Distraction osteogenesis what's this principle uses and application of it and everything related to it for 10 marks question with appropriate illustrative images and diagrams
Reading File
Finding Sources
Finding Sources
Searching Images
distraction osteogenesis bone regeneration Ilizarov technique
Reading File
Reading File
Searching Images
distraction osteogenesis phases latency distraction consolidation diagram
Reading File
Finding Sources
Searching Images
Ilizarov external fixator circular frame limb lengthening corticotomy
Reading File
Reading File
Searching Images
mandibular distraction osteogenesis craniofacial jaw lengthening device
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
Loading Image
Loading Image
I now have comprehensive information from multiple textbooks and excellent images. Let me compile the complete 10-mark answer:
Distraction Osteogenesis — Comprehensive 10-Mark Answer
1. Definition & Historical Background
Distraction osteogenesis (DO) is the mechanical induction of new bone formation by the gradual, controlled separation of two viable bone segments after a low-energy osteotomy (corticotomy). The mechanical tension placed across the healing gap stimulates biologic processes — bone, cartilage, vasculature, nerve, and soft tissue all regenerate simultaneously — a phenomenon Ilizarov termed the "tension-stress effect."
- First described by Alessandro Codivilla (1905) for femoral lengthening
- Systematically developed by Gavriil Ilizarov (USSR, 1950s–1970s) using circular external fixators and corticotomy
- Applied to the craniofacial skeleton in the 1990s; now widespread in orthopaedics, maxillofacial surgery, and reconstructive surgery
Rockwood and Green's Fractures in Adults, 10th ed. 2025
2. Principle — The Tension-Stress Effect
Under controlled, gradual mechanical tension:
- Fibroblast-like cells in the central fibrous zone (interzone) become elongated and orient along the distraction vector
- Surrounding collagen fibers align parallel to the tension vector
- Fibroblastic cells differentiate into osteoblasts, depositing osteoid on collagen bundles
- Osteoblasts further differentiate into osteocytes within the HA matrix
- New bone columns grow bidirectionally from the interzone — both proximally and distally — eventually bridging the gap
Key features of the process:
- Ossification is primarily intramembranous (bypassing the cartilaginous phase) under stable fixation
