What is receptor classification of receptor difference between slow and fast receptors properties of receptors? answer for 15 marks mbbs first year
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full 15-mark answer.
Receptor Classification, Slow vs. Fast Receptors, and Properties of Receptors
(MBBS First Year - 15 Marks)
1. DEFINITION OF A RECEPTOR
A receptor is a macromolecular protein (on the cell surface, within the cytoplasm, or in the nucleus) that specifically recognizes and binds an endogenous ligand (hormone, neurotransmitter, drug) and transduces that binding into a cellular response. Receptors are distinct from mere carrier proteins or enzymes because binding initiates signal transduction.
2. CLASSIFICATION OF RECEPTORS
Receptors are classified by structure and transduction mechanism into four major types:
TYPE I - Ligand-Gated Ion Channels (Ionotropic Receptors / "Fast" Receptors)
These receptors are directly linked to an ion channel. Ligand binding opens or closes the channel within milliseconds, without any intermediate steps.
Structure: The receptor protein itself forms the ion channel - it is a multimeric protein spanning the membrane several times.
Examples:
- Nicotinic acetylcholine receptor (nAChR) - at the neuromuscular junction; opens Na+/K+ channels
- GABA-A receptor - opens Cl- channels (inhibitory)
- Glycine receptor - opens Cl- channels (inhibitory)
- NMDA and AMPA glutamate receptors - opens Na+/K+/Ca2+ channels (excitatory)
- 5-HT3 receptor - opens Na+/K+ channels
Mechanism: Ligand binds → conformational change → ion channel opens directly → change in membrane potential (depolarization or hyperpolarization).
TYPE II - G Protein-Coupled Receptors (GPCRs / Metabotropic Receptors / "Slow" Receptors)
The largest family of cell-surface receptors. Binding activates a heterotrimeric G protein (Gα + Gβγ), which then modulates second messengers and/or ion channels indirectly.
Structure: Single polypeptide with 7 transmembrane (7-TM) domains; also called heptahelical receptors.
Subclasses by G protein family:
| G Protein | Effect | Example Receptor |
|---|---|---|
| Gs | Activates adenylyl cyclase → ↑cAMP | β-adrenergic, D1 dopamine |
| Gi | Inhibits adenylyl cyclase → ↓cAMP | M2 muscarinic, α2-adrenergic |
| Gq | Activates phospholipase C-β → ↑IP3/DAG/Ca2+ | M1/M3 muscarinic, α1-adrenergic |
| G12/13 | Activates Rho GEFs | Thrombin receptor |
Examples:
- Muscarinic ACh receptor (mAChR): at cardiac parasympathetic synapse - activates Gi, opens GIRK channels → slows heart rate
- Adrenergic receptors (α and β)
- Dopamine, serotonin (5-HT1, 5-HT2, 5-HT4), opioid receptors
Mechanism: Ligand binds → G protein activated → Gα-GTP dissociates from Gβγ → both subunits modulate effectors (adenylyl cyclase, PLC, ion channels) → second messengers (cAMP, IP3, DAG, Ca2+) produced → cellular response. Onset: seconds to minutes.
(Goodman & Gilman's Pharmacological Basis of Therapeutics; Medical Physiology [Boron & Boulpaep])
TYPE III - Enzyme-Linked (Catalytic) Receptors
These receptors have intrinsic enzymatic activity (usually tyrosine kinase) in their intracellular domain, activated upon ligand binding.
Subtypes:
- Receptor Tyrosine Kinases (RTKs): Insulin receptor, PDGF receptor, EGF receptor, VEGF receptor. Ligand binding causes receptor dimerization and autophosphorylation on tyrosine residues → downstream signaling (SH2-domain proteins, MAP kinase cascade, PI3K/Akt pathway).
- Receptor Serine/Threonine Kinases: TGF-β receptor → activates SMAD proteins.
- Membrane-bound Guanylyl Cyclase: Natriuretic peptide receptor → produces cGMP.
