Panophthalmitis case presentation for residency notes and viva questions and answers in detail ophthalmology
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
I now have comprehensive material from the textbooks. Let me compile the detailed residency notes and viva Q&A.
Panophthalmitis - Residency Notes & Viva Questions
PART 1: CASE PRESENTATION
Presenting Complaint
A 45-year-old male farmer presents with severe pain in the right eye, rapidly progressive loss of vision, redness, and swelling of the eyelids for 3 days, following an injury with a wooden stick while working in the field 5 days ago.
History of Present Illness
- H/o penetrating ocular injury with organic (wooden) material 5 days ago
- Primary wound closure done at a peripheral centre 4 days back
- Progressive worsening pain since day 2 post-injury, now severe and throbbing
- Vision: Was finger counting at 2 metres at primary centre, now only perceives light
- Swelling of both eyelids, discharge (purulent), marked redness
- Low-grade fever, malaise
- No similar history in the other eye
- No h/o diabetes, immunosuppression, or prior eye surgery
Past History
- No systemic illness
- No prior ocular surgery or trauma
- No drug allergies
Examination
General: Febrile (38.4°C), pulse 96/min, BP 122/78 mmHg
Ocular Examination - Right Eye:
| Parameter | Findings |
|---|---|
| Vision | Perception of light only (PL+) |
| IOP | Not recordable (eye too tender/soft) |
| Lids | Marked oedema, erythema, ptosis of both lids |
| Conjunctiva | Severe chemosis, 360° conjunctival injection, purulent discharge |
| Cornea | Diffuse oedema, ring abscess, stromal infiltrate |
| Anterior chamber | Hypopyon (4 mm), dense fibrinous exudate, flare 4+ |
| Iris | Congested, muddy, poorly visible |
| Lens | Hazy view |
| Vitreous | B-scan: dense vitreous opacity/abscess |
| Fundus | Not visible |
| Extraocular motility | Restricted in all directions of gaze |
| Proptosis | Present (3 mm) |
Left Eye: Normal examination
Investigations
- B-scan ultrasonography right eye: Dense vitreous echoes, choroidal thickening, posterior scleritis pattern
- CT orbit: Orbital cellulitis with extension; proptosis right eye
- Blood cultures x2 (sent before antibiotics)
- CBC: TLC 14,200 (neutrophilia), ESR elevated
- Blood sugar (rule out DM)
- Vitreous/AC tap: Gram stain, culture, and sensitivity (if surgical intervention planned)
Diagnosis
Right eye Panophthalmitis - Post-traumatic (exogenous), following penetrating injury with organic matter
PART 2: DISEASE OVERVIEW FOR RESIDENCY NOTES
Definition
Panophthalmitis is suppurative inflammation of all coats of the eyeball (retina, choroid/uvea, and sclera) extending into the orbital tissues. It represents the most severe form of intraocular infection.
- Endophthalmitis = inflammation confined to the interior of the eye (vitreous ± uveal tract), not extending beyond sclera
- Panophthalmitis = endophthalmitis + involvement of uvea and sclera + orbital extension
"Endophthalmitis is a term used to describe inflammation of the interior of the eye involving the vitreous humor, and panophthalmitis is the term used to describe inflammation of the interior of the eye that extends into the uvea and sclera."
- Robbins, Cotran & Kumar Pathologic Basis of Disease
Classification
A. By Source of Infection
| Type | Route | Example |
|---|---|---|
| Exogenous | Direct inoculation from environment | Penetrating trauma, post-surgery (cataract, vitrectomy, trabeculectomy), corneal ulcer perforation |
| Endogenous | Haematogenous seeding | Bacterial sepsis, Klebsiella liver abscess, fungemia (IV drug use, candidemia), pulmonary infections |
B. By Onset (Post-surgical)
- Acute - within days of surgery (most common; S. epidermidis)
- Subacute/Delayed - weeks to months post-surgery (Cutibacterium acnes, fungi)
- Bleb-related - complicating filtering surgery
Aetiology and Causative Organisms
Post-cataract extraction:
- Most common: Staphylococcus epidermidis
- Common: S. aureus, Streptococcal species
- Less common: Gram-negative bacilli (Pseudomonas, Klebsiella, Bacillus, E. coli, Proteus, Haemophilus influenzae)
- Anaerobes
Post-traumatic (penetrating injury with IOFB):
- Staphylococcus spp. and Bacillus spp. - ~90% of culture-positive cases
- Bacillus cereus - especially in agricultural injuries; notoriously virulent and rapidly destructive
Bleb-associated:
- Streptococcus spp. and Gram-negative infections (more virulent than post-cataract)
Endogenous:
- Gram-positives: S. aureus, Streptococci
- Gram-negatives: Klebsiella pneumoniae (especially in Asians with liver abscess), E. coli, Pseudomonas
- Fungi: Candida albicans (IV drug users, post-surgical), Aspergillus
Subacute:
- Cutibacterium acnes (formerly Propionibacterium acnes) - requires anaerobic culture held for 14 days; classic white capsular plaque
Robbins Pathology notes that Candida may disseminate hematogenously to the retina, especially in IV drug users or systemic candidemia, producing multiple retinal abscesses
Pathogenesis
Penetrating trauma / Post-surgical wound / Haematogenous seeding
↓
Entry of organisms into vitreous cavity
↓
Suppurative vitritis (Endophthalmitis)
↓
Extension through choroid and sclera
↓
Panophthalmitis (orbital involvement, proptosis, restricted EOM)
- The retina is extremely sensitive to suppurative inflammation - irreversible injury can occur within a few hours
- Viable bacteria in the vitreous have few host defences (avascular, poor neutrophil access)
Clinical Features
Symptoms
- Severe, throbbing ocular pain
- Rapid loss of vision (may progress to no light perception)
- Redness, swelling of eyelids
- Purulent discharge
- Photophobia, lacrimation
- Systemic: fever, malaise (especially endogenous)
Signs - Anterior Segment
- Lid oedema, erythema
- Conjunctival chemosis, 360° injection
- Purulent discharge
- Corneal oedema, infiltrate, ring abscess (in severe cases)
- Hypopyon (pathognomonic of suppurative intraocular infection)
- Fibrin/exudate in anterior chamber, 4+ cells and flare
- Muddy, congested iris
- Absent red reflex
Signs - Posterior Segment
- Vitreous haze, vitritis
- Vitreous abscess
- Retinal infiltrates, flame haemorrhages ± white centres
- Retinal/subretinal/choroidal abscesses
- Retinal detachment (late)
Signs of Panophthalmitis Specifically (Orbital Extension)
- Proptosis
- Restricted extraocular movements (all directions)
- Chemosis extending to the forniceal region
- Eyelid cellulitis
- Orbital pain on movement
(Wills Eye Manual: "Panophthalmitis with orbital involvement (proptosis, restricted ocular motility)")
Investigations
-
B-scan ultrasonography (mandatory if posterior pole not visible)
- Dense vitreous echoes (vitritis/abscess)
- Choroidal thickening
- Retinal detachment
- Scleral/orbital involvement
-
CT orbit - rule out orbital cellulitis extension, retained foreign body, intracranial extension
-
Intraocular fluid sampling for culture:
- Vitreous aspirate (preferred - higher yield)
- Aqueous paracentesis
- Stains: Gram stain, Giemsa stain, Methenamine-silver (fungi)
- Cultures: Blood agar, Chocolate agar, Sabouraud agar (fungi), Thioglycolate broth (anaerobes)
- Critical: For C. acnes - anaerobic culture must be held for 14 days
-
Blood cultures x2 (before antibiotics, especially in endogenous cases)
-
CBC, ESR, CRP, blood sugar, LFT, RFT, HIV, immunosuppression workup
-
Removed IOFB should be sent for culture
Treatment
1. Medical Management
Intravitreal antibiotics (first-line, most important):
- Vancomycin 1 mg/0.1 mL (Gram-positive coverage)
- Ceftazidime 2.25 mg/0.1 mL (Gram-negative coverage)
- Alternative if penicillin allergic: Amikacin instead of ceftazidime
- Intravitreal dexamethasone 0.4 mg/0.1 mL - considered in severe vitreous inflammation (after cultures obtained)
Topical antibiotics (fortified):
- Vancomycin + Tobramycin, q1h around the clock for 24-48 hours
- Especially important for bleb-related cases, wound leaks
Topical steroids:
- Prednisolone acetate 1% q1h (after 48 hours)
Cycloplegic:
- Atropine 1% b.i.d. to t.i.d.