- Under instability, endochondral ossification occurs; under extreme instability, pseudarthrosis forms
- Intense neovascularization occurs in parallel — capillaries proliferate along the distraction vector, forming a dense longitudinal vascular network
Rockwood and Green's Fractures in Adults, 10th ed. 2025; Miller's Review of Orthopaedics, 9th ed.
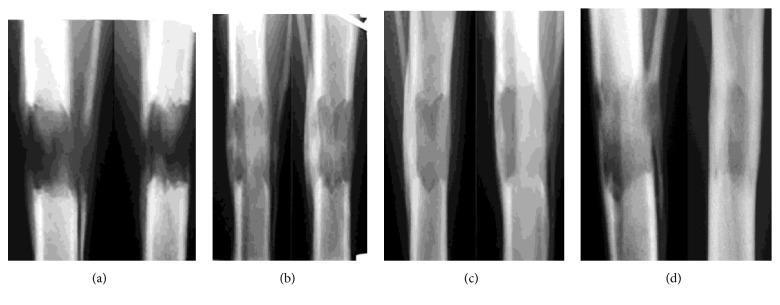
3. Three Phases of Distraction Osteogenesis
The process follows three well-defined phases:
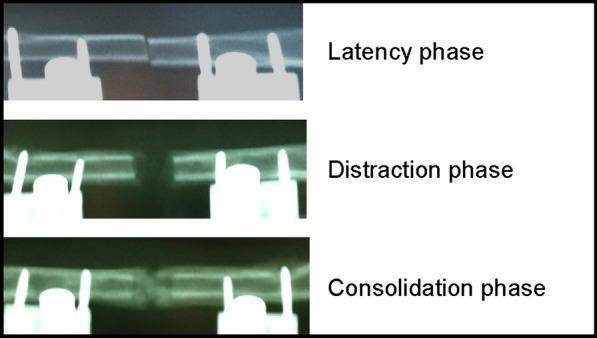
Phase 1 — Latency Phase (5–7 days)
- Occurs between corticotomy and initiation of distraction
- Soft callus formation begins; granulation tissue organises
- Hematoma organises; early vascular ingrowth commences
- Periosteum and marrow blood supply regenerate
- Critical: distraction must not begin too early (disrupts callus) or too late (premature consolidation, especially in children)
Phase 2 — Distraction Phase (~1 mm/day)
- Active mechanical separation of bone segments
- Fibrous interzone maintained at the centre
- Longitudinal columns of new bone form from each surface toward the interzone
- Bone forms by direct intramembranous ossification
- Intense neovascularization parallels osteogenesis
- Rate: 1 mm/day divided into 4 increments of 0.25 mm (rhythm)
- < 0.5 mm/day → premature consolidation
-
2 mm/day → vascular disruption, cyst formation, regenerate failure
- Soft tissues (muscle, nerve, skin) adapt simultaneously
Phase 3 — Consolidation Phase (typically 2× the distraction phase)
- Distraction ceases; frame remains in place
- Fibrous interzone mineralises and matures into cortical bone
- Progressive corticalization from periphery inward
- Trabecular bone converts to lamellar bone
- Frame removed only when full cortical continuity on radiograph confirmed
4. Histology of the Distraction Zone
The regenerate zone has a characteristic physis-like microarchitecture:
| Zone (from centre outward) | Characteristics |
|---|---|
| Fibrous interzone | Fibroblast-like cells; central growth region |
| Transition zone | Collagen bundles aligning along distraction vector |
| Osteogenic zone | Osteoblasts lining collagen; osteoid deposition |
| Remodeling zone | Woven bone → lamellar bone; large vascular channels |
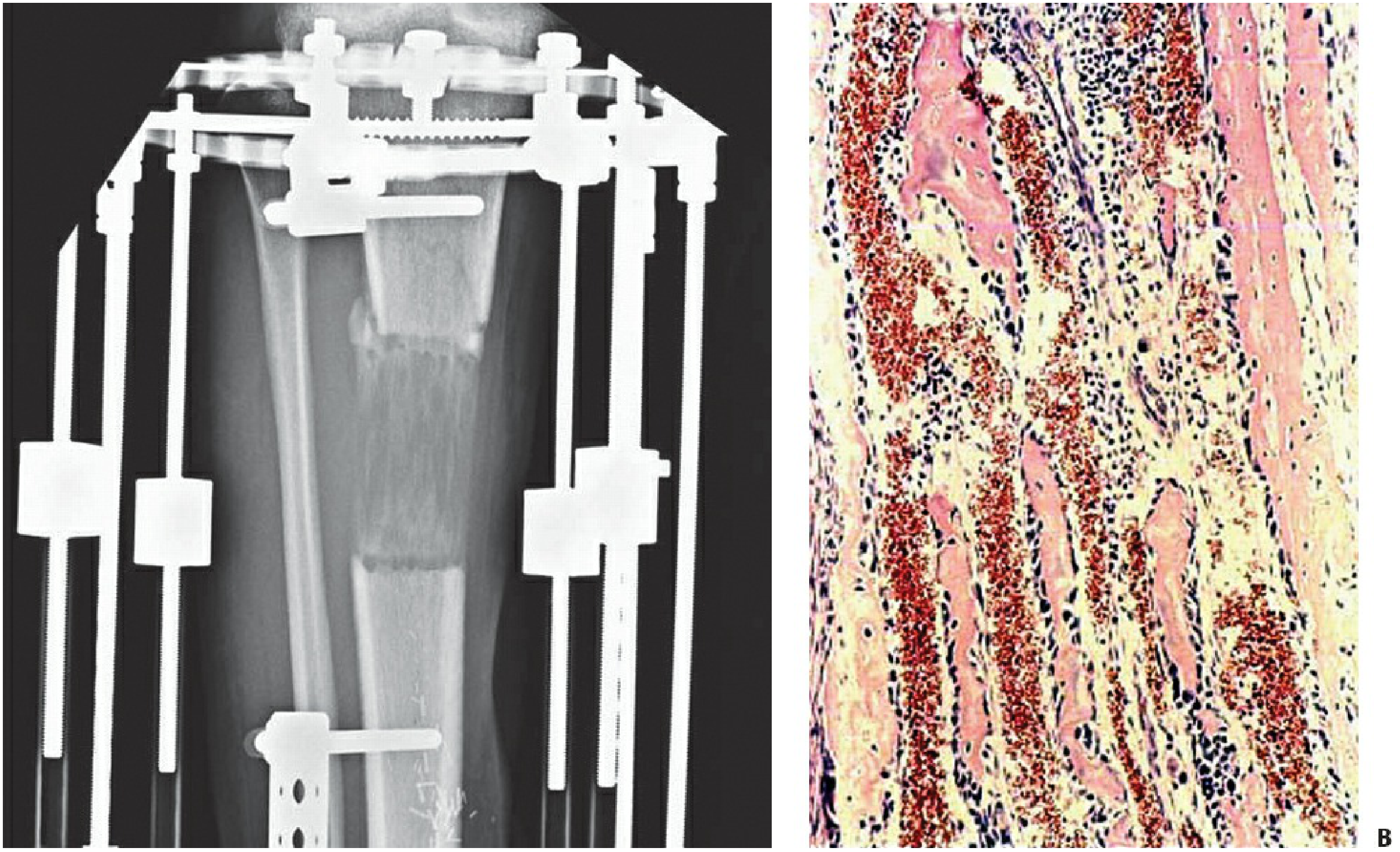
Rockwood and Green's Fractures in Adults, 10th ed. — The interzone is the "dark z area mid-regenerate." Collagen fibrils align along the vector of distraction; osteoblasts line collagen bundles; large vascular channels surround each bundle.