- Cytokine Receptors (JAK-STAT pathway): Receptors for interleukins, growth hormone, prolactin - activate JAK kinases → STAT transcription factors.
Onset: Minutes to hours.
TYPE IV - Nuclear (Intracellular) Receptors
These receptors are located inside the cell (cytoplasm or nucleus) rather than on the membrane. Their ligands must be lipid-soluble to diffuse across the cell membrane.
Ligands: Steroid hormones (glucocorticoids, mineralocorticoids, androgens, estrogens), thyroid hormones (T3/T4), vitamin D, retinoic acid.
Mechanism: Lipophilic ligand diffuses across membrane → binds receptor in cytoplasm or nucleus → receptor-ligand complex acts as transcription factor → binds specific DNA sequences (hormone response elements/HREs) → regulates gene expression → protein synthesis changes.
Onset: Hours to days (gene transcription + translation required).
Structure: All share a conserved DNA-binding domain (zinc-finger motif), a ligand-binding domain, and a transactivation domain. The superfamily contains at least 48 genes.
(Medical Physiology [Boron & Boulpaep]; Goodman & Gilman's)
3. FAST vs. SLOW RECEPTORS - A DETAILED COMPARISON
This distinction is central to first-year pharmacology and physiology:
| Feature | Fast Receptors (Ionotropic) | Slow Receptors (Metabotropic/GPCRs) |
|---|---|---|
| Structural type | Ligand-gated ion channel (multimeric) | 7-TM GPCR (single polypeptide) |
| Transduction | Direct: ligand opens channel | Indirect: via G protein + second messengers |
| Onset of response | Milliseconds (1-10 ms) | Seconds to minutes |
| Duration of response | Brief (ms range) | Prolonged (seconds-minutes) |
| Second messengers | None required | cAMP, cGMP, IP3, DAG, Ca2+ |
| Effect | Change in membrane potential (depolarization or hyperpolarization) | Diverse: altered enzyme activity, gene expression, ion channel gating |
| Amplification | Low (1:1 or small) | High (one receptor activates thousands of second-messenger molecules) |
| Reversal | On ligand dissociation | Slower - requires GTPase activity (Gα) + phosphodiesterase action |
| Example (ACh system) | Nicotinic AChR at NMJ: Na+/K+ influx → depolarization → muscle contraction | Muscarinic M2 AChR at heart: activates Gi → GIRK channels open → hyperpolarization → ↓HR |
| Example (GABA system) | GABA-A: Cl- influx → fast inhibition | GABA-B: Gi-coupled → K+ channel opening → slow inhibition |
| Pharmacological use | Neuromuscular blockers act here (tubocurarine, succinylcholine) | Beta-blockers, antimuscarinics, opioids act here |
Classic Example to Remember: Both nicotinic and muscarinic receptors respond to acetylcholine but produce completely opposite effects on different tissues - the former is fast (milliseconds), the latter is slow (seconds) - explaining why ACh can both activate skeletal muscle AND slow the heart.
(Medical Physiology; Eric Kandel Principles of Neural Science 6th Edition; Katzung's Basic and Clinical Pharmacology 16th Edition)
4. PROPERTIES OF RECEPTORS
(a) Specificity
Receptors are highly specific for their ligand due to the complementary 3D structure (lock-and-key or induced-fit). A receptor binds only ligands with the correct molecular geometry. E.g., the muscarinic receptor binds muscarine and ACh but not nicotine.
(b) Affinity (Kd)
Affinity is the strength of binding between receptor and ligand, expressed as the dissociation constant (Kd) - the concentration of ligand that occupies 50% of receptors at equilibrium. A lower Kd = higher affinity. Affinity is measured using radioligand-binding assays and Scatchard plots.
(c) Saturability
Receptors are present in finite numbers. As ligand concentration increases, a maximum response is reached when all receptors are occupied - the response cannot be increased beyond this point regardless of further ligand addition.
(d) Reversibility
Receptor-ligand binding is generally reversible (non-covalent: ionic bonds, hydrogen bonds, van der Waals forces). Irreversible binding (covalent) occurs with certain drugs (e.g., organophosphates at acetylcholinesterase; aspirin at COX).