Systemic antibiotics:
- IV/oral fluoroquinolones (moxifloxacin) - especially for bleb-related, traumatic, or endogenous endophthalmitis
- Systemic antibiotics not routinely indicated for post-cataract endophthalmitis (poor intraocular penetration)
- For fungal: Intravitreal amphotericin B 5-10 μg/0.1 mL or voriconazole 100 μg/0.1 mL + systemic antifungals
2. Surgical Management
Pars Plana Vitrectomy (PPV):
- Indication: Vision of light perception or worse at presentation (post-cataract extraction - per Endophthalmitis Vitrectomy Study)
- PPV removes the microbial load, inflammatory debris, and allows direct sampling
- May also be beneficial in bleb-related, traumatic, or endogenous cases
Evisceration:
- Removal of ocular contents while preserving the scleral shell
- Indicated when the eye is unsalvageable and infection is limited to the globe
- Preferred over enucleation in active infection (less risk of spreading meningitis)
Enucleation:
- Removal of the entire globe
- Indicated in cases where orbital extension cannot be controlled, painful blind eye, or sympathetic ophthalmia risk
In panophthalmitis with orbital extension, evisceration/enucleation may be necessary to control life-threatening orbital sepsis.
3. Prevention
- 5% povidone-iodine conjunctival preparation before intraocular surgery (evidence-based)
- Intracameral antibiotics at time of cataract surgery (reduces risk)
- Prophylactic intravitreal antibiotics for high-risk penetrating trauma (agricultural injuries)
- Prompt removal of IOFB
Prognosis
- Post-traumatic panophthalmitis (especially with Bacillus cereus or Streptococcus) - very poor visual prognosis; often requires evisceration
- Bleb-related endophthalmitis - worse prognosis than post-cataract (more virulent organisms)
- Endogenous - poor if bilateral or Bacillus/Klebsiella; better with early systemic treatment
- Post-cataract - relatively better if treated promptly (S. epidermidis)
PART 3: PATHOLOGY IMAGE
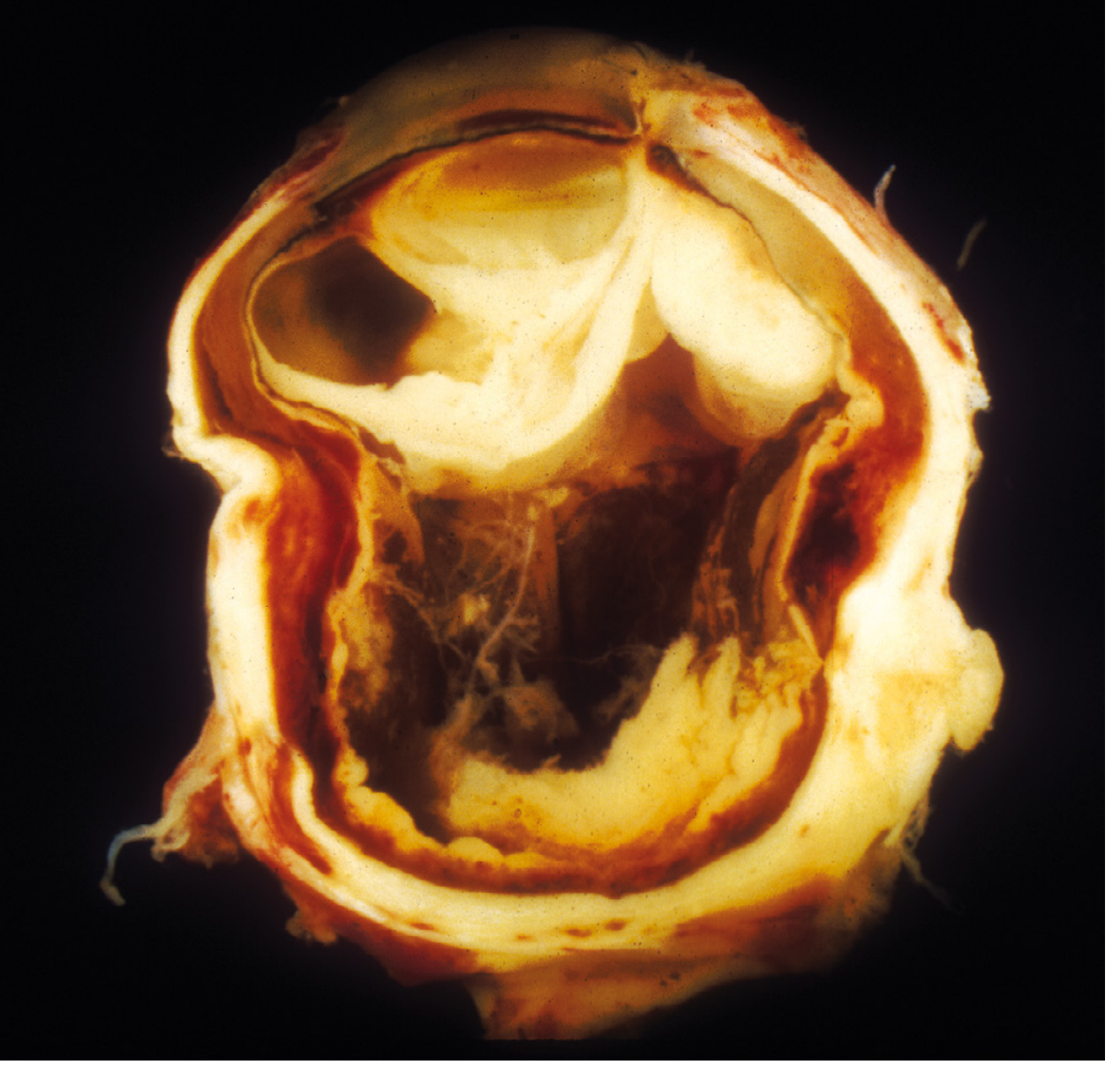
Exogenous panophthalmitis from Robbins Pathology (Fig. 29.16) - this eye was removed after a foreign body injury. Note the complete architectural distortion of the globe from suppurative inflammation extending through all coats:
PART 4: VIVA QUESTIONS AND ANSWERS
Q1. Define panophthalmitis and distinguish it from endophthalmitis.
