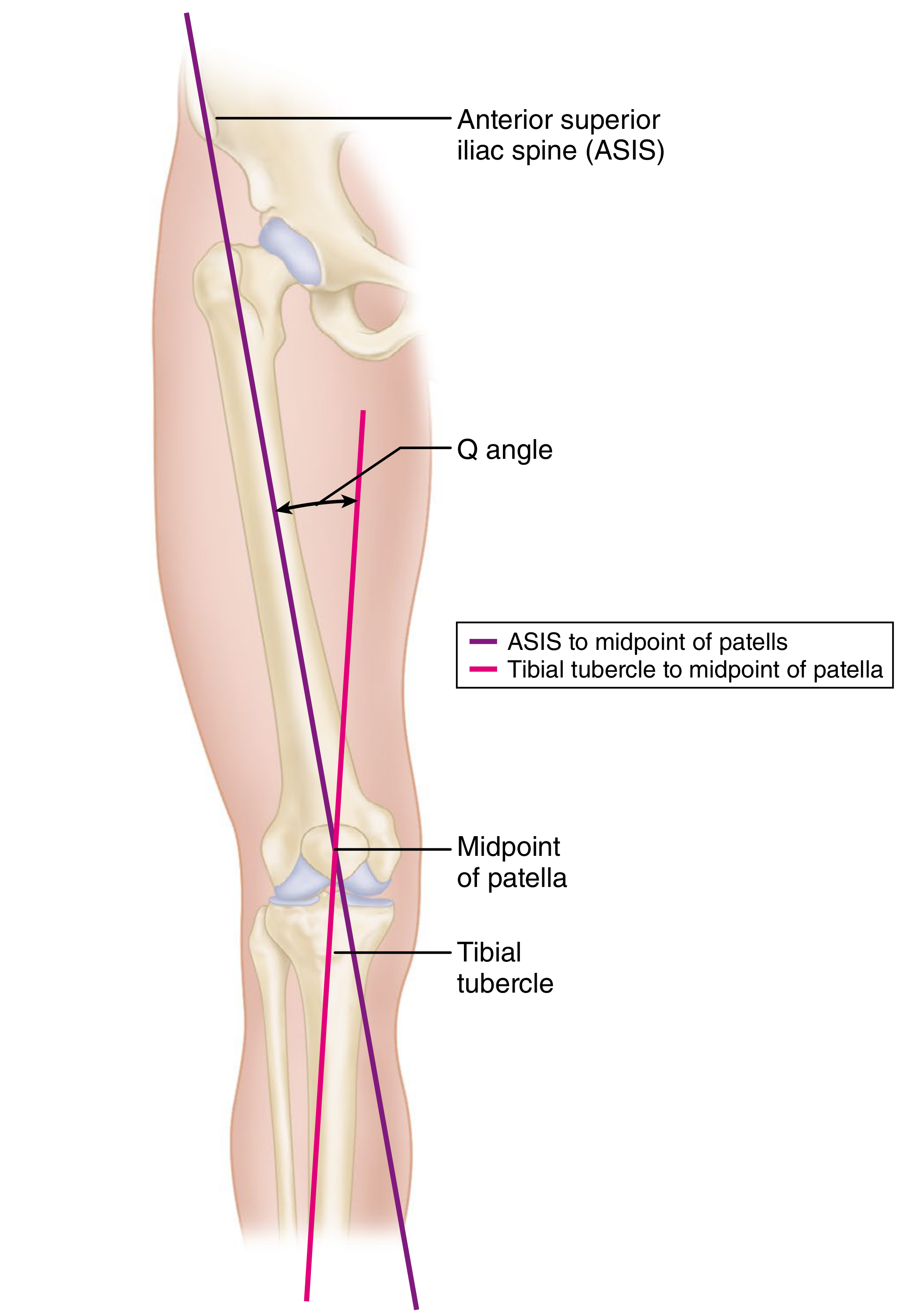
The Q angle is measured between the extended anatomic axis of the femur and the line from the center of the patella to the tibial tubercle. Larger Q angles create greater lateral patellar subluxation tendency. Lateral subluxation in early flexion is resisted primarily by the vastus medialis obliquus (VMO); as flexion increases, bony constraints of the trochlear groove become dominant. - Campbell's Operative Orthopaedics, 15th Ed.