(e) Transduction (Signal Coupling)
The receptor must be coupled to an effector mechanism. Uncoupled receptors (due to mutations or disease) lose the ability to produce a response even when occupied.
(f) Desensitization (Tachyphylaxis)
Repeated or prolonged receptor stimulation leads to reduced response. Mechanisms include:
- Receptor phosphorylation by GRKs (G protein-coupled receptor kinases) → β-arrestin binding → receptor uncoupling
- Internalization (down-regulation): Receptor is removed from the cell surface via endocytosis → fewer surface receptors → diminished response
- Receptor degradation in lysosomes
(g) Up-regulation and Supersensitivity
Prolonged blockade or absence of agonist leads to an increase in receptor number (up-regulation) and heightened sensitivity. Clinically important: abrupt discontinuation of beta-blockers can precipitate rebound hypertension/angina due to up-regulated β-receptors.
(h) Spare Receptors (Receptor Reserve)
Many tissues have more receptors than required for a maximal response. The maximum effect can be achieved at submaximal receptor occupancy. This provides a safety margin and also explains why partial agonists may be full agonists in tissues with large receptor reserve.
(i) Selectivity
Some drugs act on one receptor subtype more than others - e.g., salbutamol is selective for β2 over β1 receptors. Selectivity differs from specificity (specificity = one receptor type; selectivity = preference within a family).
(j) Stereoselectivity
Receptors typically bind one optical isomer (enantiomer) far better than the other. E.g., L-norepinephrine is much more potent than D-norepinephrine at adrenergic receptors.
5. SUMMARY TABLE
| Receptor Class | Location | Mechanism | Speed | Example |
|---|---|---|---|---|
| Ionotropic (Type I) | Cell membrane | Ion channel | ms (Fast) | nAChR, GABA-A |
| GPCR (Type II) | Cell membrane | G protein → 2nd messenger | Seconds-min (Slow) | mAChR, β-adrenoceptor |
| Enzyme-linked (Type III) | Cell membrane | Intrinsic kinase / JAK | Minutes-hours | Insulin R, EGF R |
| Nuclear (Type IV) | Cytoplasm/Nucleus | Gene transcription | Hours-days | Glucocorticoid R, T3 R |
Key Sources:
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 14th Ed. - Table 3-1 (Classes of Receptors Relevant to Drug Actions)
- Medical Physiology (Boron & Boulpaep) - pp. 51-66, 327-328 (Ionotropic vs. metabotropic receptors)
- Eric Kandel: Principles of Neural Science, 6th Ed. - Fast/slow synaptic transmission
- Katzung's Basic and Clinical Pharmacology, 16th Ed. - GABA-A (fast) vs. GABA-B (slow) receptors
Fast and slow adapting receptors
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
I now have everything needed for a thorough answer. Let me compile it.
Fast and Slow Adapting Receptors
(MBBS First Year - Physiology)
1. RECEPTOR ADAPTATION - DEFINITION
When a constant, sustained stimulus is applied to a sensory receptor, the frequency of action potentials generated in its sensory nerve declines over time despite the stimulus remaining unchanged. This phenomenon is called receptor adaptation.
Receptors are classified based on how quickly they adapt:
- Rapidly adapting (phasic) receptors - adapt quickly, fire only at onset (and offset) of stimulus
- Slowly adapting (tonic) receptors - continue firing as long as the stimulus is maintained
(Guyton & Hall Textbook of Medical Physiology; Ganong's Review of Medical Physiology 26th Ed.)
2. FAST-ADAPTING (RAPIDLY ADAPTING / PHASIC) RECEPTORS
Definition
Receptors that respond strongly at the onset of a stimulus, then quickly reduce or cease firing even though the stimulus continues. They fire again at offset (when the stimulus is removed).