A: Endophthalmitis is suppurative inflammation of the interior of the eye (vitreous and uveal tract). Panophthalmitis is inflammation that extends beyond this, involving the uvea, sclera, and into the orbit. Clinically, panophthalmitis presents with features of endophthalmitis PLUS orbital signs: proptosis, restricted extraocular movements, and orbital cellulitis. The distinction is clinically important because panophthalmitis carries a worse prognosis and often requires more aggressive surgical intervention.
Q2. What is the most common causative organism in post-cataract endophthalmitis?
A: Staphylococcus epidermidis is the most common. It is a coagulase-negative Staphylococcus (CONS) from the normal lid/conjunctival flora that gains entry during surgery. S. aureus and Streptococcal species are next most common. Gram-negative organisms (Pseudomonas, Klebsiella) are less common but have worse prognosis.
Q3. Which organism causes the most devastating post-traumatic endophthalmitis and why?
A: Bacillus cereus. It is a Gram-positive, spore-forming rod found in soil and organic matter. It secretes multiple toxins including phospholipases and proteases that cause rapid, fulminant intraocular destruction. Agricultural injuries (e.g., vegetable matter, soil contamination) carry the highest risk. Vision loss can occur within 12-24 hours. The organism is resistant to beta-lactams and is treated with vancomycin + clindamycin.
Q4. What is the Endophthalmitis Vitrectomy Study (EVS) and what were its key conclusions?
A: The EVS was a landmark randomised controlled trial in post-cataract extraction endophthalmitis. Key conclusions:
- Immediate PPV was beneficial only when vision was light perception or worse at presentation
- When vision was hand motions or better, tap and inject (without PPV) had comparable outcomes
- Systemic antibiotics (IV amikacin + vancomycin) added NO benefit over intravitreal antibiotics alone
- Intravitreal vancomycin + amikacin/ceftazidime were the standard treatment
- Note: The EVS was specific to post-cataract extraction endophthalmitis. PPV may be beneficial in other settings (bleb-related, post-traumatic) independent of vision level.
Q5. What are the critical signs distinguishing panophthalmitis from orbital cellulitis?
A: Both can present with proptosis, lid oedema, restricted EOM, and fever. The key distinguishing features:
| Feature | Panophthalmitis | Orbital Cellulitis |
|---|---|---|
| Hypopyon | Present | Absent |
| Vitreous cells/abscess | Present (B-scan) | Absent |
| Red reflex | Absent | Present |
| Antecedent ocular trauma/surgery | Often present | Often sinusitis/dacryocystitis |
| Intraocular pressure | Variable/low | Normal/elevated |
| Primary site | Inside globe | Outside globe (orbital fat) |
In fact, panophthalmitis can cause secondary orbital cellulitis, and orbital cellulitis can cause secondary panophthalmitis (by direct extension).
Q6. What intravitreal antibiotics are used and what are their doses?
A:
- Vancomycin: 1 mg/0.1 mL (covers Gram-positives including MRSA)
- Ceftazidime: 2-2.25 mg/0.1 mL (covers Gram-negatives including Pseudomonas)
- If penicillin-allergic: Amikacin 0.4 mg/0.1 mL instead of ceftazidime
- Fungal: Amphotericin B 5-10 μg/0.1 mL or Voriconazole 100 μg/0.1 mL
- Intravitreal dexamethasone: 0.4 mg/0.1 mL (adjunctive, in select severe cases)
- Bleb-related: Vancomycin 2 mg/0.1 mL + Ceftazidime 2 mg/0.1 mL
Q7. What is TASS and how do you differentiate it from infectious endophthalmitis?
A: Toxic Anterior Segment Syndrome (TASS) is sterile inflammation from a non-infectious agent introduced during surgery (e.g., incorrect irrigating solution pH/concentration, preservatives, improperly cleaned instruments).
| Feature | TASS | Infectious Endophthalmitis |
|---|---|---|
| Onset | 6-24 hours post-op | Usually 2-7 days post-op |
| Pain | Usually minimal | Severe |
| Vitreous involvement | Absent/minimal | Present (vitritis) |
| Corneal oedema | Diffuse, severe | Variable |
| Response to steroids | Rapid | Minimal/none |
| Systemic features | Absent | May be present |
| Cultures | Negative | Positive |
Q8. What is Cutibacterium acnes endophthalmitis?
A: C. acnes (formerly Propionibacterium acnes) is an anaerobic Gram-positive rod that causes delayed/subacute post-cataract endophthalmitis, typically months to years after surgery. Characteristic features:
- White capsular plaque or opacity on the posterior lens capsule (organisms sequestered in capsular bag)
- Recurrent anterior uveitis with granulomatous KP
- Minimal pain and injection
- Transient response to steroids only
- Diagnosis: Anaerobic culture held for 14 days
- Treatment: Vitrectomy with posterior capsulectomy + intravitreal vancomycin; removal of IOL and entire capsular bag if recurs
Q9. When do you choose evisceration over enucleation in panophthalmitis?
A: In acute panophthalmitis with active infection, evisceration is preferred over enucleation for several reasons:
- Evisceration is a faster, simpler procedure with less surgical trauma
- Preserves the scleral shell for a better cosmetic outcome with an implant
- In active meningitis risk - evisceration leaves sclera intact, reducing the theoretical risk of spreading infection along the optic nerve to the CNS (though this is debated)
- Enucleation is preferred when: sympathetic ophthalmia risk (perforating injury with uveal prolapse), orbital extension that cannot be controlled by evisceration, or intraocular malignancy is suspected
Q10. What is sympathetic ophthalmia and why is it relevant to panophthalmitis management?
A: Sympathetic ophthalmia is a bilateral granulomatous panuveitis affecting the uninjured (sympathizing) eye, triggered by exposure of uveal antigens in the injured (exciting) eye. It is relevant because:
- Any penetrating trauma with uveal prolapse carries this risk
- Onset: typically 2 weeks to 3 months after injury (rarely up to years)
- Management: Enucleation of the exciting eye within 2 weeks of injury may prevent development
- If sympathetic ophthalmia has already developed, enucleation of the exciting eye will NOT protect the sympathizing eye
- Treatment of established cases: high-dose systemic steroids + immunosuppressants
Q11. What is the role of systemic antibiotics in endophthalmitis/panophthalmitis?