4. Ligament Biomechanics
Ligaments are passive restraints against abnormal motion. Their tensile (failure) strengths (from Miller's Review of Orthopaedics, 9th Ed.):
| Ligament | Tensile Strength |
|---|---|
| ACL | ~2,200 N (up to 2,500 N in young individuals) |
| PCL | ~2,500-3,000 N |
| Superficial MCL (sMCL) | ~550 N |
| Deep MCL (dMCL) | ~100 N |
| Posterior oblique ligament (POL) | ~250 N |
| LCL | ~750 N |
For comparison, ACL graft strengths: 10-mm patellar tendon graft ~2,900 N; quadrupled hamstring graft up to ~4,000 N (though in-vivo strength diminishes).
ACL loads in daily activity: ~170 N during walking, up to ~500 N with running.
Directional Stability (Table from Miller's):
| Direction | Primary Stabilizers |
|---|---|
| Medial | Superficial MCL (primary), joint capsule, medial meniscus, ACL/PCL |
| Lateral | Joint capsule, IT band, popliteus |
| Anterior translation | ACL (primary) |
| Posterior translation | PCL (89% of resistance) |
| Rotation | ACL, PCL (axis of rotation for screw-home) |
Ligaments anterior to the flexion axis stretch with flexion; ligaments posterior to the axis shorten. Reconstructed ligaments must lie within the flexion axis to function isometrically through range of motion. - Miller's Review of Orthopaedics, 9th Ed.
5. Meniscal Biomechanics
The menisci serve multiple mechanical roles: load transmission, stress distribution, stability, lubrication, and deepening of the tibial plateau.
Load transmission (Miller's Review of Orthopaedics, 9th Ed.):
- Menisci transmit 50-75% of axial loads in full extension
- They transmit 85% of axial loads at 90° of knee flexion
- Medial meniscus bears 30-40% of tibiofemoral load
- Lateral meniscus bears ~70% of lateral compartment load
- Menisci reduce peak contact stresses by 100-200%
- Resection of 75% of radial meniscal width = equivalent contact stress increase to total meniscectomy
Stability role:
- The medial meniscus is a major secondary stabilizer against anterior tibial translation in an ACL-deficient knee (posterior horn of medial meniscus)
- ACL deficiency causes abnormal meniscal strain, especially in the posterior horn of the medial meniscus
- Lateral meniscus has twice the excursion of the medial meniscus during flexion (0.5 cm medial vs. 1.1 cm lateral during 120° of motion)
- Menisci move anteriorly in extension and posteriorly with flexion
Meniscal vascularity and biomechanical zones:
- Red-red zone (outer, vascular): highest healing potential
- Red-white zone (intermediate): less predictable healing
- White-white zone (inner, avascular): nutrition from synovial fluid only; poor healing
50% of the medial tibial plateau and 59% of the lateral tibial plateau are covered by meniscus.
6. Summary of Key Forces
| Activity | Joint Reaction Force |
|---|---|
| Walking | ~2-3x body weight |
| Climbing stairs | ~3-4x body weight |
| Running | ~5x body weight |
| Jumping (patellar) | Up to 20x body weight |
Clinical Correlates
- ACL injury - typically from non-contact twisting/landing; disrupts anterior tibial restraint and the screw-home guidance mechanism
- PCL injury - disrupts posterior restraint (89% contribution) and femoral rollback; posterior drawer sign positive
- Meniscectomy - dramatically increases contact stresses, predisposing to early osteoarthritis
- Patellar dislocation - results from abnormal Q angle, VMO weakness, or trochlear dysplasia
- Collateral ligament stress testing - opening at 30° = isolated collateral injury; opening in full extension = combined cruciate + collateral injury
Sources: Bailey & Love's Short Practice of Surgery 28th Ed. | Miller's Review of Orthopaedics 9th Ed. | Campbell's Operative Orthopaedics 15th Ed. (2026)
This is a shared conversation. Sign in to Orris to start your own chat.