5. Technique — Corticotomy
A low-energy corticotomy (not an osteotomy) is fundamental to successful DO:
- Anterior, antero-lateral, and antero-medial cortices are scored with a narrow osteotome
- Posterior cortex is fractured by closed osteoclasis to preserve the periosteum and endosteum
- The medullary canal and periosteum are kept intact → maximises blood supply to the regenerate
- Incision is minimal to protect surrounding soft tissue vascularity
Rockwood and Green's Fractures in Adults, 10th ed. — "Superior bone regeneration is formed when a very low-energy osteoclasis technique is utilized"
6. Optimal Conditions (Summary Table)
| Parameter | Optimal Value |
|---|---|
| Latency period | 5–7 days |
| Rate of distraction | 1 mm/day |
| Rhythm | 0.25 mm × 4 times/day |
| Fixation stability | Rigid; eliminate shear/torsion/bending |
| Corticotomy | Low-energy; periosteum preserved |
| Soft tissue stripping | Minimal |
| Weight bearing | Encouraged (physiologic loading) |
Miller's Review of Orthopaedics, 9th ed.
7. Devices Used
Circular External Fixator (Ilizarov Frame)
- Multiple stainless steel rings connected by threaded rods
- Trans-osseous wires and half-pins anchor to bone
- Provides multi-planar stability; limits shear and torsional forces
- Adjustable for deformity correction in any plane

Hexapod (Taylor Spatial Frame)
- Six adjustable oblique struts on Ilizarov-style rings
- Computer-software-guided correction in 6 axes simultaneously (coronal/sagittal angulation and translation, rotation, length)
- Ideal for complex multi-planar deformities
Monolateral Fixators
- Simpler; used for straightforward lengthening
Internal Lengthening Nails (Modern)
- Motorized intramedullary nails (e.g., PRECICE nail)
- Eliminate external fixator entirely; patient-driven using an external magnetic remote controller
- Preferred for cosmesis and comfort in modern limb lengthening
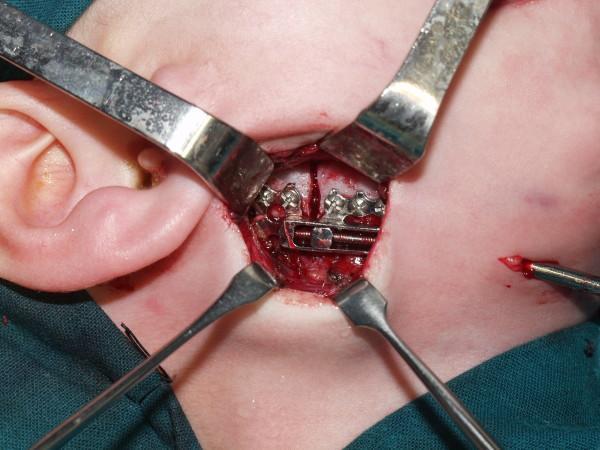
Internal Distraction Devices (Craniofacial)
- Miniaturized tooth-borne or bone-anchored distraction screws for jaw/skull
8. Applications
A. Orthopaedic
| Indication | Details |
|---|---|
| Limb length discrepancy | Most common; > 2 cm usually treated with DO |
| Deformity correction | Angular and rotational deformities via differential lengthening |
| Bone transport | Bifocal or trifocal transport to fill critical-size bone defects (tumour resection, trauma, infection) |
| Non-union / infected non-union | Debridement + acute shortening + re-lengthening |
| Congenital anomalies | Achondroplasia, fibular hemimelia, congenital pseudarthrosis of tibia |
| Osteomyelitis with bone loss | Ilizarov bone transport after saucerisation |
Bone transport uses a corticotomy proximal (or distal) to the defect; the transport segment is gradually distracted through the defect until it contacts the opposite end ("docking site"), where compression is applied to achieve union — bifocal technique.