A:
- In post-cataract endophthalmitis: systemic antibiotics provide NO additional benefit (EVS, 1995) and are NOT routinely recommended
- However, fluoroquinolones (moxifloxacin) achieve reasonable intraocular levels and are used in:
- Bleb-related endophthalmitis - oral moxifloxacin for 10-14 days
- Post-traumatic panophthalmitis - especially high-risk cases
- Endogenous endophthalmitis - systemic antibiotics are KEY to treatment (targeting the primary source)
- IV antibiotics are reserved for severe systemic sepsis or endogenous cases
Q12. What precautions must be taken while doing a vitreous tap?
A:
- Informed consent, sterile technique
- Topical/subconjunctival/retrobulbar anaesthesia as appropriate
- Use a 23-25G needle on a tuberculin syringe
- Entry site: 3.5 mm (aphakic/pseudophakic) or 4 mm (phakic) from limbus in the inferotemporal quadrant
- Aspirate 0.2-0.3 mL of vitreous (not more - risk of retinal detachment)
- Dry tap may occur in very inflamed eyes - proceed with intravitreal antibiotics anyway
- Send immediately for cultures (blood agar, chocolate agar, Sabouraud, thioglycolate for anaerobes)
- Smears: Gram stain, Giemsa, Methenamine-silver
Q13. What are the risk factors for post-operative endophthalmitis after cataract surgery?
A:
- Surgical factors: Wound leak, posterior capsular rupture with vitreous loss, intraoperative vitreous in the wound
- Patient factors: Blepharitis, conjunctivitis, nasolacrimal duct obstruction, diabetes, immunosuppression
- Exposed/intact sutures, filtering bleb (trabeculectomy patients)
- Failure to use povidone-iodine preoperatively
- Prolonged surgery time
Prevention: 5% povidone-iodine conjunctival prep (proven) + intracameral antibiotics at end of surgery.
Q14. List the differences between exogenous and endogenous endophthalmitis.
A:
| Feature | Exogenous | Endogenous |
|---|---|---|
| Source | External (surgery, trauma, corneal ulcer) | Internal (haematogenous) |
| Laterality | Unilateral | Can be bilateral |
| Onset | Acute to subacute | Variable |
| Systemic illness | Usually absent | Usually present (sepsis, liver abscess, IV drug use) |
| Anterior segment | Severe hypopyon, wound leak | Less severe anteriorly initially |
| Common organisms | S. epidermidis, Bacillus, Streptococcus | S. aureus, Klebsiella, Candida |
| Blood cultures | Not usually needed | Always needed |
| Treatment | Intravitreal antibiotics ± PPV | Systemic + intravitreal antibiotics |
Q15. A patient with Klebsiella liver abscess develops sudden visual loss. What do you suspect and how would you manage it?
A: This is classic for endogenous Klebsiella endophthalmitis, a well-recognised syndrome particularly in Southeast Asian patients with diabetes and Klebsiella liver abscess. Features:
- Rapid, catastrophic visual loss
- Often bilateral
- Choroidal and retinal abscesses on fundoscopy/B-scan
- Associated with bacteraemia
Management:
- Urgent ophthalmology consultation
- Blood cultures, vitreous tap for cultures
- IV antibiotics targeting Klebsiella (ceftriaxone or fluoroquinolone based on sensitivity)
- Intravitreal antibiotics (ceftazidime + vancomycin)
- Pars plana vitrectomy in selected cases
- Management of the primary source (liver abscess - drainage)
- Prognosis: Very poor; many patients lose vision permanently despite aggressive treatment.
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease - Chapter 29 (Eye), pp. 1199/1216
- Wills Eye Manual - Office and Emergency Room Diagnosis and Treatment of Eye Disease (12.13 Postoperative Endophthalmitis; 12.14 Chronic Postoperative Uveitis)
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition
Panophthalmitis case presentation for residency notes and viva questions and answers in detail ophthalmology
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
I now have comprehensive, authoritative material from multiple textbooks. Here is the complete, structured residency document:
PANOPHTHALMITIS
Residency Notes, Case Presentation & Viva Q&A
Ophthalmology
PART 1 - CASE PRESENTATION
Chief Complaint
A 45-year-old male farmer presents with severe pain, rapidly progressive loss of vision, redness, swelling of the right eyelid, and purulent discharge for 3 days, following a penetrating injury with an agricultural implement 5 days ago.
History of Present Illness
- Right eye struck by a wooden stick while working in the field (day 0)
- Taken to a peripheral centre; primary wound repair done same day
- Day 2: Pain increasing, eye became increasingly red
- Day 3: Vision dropped to finger counting
- Day 5 (today): Vision only light perception, lids swollen shut, purulent discharge
- Fever and malaise for 2 days
- No similar episode before; no injury to the left eye
Past History / Review of Systems
- No diabetes, no immunosuppression, no long-term medication
- No prior ocular surgery
- No known drug allergies
- Immunisation history: Tetanus status unknown
Examination
Vitals: Temp 38.6°C, Pulse 98/min, BP 128/80 mmHg, SpO₂ 98% RA
Right Eye
| Parameter | Finding |
|---|---|
| Visual Acuity | PL + (perception of light positive) |
| Lids | Marked oedema, erythema, lagophthalmos, ecchymosis |
| Conjunctiva | 360° chemosis, severe conjunctival injection, copious mucopurulent discharge |
| Cornea | Diffuse oedema, stromal infiltrate, ring ulcer/abscess at periphery |
| Anterior Chamber | Hypopyon (5 mm), dense fibrinous membrane, 4+ cells and flare |
| Iris | Congested, muddy brown, details poorly seen |
| Pupil | Mid-dilated, poorly reacting |
| Lens | Cannot assess |
| Red Reflex | Absent |
| Vitreous (B-scan) | Dense echogenic vitreous opacities; posterior vitreous membrane; choroidal thickening |
| Fundus | Not visible |
| Extraocular Movements | Restricted in all directions |
| Proptosis | +3 mm (exophthalmometer) |
| IOP | Not recordable; eye hypotonus on palpation |
| Wound | 3 mm corneoscleral laceration at 10 o'clock, partially gaping |
Left Eye
Normal examination; VA 6/6; IOP 14 mmHg
Investigations
- B-scan ultrasonography RE - dense vitreous echoes (vitritis/abscess), choroidal thickening, no obvious IOFB; membrane formation posteriorly
- CT orbit (axial + coronal, 1 mm cuts) - proptosis RE, thickened posterior coats, orbital fat stranding; no retained metallic IOFB
- Vitreous tap (0.2 mL) - sent for:
- Gram stain (polymorphs, Gram-positive rods suggestive of Bacillus spp.)
- Giemsa stain
- Culture: Blood agar, Chocolate agar, Sabouraud agar, Thioglycolate broth (anaerobes)
- Blood cultures x2 (before antibiotics)
- CBC: WBC 15,200 (neutrophilia 84%), Hb 12.8, platelets normal; ESR 72 mm/hr; CRP elevated
- RBS: 98 mg/dL
- Renal function: Normal
- Tetanus toxoid status: Unverified
Diagnosis
Right Eye Panophthalmitis - Post-traumatic, exogenous, following penetrating injury with organic (agricultural) material, complicated by orbital cellulitis
Provisional Microbiological Diagnosis
Bacillus cereus endophthalmitis (Gram-positive rods on Gram stain, agricultural injury, fulminant course, ring corneal abscess, high fever, and proptosis are characteristic)
PART 2 - COMPLETE DISEASE NOTES
1. DEFINITION
Panophthalmitis is suppurative inflammation involving all coats of the eye - the retina, uveal tract (choroid + ciliary body + iris), and sclera - extending beyond the sclera into the orbital tissues.
"Panophthalmitis is the term used to describe inflammation of the interior of the eye that extends into the uvea and sclera... applied to eye inflammation involving the retina, choroid, and sclera extending into the orbit."
- Robbins, Cotran & Kumar Pathologic Basis of Disease
It is the most severe and advanced form of intraocular infection, representing failed or overwhelmed endophthalmitis.
2. CLASSIFICATION
By Source of Infection
| Type | Route | Common Causes |
|---|---|---|
| Exogenous | Direct inoculation from environment | Penetrating trauma, post-surgical (cataract, vitrectomy, trabeculectomy), corneal ulcer perforation, IOFB |
| Endogenous | Haematogenous spread from systemic infection | Bacterial sepsis, endocarditis, liver abscess (Klebsiella), fungemia (IV drug use, candidemia), pulmonary infection |
"Endophthalmitis is classified as exogenous (originating in the environment and gaining access to the eye's interior through a wound as a complication of surgery or penetrating injury) or endogenous (delivered to the eye hematogenously, e.g., secondary to pulmonary infections)."
- Robbins Pathology
Exogenous infections account for >80% of all cases (Tietz Textbook of Laboratory Medicine).
By Timing (Post-surgical)
- Acute - days after surgery (most common)
- Subacute/Chronic - weeks to months post-surgery (Cutibacterium acnes, fungi)
- Bleb-associated - complication of filtering surgery (trabeculectomy)
3. CAUSATIVE ORGANISMS
Post-cataract extraction (Wills Eye Manual)
| Rank | Organism |
|---|---|
| Most common | Staphylococcus epidermidis (coagulase-negative Staph) |
| Common | S. aureus, Streptococcal species |
| Less common | Gram-negatives: Pseudomonas, Klebsiella, Proteus, E. coli, Haemophilus influenzae, Bacillus, Enterobacter |
| Rare | Anaerobes, fungi |
Post-vitrectomy
- S. epidermidis
Post-intravitreal injection
- S. epidermidis, oral Streptococci
Bleb-associated (filtering surgery)
- Streptococcus spp. and Gram-negatives (more virulent than post-cataract)
Post-traumatic (penetrating injury)
- Staphylococcus spp. and Bacillus spp. - ~90% of culture-positive cases
- Bacillus cereus - especially agricultural injuries; notoriously virulent; mixed flora from organic matter increases fungal risk too
- Classic Bacillus triad: high fever + leukocytosis + corneal ring abscess + proptosis + rapid visual deterioration
Endogenous bacterial
- Bacillus cereus (IV drug users)
- Streptococcus, Neisseria meningitidis, S. aureus, H. influenzae
- Klebsiella pneumoniae - East Asia, associated with liver abscess and diabetes
Endogenous fungal
- Candida albicans - IV drug users, post-surgical immunocompromised, indwelling catheters, candidemia
- Aspergillus - immunocompromised (neutropenic)
- Fluffy white vitreous opacities are characteristic of fungal endophthalmitis
Subacute/Chronic post-surgical
- Cutibacterium acnes (formerly Propionibacterium acnes) - anaerobe; white lens capsular plaque; needs 14-day anaerobic culture
4. PATHOGENESIS
Penetrating trauma OR Post-surgical wound leak OR Haematogenous seeding
↓
Microbial entry into vitreous cavity
↓
Vitritis - rapid, unimpeded growth
(vitreous = avascular, immune-privileged,
poor neutrophil access = minimal defence)
↓
Retinal injury (may be irreversible within hours)
↓
Suppurative choroiditis + scleritis
↓
PANOPHTHALMITIS - orbital extension
(proptosis, ophthalmoplegia, orbital cellulitis)
↓
Cavernous sinus thrombosis / Meningitis (rare)
"The retina poorly tolerates suppurative inflammation in the vitreous humor; a few hours may be sufficient to cause irreversible retinal injury."
- Robbins Pathology
5. CLINICAL FEATURES
Symptoms
- Severe, throbbing, deep orbital pain (worse than endophthalmitis)
- Rapid, progressive loss of vision (PL or worse)
- Redness - globe and eyelids
- Swelling of lids
- Mucopurulent discharge
- Photophobia
- Systemic: fever, chills, malaise (especially in endogenous type)
Anterior Segment Signs
- Lid oedema and erythema (may prevent lid opening)
- 360° conjunctival injection
- Chemosis
- Mucopurulent discharge
- Corneal oedema, stromal infiltrate, ring abscess/ulcer
- Hypopyon - fluid level of pus in anterior chamber (pathognomonic of suppurative intraocular infection)
- Dense fibrinous exudate in anterior chamber
- Flare 4+, cells 4+
- Muddy/congested iris
- Absent or severely reduced red reflex
- Critical signs: Hypopyon + fibrin + absent red reflex = endophthalmitis until proven otherwise
Posterior Segment Signs
- Vitritis (vitreous haze/cells)
- Vitreous abscess
- Retinal infiltrates, flame haemorrhages ± white centres (Roth spots)
- Retinal/subretinal/choroidal abscesses
- Retinal detachment (late complication)
- Iris microabscesses (endogenous)
Signs Specific to Panophthalmitis (Orbital Extension)
- Proptosis (exophthalmos)
- Restricted extraocular movements in all directions (painful)
- Lid oedema extending beyond orbital rim
- Orbital pain on palpation and on movement
- Soft tissue swelling of the entire orbit
- (May progress to cavernous sinus thrombosis - emergency)
6. INVESTIGATIONS
Ocular
-
B-scan ultrasonography (mandatory when posterior pole not visible):
- Dense vitreous echoes (vitritis)
- Vitreous membranes / abscess
- Choroidal thickening / detachment
- Retinal detachment
- Rules out IOFB (metallic/non-metallic)
- Establishes baseline for monitoring treatment response
-
Intraocular fluid sampling (cultures - cornerstone of management):
- Vitreous aspirate preferred (higher diagnostic yield than aqueous)
- Aqueous paracentesis if vitreous cannot be obtained
- Volume: 0.2-0.3 mL (not more - retinal detachment risk)
- Stains: Gram stain, Giemsa stain, Methenamine-silver (fungi), KOH prep (fungi)
- Culture media:
- Blood agar (aerobic bacteria)
- Chocolate agar (Haemophilus, Neisseria)
- Sabouraud's agar (fungi)
- Thioglycolate broth (anaerobes)
- For C. acnes: Anaerobic culture held for 14 days
-
CT orbit (axial + coronal, 1 mm cuts):
- Assess orbital extension
- Detect retained IOFB (metallic)
- Rule out intracranial extension / cavernous sinus thrombosis
- Assess sinus pathology (endogenous from sinusitis)
- Note: MRI is contraindicated if metallic IOFB suspected
Systemic (Endogenous / Uncertain Aetiology)
- Blood cultures x2 (before antibiotics)
- CBC, ESR, CRP
- Blood sugar (rule out undetected diabetes)
- Renal and liver function tests
- Urine culture
- Chest X-ray
- Echocardiogram (rule out infective endocarditis if bacteraemia)
- Lumbar puncture (only if meningeal signs present)
- HIV serology, CD4 count (if immunocompromised suspected)
- Infectious disease specialist consultation
7. TREATMENT
A. Immediate Medical Treatment
Step 1 - Secure samples FIRST, then inject antibiotics.