B. Craniofacial and Maxillofacial Surgery
Distraction osteogenesis was first applied to the craniofacial skeleton more than 80 years ago but came into widespread use only in the past 25 years. Key applications:
| Application | Indication |
|---|---|
| Mandibular DO | Micrognathia, Pierre Robin sequence, hemifacial microsomia, TMJ ankylosis |
| Midface (Le Fort III / monobloc) DO | Syndromic craniosynostosis (Crouzon, Apert) — midface hypoplasia |
| Posterior cranial vault distraction (PCVD) | Multi-suture craniosynostosis; achieves 20–40 mm advancement vs 10–15 mm with conventional FOA |
| Maxillary DO | Cleft palate, sleep apnea (DOME procedure) |
| Alveolar DO | Dental implant site augmentation |

Advantages of craniofacial DO over conventional osteotomies:
- Gradual stretching of the soft tissue envelope → reduced tension → fewer wound complications
- Less blood loss; no need for bone grafts
- Larger advancements possible (especially PCVD)
- Safer in infants with syndromic craniosynostosis (avoids early major blood loss)
Cummings Otolaryngology Head & Neck Surgery; Bailey and Love's Surgery, 28th ed.
9. Advantages of Distraction Osteogenesis
- Creates new bone without grafts — the patient is their own bone bank
- Simultaneously stretches all surrounding soft tissues (muscle, nerve, skin, vessels)
- Allows corrections in three dimensions gradually
- Reduced blood loss and operative time compared to traditional osteotomies
- Weight-bearing encouraged — physiologic loading improves regenerate quality
- Applicable to children (bone formation is rapid in younger patients)
10. Complications
| Complication | Details |
|---|---|
| Pin-track infection | Most common (10–100%); graded I–IV; managed with pin care, antibiotics, or pin removal |
| Premature consolidation | Too-long latency; especially in children; managed by slow continued distraction or repeat corticotomy |
| Delayed consolidation / regenerate failure | Rapid distraction rate, periosteal stripping, frame instability |
| Axial deviation | Unequal soft tissue tension; needs frame adjustment |
| Neurovascular injury | 2–13%; especially with rapid distraction or poor vector |
| Fracture | Refracture through regenerate or pin sites (4–5%); premature frame removal |
| Joint stiffness / contracture | From prolonged fixation; prevented by physiotherapy |
| Psychological burden | Prolonged treatment (months); patient/family compliance essential |
| Docking site non-union | After bone transport; may require bone grafting or BMP |
Rockwood and Green's Fractures in Adults, 10th ed. 2025
11. Summary Mind-Map
DISTRACTION OSTEOGENESIS
├── PRINCIPLE: Tension-Stress Effect (Ilizarov)
│ ├── Controlled corticotomy → gradual separation
│ └── Intramembranous ossification in distraction gap
│
├── PHASES
│ ├── Latency (5–7 days) — callus organises
│ ├── Distraction (1 mm/day × 4) — bone columns form
│ └── Consolidation (2× distraction phase) — mineralisation
│
├── DEVICES
│ ├── Ilizarov circular frame
│ ├── Hexapod (Taylor Spatial Frame)
│ ├── Monolateral fixator
│ ├── Internal lengthening nail (PRECICE)
│ └── Internal craniofacial distractors
│
├── APPLICATIONS
│ ├── Orthopaedic: LLD, deformity, bone transport, non-union
│ └── Craniofacial: mandible, midface, cranial vault, alveolus
│
└── COMPLICATIONS
├── Pin-track infection (most common)
├── Premature / delayed consolidation
├── Axial deviation, refracture
└── Neurovascular injury
Key references:
- Rockwood and Green's Fractures in Adults, 10th ed. 2025 — Biology of Distraction Osteogenesis, pp. 430–454
- Miller's Review of Orthopaedics, 9th ed. — Distraction Osteogenesis, p. 36
- Cummings Otolaryngology Head and Neck Surgery — Distraction Osteogenesis, p. 3587
- Bailey and Love's Short Practice of Surgery, 28th ed.
This is a shared conversation. Sign in to Orris to start your own chat.