Intravitreal Antibiotics (most critical; highest intraocular concentrations)
| Drug | Dose | Coverage |
|---|---|---|
| Vancomycin | 1 mg/0.1 mL | Gram-positive (including MRSA) |
| Ceftazidime | 2.2-2.25 mg/0.1 mL | Gram-negative (including Pseudomonas) |
| Amikacin | 0.4 mg/0.1 mL | Gram-negative alternative (penicillin allergy) - use with caution (macular infarction risk) |
| Clindamycin | 1 mg/0.1 mL | Anaerobic (Bacillus) coverage |
| Dexamethasone | 0.4 mg/0.1 mL | Adjunctive anti-inflammatory; in select cases with severe vitreous inflammation |
| Amphotericin B | 5-10 μg/0.1 mL | Fungal (if suspected) |
| Voriconazole | 100 μg/0.1 mL | Fungal alternative |
- Intravitreal antibiotics may be repeated every 48-72 hours if needed
- For Bacillus: Vancomycin + Clindamycin are the agents of choice (Bacillus is resistant to beta-lactams)
Fortified Topical Antibiotics
- Vancomycin (50 mg/mL) + Tobramycin (15 mg/mL) - every hour around the clock for 24-48 hours
- Especially for bleb-related cases, wound leaks, or exposed sutures
Cycloplegia
- Atropine 1% eye drops 2-3 times daily
- Prevents posterior synechiae, reduces ciliary spasm, provides pain relief
Topical Steroids
- Prednisolone acetate 1% every hour (after 48 hours; do not start before cultures obtained and fungi ruled out)
B. Systemic Antibiotics
Post-cataract endophthalmitis: systemic antibiotics add NO benefit (EVS 1995) - not routinely used.
Give systemic antibiotics for:
- Traumatic panophthalmitis: ciprofloxacin 400 mg IV q12h OR moxifloxacin 400 mg PO/IV daily + cefazolin 1 g IV q8h
- Bleb-related: oral moxifloxacin for 10-14 days
- Endogenous endophthalmitis: systemic antibiotics are the CORNERSTONE (targeting primary source), dosages appropriate for meningitis/severe infection, guided by cultures and ID specialist, IV antibiotics for at least 2 weeks
- IV drug users with suspected Bacillus: aminoglycoside + clindamycin
Tetanus prophylaxis (if open trauma and not up-to-date): tetanus toxoid 0.5 mL IM
C. Surgical Management
1. Vitreous Tap (Tap and Inject)
- When vision is hand motions (HM) or better at presentation (post-cataract)
- Aspirate 0.2 mL vitreous + intravitreal antibiotics at bedside
- Provides specimen + delivers highest possible drug concentration
2. Pars Plana Vitrectomy (PPV)
- Indication post-cataract (EVS): Vision = light perception or worse at presentation
- PPV + intravitreal antibiotics when vision is LP for post-cataract endophthalmitis
- May benefit bleb-related, traumatic, or endogenous cases regardless of vision level (EVS does not apply to these)
- Benefits: removes microbial load + inflammatory debris, allows diagnostic sampling, direct antibiotic delivery
- PPV role in C. acnes: vitrectomy + posterior capsulectomy ± IOL removal
3. IOFB Removal
- Removal of retained IOFB is paramount in controlling post-traumatic infection
- All removed IOFBs should be sent for culture
4. Evisceration
- Removal of all ocular contents while preserving the scleral shell
- Indicated when the eye is unsalvageable and infection is confined to the globe
- Preferred over enucleation in active panophthalmitis (faster, less surgical trauma, better cosmesis with implant)
- Note: Evisceration does NOT protect from sympathetic ophthalmia (uveal tissue may be left behind)
5. Enucleation
- Removal of the entire globe and optic nerve stump
- Indicated: risk of sympathetic ophthalmia (uveal prolapse + fellow eye threatened), orbital spread that cannot be controlled by evisceration alone, suspected intraocular malignancy, painful blind eye
8. PREVENTION
- 5% povidone-iodine conjunctival and eyelid preparation before all intraocular surgery - proven to reduce endophthalmitis risk
- Intracameral antibiotics at end of cataract surgery (reduces post-operative endophthalmitis risk)
- Topical perioperative antibiotics reduce bacterial load but have not been proven to reduce endophthalmitis rate, and may promote resistance
- Prophylactic intravitreal antibiotics for high-risk penetrating trauma (agricultural injuries)
- Prompt recognition and treatment of wound leaks and bleb infections
- Culture of all removed IOFBs
- Avoidance of talking/coughing by surgeon during intravitreal injection procedures
9. PATHOLOGY IMAGE
Exogenous panophthalmitis - This eye was removed following a foreign body injury. Suppurative inflammation of the entire globe has completely distorted the normal ocular architecture (from Robbins Pathologic Basis of Disease, Fig. 29.16):
10. PROGNOSIS
| Type | Visual Prognosis |
|---|---|
| Post-cataract (S. epidermidis, treated promptly) | Relatively good |
| Bleb-related (Streptococcus) | Poor; often leads to blindness or eye loss |
| Post-traumatic (Bacillus cereus) | Very poor; often requires evisceration |
| Endogenous (Klebsiella, bilateral) | Very poor |
| Endogenous fungal (Candida, early treatment) | Moderate with systemic + intravitreal antifungals |
| C. acnes | Good if diagnosed and treated appropriately |
PART 3 - VIVA QUESTIONS AND ANSWERS
Q1. Define panophthalmitis and distinguish it from endophthalmitis.
A: Endophthalmitis is suppurative inflammation of the interior of the eye involving the vitreous humor. Panophthalmitis is inflammation that extends further to involve the uvea, sclera, and orbit. In clinical terms, panophthalmitis is endophthalmitis with orbital signs - proptosis, restricted and painful extraocular movements, and orbital cellulitis - in addition to all the features of endophthalmitis (hypopyon, absent red reflex, vitritis). The distinction matters because panophthalmitis carries a worse prognosis, often requires more aggressive surgical management (evisceration/enucleation), and can spread to cause cavernous sinus thrombosis or meningitis.
Q2. What are the most common organisms in post-cataract endophthalmitis?
A: The most common is Staphylococcus epidermidis (coagulase-negative Staphylococcus), a member of normal lid and conjunctival flora. S. aureus and Streptococcal species are next. Gram-negative organisms (Pseudomonas, Klebsiella, E. coli) are less frequent but associated with worse outcomes. Fungi (Candida, Aspergillus) are rare in this setting. Anaerobes (Cutibacterium acnes) cause delayed/chronic post-cataract endophthalmitis with a distinctive presentation.
Q3. Which organism causes the most rapidly destructive post-traumatic endophthalmitis? Describe its clinical features.
A: Bacillus cereus, a Gram-positive, spore-forming anaerobic rod found in soil and organic matter. It produces multiple exotoxins (phospholipase C, cereulide, cereolysin) causing fulminant destruction.
Classical clinical picture:
- Agricultural/soil-contaminated penetrating injury
- High fever and leukocytosis (systemic toxin effect)
- Rapid visual deterioration within 12-24 hours
- Ring corneal abscess at the periphery of the cornea
- Severe proptosis
- Hypopyon with dense fibrinous membrane
Bacillus is resistant to beta-lactams. Treatment: vancomycin + clindamycin intravitreally; ciprofloxacin/moxifloxacin systemically. Visual prognosis is extremely poor; evisceration is frequently required.
Q4. Describe the Endophthalmitis Vitrectomy Study (EVS). What were its key findings?
A: The EVS (1995) was a landmark RCT of 420 patients with post-cataract extraction endophthalmitis. Key findings:
-
Immediate PPV is beneficial ONLY when vision at presentation is light perception (LP) or worse. When vision was hand motions (HM) or better, tap-and-inject and PPV had equivalent outcomes.
-
Systemic IV antibiotics (vancomycin + amikacin) added NO benefit to intravitreal antibiotics alone and are not routinely recommended.
-
Intravitreal vancomycin + amikacin/ceftazidime were the standard treatment.
Limitations of EVS:
- Applies ONLY to post-cataract extraction endophthalmitis
- Does NOT apply to: bleb-related, post-traumatic, or endogenous endophthalmitis
- In these other types, PPV may benefit regardless of visual acuity level
Q5. How do you differentiate panophthalmitis from orbital cellulitis clinically?
A:
| Feature | Panophthalmitis | Orbital Cellulitis |
|---|---|---|
| Primary site | Inside the globe | Orbital fat (outside globe) |
| Hypopyon | Present | Absent |
| Red reflex | Absent | Preserved |
| Vitreous opacities on B-scan | Present | Absent |
| Intraocular pressure | Low/hypotony (soft eye) | Normal or raised |
| Antecedent history | Ocular trauma, surgery, or endogenous sepsis | Sinusitis, dacryocystitis, facial infection |
| Proptosis | Present | Present |
| Restricted EOM | Present (from both orbital and intraocular pathology) | Present (from orbital pressure) |
Key point: The two conditions can coexist - panophthalmitis can cause orbital cellulitis by direct extension, and severe orbital cellulitis (from sinusitis) can cause secondary panophthalmitis.
Q6. What intravitreal antibiotics are used and at what doses?
A:
| Drug | Dose | Coverage |
|---|---|---|
| Vancomycin | 1 mg/0.1 mL | Gram-positives, MRSA |
| Ceftazidime | 2.2 mg/0.1 mL | Gram-negatives, Pseudomonas |
| Amikacin | 0.4 mg/0.1 mL | Gram-negatives (if penicillin allergic) |
| Clindamycin | 1 mg/0.1 mL | Anaerobes, Bacillus |
| Dexamethasone | 0.4 mg/0.1 mL | Adjunct anti-inflammatory |
| Amphotericin B | 5-10 μg/0.1 mL | Fungi |
| Voriconazole | 100 μg/0.1 mL | Fungi (better tolerated) |
Important: Aminoglycosides (amikacin, gentamicin) carry a risk of macular infarction and should be used with caution intravitreally. Bleb-related endophthalmitis: vancomycin 2 mg/0.1 mL + ceftazidime 2 mg/0.1 mL.
Q7. What is TASS? How do you differentiate it from infectious endophthalmitis?
A: Toxic Anterior Segment Syndrome (TASS) is a sterile non-infectious inflammatory reaction following intraocular surgery caused by toxic agents (incorrect pH/concentration of irrigating solutions, preservatives, instrument residues, detergents).
| Feature | TASS | Infectious Endophthalmitis |
|---|---|---|
| Onset | 6-24 hours post-op | Usually 2-7 days post-op |
| Pain | Minimal | Severe |
| Corneal oedema | Diffuse and severe (limbus-to-limbus) | Variable, less severe |
| Vitreous involvement | Absent/minimal | Present (vitritis) |
| Hypopyon | May be present | Present |
| Response to steroids | Rapid, dramatic | None or minimal |
| Cultures | Negative | Positive |
| Systemic symptoms | Absent | May be present (fever) |
TASS responds to intensive topical steroids; no antibiotics needed. If unclear, treat as infectious until proven otherwise.
Q8. Describe Cutibacterium acnes endophthalmitis.
A: C. acnes (formerly Propionibacterium acnes) is an anaerobic Gram-positive rod that causes a distinctive late-onset (months to years), subacute, chronic endophthalmitis following cataract surgery. The organism is sequestered in the capsular bag between the posterior capsule and IOL.
Classic features:
- Recurrent, granulomatous anterior uveitis with mutton-fat KP
- White plaque or opacities on the posterior lens capsule
- Minimal pain and injection
- Transient improvement with steroids only (then recurs)
- Hypopyon may be present
Diagnosis: Anaerobic culture held for 14 days (will be missed on routine culture). Vitreous sample with capsular plaque material gives highest yield.
Treatment:
- Vitrectomy + posterior capsulectomy + intravitreal vancomycin
- If recurs: removal of entire posterior capsule + IOL
Q9. When do you choose evisceration versus enucleation in panophthalmitis?
A:
Evisceration (remove contents, preserve scleral shell) is preferred in:
- Acute, active panophthalmitis with unsalvageable eye
- Infection limited to the globe (no orbital extension that cannot be controlled)
- Advantages: faster, simpler, less blood loss, better cosmetic result with orbital implant, preserves socket volume
Enucleation (remove entire globe) is preferred when:
- Risk of sympathetic ophthalmia is high (perforating injury with uveal prolapse - enucleation of exciting eye within 2 weeks may prevent SO)
- Orbital extension cannot be controlled by evisceration
- Intraocular malignancy is suspected or cannot be excluded
- Evisceration has failed to control infection
Critical point: Sympathetic ophthalmia can follow evisceration (if uveal tissue is inadvertently retained), so some surgeons prefer enucleation in traumatic panophthalmitis with extensive uveal prolapse.
Q10. What is sympathetic ophthalmia (SO)? Why is it relevant to penetrating ocular trauma management?
A: SO is a rare, bilateral granulomatous panuveitis that affects the uninjured (sympathizing) eye weeks to months after penetrating trauma or surgery to the other (exciting) eye. It is an autoimmune response to uveal antigens exposed at the time of injury.
Relevance to panophthalmitis/trauma management:
- Any penetrating trauma with uveal prolapse carries SO risk
- Enucleation of the exciting eye within 2 weeks of injury may prevent SO developing in the sympathising eye
- If SO has already developed, enucleation of the exciting eye will NOT protect the sympathising eye
- Treatment of established SO: high-dose systemic steroids + immunosuppressants (mycophenolate, azathioprine, cyclosporine)
Q11. What are the specific features of endogenous endophthalmitis and how is it managed?
A: Endogenous endophthalmitis occurs via haematogenous spread from a systemic source. Patients are typically acutely ill, immunocompromised, post-hospitalisation, on indwelling catheters, or IV drug users.
Signs (Wills Eye Manual): Chorioretinitis, vitreous cells and debris, anterior chamber cell and flare, hypopyon, iris microabscesses, absent red reflex, retinal inflammatory infiltrates, flame-shaped haemorrhages ± white centres, retinal/subretinal/choroidal abscesses, and panophthalmitis with proptosis and restricted EOM. May be bilateral.
Key organisms:
- Bacillus cereus (IV drug users)
- Klebsiella pneumoniae (East Asia, liver abscess, diabetes)
- S. aureus, Streptococci, H. influenzae, N. meningitidis
- Candida (fungemia, indwelling lines, post-surgical)
- Aspergillus (immunocompromised)
Management:
- Hospitalisation; co-management with infectious disease
- Blood cultures x2 + cultures from all indwelling lines, urine, wound
- Chest X-ray, echocardiogram (rule out endocarditis)
- Lumbar puncture only if meningeal signs present
- IV broad-spectrum antibiotics (dosages for severe infection/meningitis) - guided by cultures; maintained for at least 2 weeks
- Topical cycloplegic + steroid
- Intravitreal antibiotics if significant vitreous involvement
- PPV if severe or non-responsive to therapy
- Treat underlying source (drain liver abscess, remove infected line, etc.)
- IV drug users with Bacillus: aminoglycoside + clindamycin
Q12. What are the risk factors for post-operative endophthalmitis after cataract surgery?
A:
Patient factors:
- Blepharitis, chronic conjunctivitis, dacryocystitis (nasolacrimal duct obstruction)
- Diabetes mellitus
- Immunosuppression (steroids, chemotherapy, HIV)
- One-eyed patient (increased threshold for surgery but higher perceived risk)
Surgical factors:
- Posterior capsular rupture with vitreous loss
- Wound leak, gaping incision, exposed/intact suture
- Vitreous to wound (suction onto incision)
- Prolonged operative time
- Failure to use preoperative povidone-iodine
Post-operative factors:
- Filtering bleb (trabeculectomy patients - lifelong increased risk)
- Wound dehiscence
- Non-compliance with postoperative drops
Prevention (evidence-based):
- 5% povidone-iodine preparation (proven)
- Intracameral cefuroxime at end of surgery (ESCRS data)
- Topical antibiotics: reduce bacterial load but not proven to reduce endophthalmitis rates
Q13. Describe the technique of vitreous tap and intravitreal antibiotic injection.
A:
- Informed consent; explain the procedure
- Topical anaesthesia (proparacaine/amethocaine); peribulbar/retrobulbar block if needed
- Strict aseptic technique: povidone-iodine preparation, sterile drape, sterile gloves
- 25 or 27G needle attached to a tuberculin syringe
- Entry site: 3.5 mm from limbus (pseudophakic/aphakic) or 4.0 mm from limbus (phakic) in the inferotemporal quadrant
- Aspirate 0.2-0.3 mL of vitreous fluid (undiluted, "dry" tap)
- Dry tap may occur in very inflamed eyes; proceed with injection regardless
- Send immediately for: Gram stain, Giemsa, Methenamine-silver stain; Blood agar, Chocolate agar, Sabouraud agar, Thioglycolate culture
- Change needle; inject antibiotics (vancomycin 1 mg/0.1 mL, then ceftazidime 2.2 mg/0.1 mL) as two separate injections at the same site or different sites
- Check IOP after injection (avoid central retinal artery occlusion)
- Pad and patch; review next day
Q14. What is the role of systemic steroids in endophthalmitis/panophthalmitis?
A: The role of steroids is controversial:
- They reduce the inflammatory response that contributes to retinal and visual damage
- However, they can potentially suppress host immunity and impair clearance of infection
- Intravitreal dexamethasone (0.4 mg/0.1 mL) is used in select cases with severe vitreous inflammation, after obtaining samples and starting antibiotics
- Topical steroids are started after 48 hours (once fungi are ruled out and antibiotic therapy initiated)
- Systemic steroids: Defined role only after infection is controlled; used in specific contexts (e.g., once culture-directed antibiotics are working in endogenous cases)
- Critical rule: Do NOT start steroids before ruling out fungal infection (can lead to catastrophic fungal proliferation)
Q15. A young IV drug user presents with sudden bilateral visual loss and fluffy white vitreous opacities. What is your diagnosis and management?
A: The diagnosis is endogenous Candida endophthalmitis (bilateral, IV drug use, fluffy white vitreous opacities = classic "string of pearls" or "snowball" lesions).
Candida seeding typically begins in the choroid (highly vascular), then extends to retina producing chorioretinitis, and subsequently to vitreous to produce full-blown endophthalmitis. (Tietz Textbook of Lab Medicine)
Management:
- Hospitalise; ophthalmology + infectious disease co-management
- Blood cultures, urine, all line cultures
- Echocardiogram (rule out endocarditis)
- Systemic antifungals: IV fluconazole or micafungin (echinocandin), depending on Candida species and sensitivity
- Intravitreal antifungal: Amphotericin B 5-10 μg/0.1 mL OR Voriconazole 100 μg/0.1 mL
- Partial vitrectomy if significant vitreous involvement unresponsive to intravitreal therapy
- Remove all indwelling lines/catheters
- Drug rehabilitation referral
- Monitor closely - can progress during antifungal therapy
IV drug users: Bacillus cereus must also be considered - give aminoglycoside + clindamycin until cultures confirm
Q16. What complications can arise from untreated or inadequately treated panophthalmitis?
A:
Ocular complications:
- Permanent blindness (no light perception)
- Retinal detachment
- Phthisis bulbi (shrunken, disorganised, non-functional eye)
- Corneal scarring, perforation
- Secondary glaucoma or hypotony
- Sympathetic ophthalmia (if penetrating trauma with uveal prolapse)
Orbital/periorbital complications:
- Orbital abscess
- Orbital cellulitis (if not already present)
- Subperiosteal abscess
Intracranial/systemic complications:
- Cavernous sinus thrombosis (emergency - septic thrombosis, high mortality)
- Meningitis (spread along optic nerve sheaths)
- Brain abscess
- Systemic sepsis and septicaemia
- Death (rare; more likely with endogenous source and immunocompromised host)
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease - Chapter 29 (Eye), pp. 1199/1216
- Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease - Sections 12.13, 12.15, 12.16, 12.17
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition
- Tietz Textbook of Laboratory Medicine, 7th Edition - Eye Infections
- Tintinalli's Emergency Medicine: A Comprehensive Study - Ophthalmologic Infections
This is a shared conversation. Sign in to Orris to start your own chat.