Also Called
- Phasic receptors
- Rate receptors
- Movement receptors
- "Change detectors"
Key Characteristics
- Fire at high frequency when stimulus is first applied
- Go silent within milliseconds to ~1 second during sustained stimulation
- Fire again when stimulus is removed (off-response)
- Cannot signal the continued presence of a stimulus
- Signal the rate of change of a stimulus, not its magnitude
Mechanism of Rapid Adaptation
Two main mechanisms (Guyton & Hall):
- Structural/viscoelastic redistribution - e.g., in the Pacinian corpuscle, fluid within the laminar capsule redistributes within hundredths of a second, so the distorting force no longer reaches the central nerve fiber
- Ionic accommodation - progressive inactivation of sodium channels in the nerve terminal membrane, reducing the generator potential
Examples of Fast-Adapting Receptors
| Receptor | Location | Stimulus Detected | Fiber Type |
|---|---|---|---|
| Pacinian corpuscle (RA2) | Deep dermis and subcutaneous tissue | Vibration (200-300 Hz), rapid pressure changes | Aβ |
| Meissner corpuscle (RA1) | Dermal papillae (fingertips, lips) | Lateral motion, tapping, slow vibration (1-300 Hz) | Aβ |
| Hair follicle receptors | Around hair base | Hair movement, light touch | Aβ |
| Semicircular canals | Inner ear | Rate of head rotation (angular acceleration) | CN VIII |
Functional Significance
- Detect change and movement - not constant conditions
- Rate/predictive function: By knowing how rapidly a change is occurring, the CNS predicts future states and adjusts motor responses ahead of time (e.g., balance when turning, limb position while running)
- Useful for detecting vibration (repeating on-off cycles)
- Pacinian corpuscles adapt to extinction within a few hundredths of a second - the fastest adapting receptor
3. SLOW-ADAPTING (SLOWLY ADAPTING / TONIC) RECEPTORS
Definition
Receptors that continue to fire action potentials as long as the stimulus is maintained, or at least for many minutes to hours. Firing rate is proportional to stimulus intensity throughout stimulation.
Also Called
- Tonic receptors
- "Static" receptors
Key Characteristics
- Fire during the entire duration of a sustained stimulus
- Firing rate is high initially, then settles to a steady level proportional to stimulus magnitude
- Keep the brain continuously informed about the status of body position and environment
- Detect both onset (dynamic phase) and steady-state (static phase) of a stimulus
Mechanism of Slow Adaptation
- Structural properties of the receptor allow continued deformation of the nerve terminal
- Sodium channels do not inactivate as quickly
- Accessory structures do not redistribute the stimulus force
Examples of Slow-Adapting Receptors
| Receptor | Location | Stimulus Detected | Fiber Type |
|---|---|---|---|
| Merkel cells (SA1) | Epidermis (superficial) | Sustained pressure, edges, Braille dots | Aβ |
| Ruffini endings (SA2) | Deep dermis, joints | Skin stretch, joint position, sustained pressure | Aβ |
| Muscle spindles (Ia, II) | Intrafusal muscle fibers | Muscle length and rate of change | Ia (Aα) |
| Golgi tendon organs | Musculotendinous junction | Muscle tension/force | Ib (Aα) |
| Joint capsule receptors | Joint capsule | Joint angle and position | Aβ |
| Vestibular macula receptors | Utricle, saccule | Linear acceleration, gravity | CN VIII |
| Arterial baroreceptors | Carotid sinus, aortic arch | Blood pressure | IX, X |
| Pain receptors (nociceptors) | All tissues | Noxious stimuli | Aδ, C fibers |
| Carotid/aortic chemoreceptors | Carotid/aortic bodies | PO2, PCO2, pH | IX, X |
Functional Significance
- Maintain postural tone - muscle spindles signal muscle length continuously
- Body position sense (proprioception) - joint and tendon receptors
- Blood pressure regulation - baroreceptors signal BP moment-to-moment
- Sustained pain warning - nociceptors do not fully adapt; this is protective
- Some slowly adapting receptors (baroreceptors) may take up to 2 days to adapt partially; nociceptors and chemoreceptors likely never fully adapt
4. ADAPTATION GRAPH (Guyton & Hall)
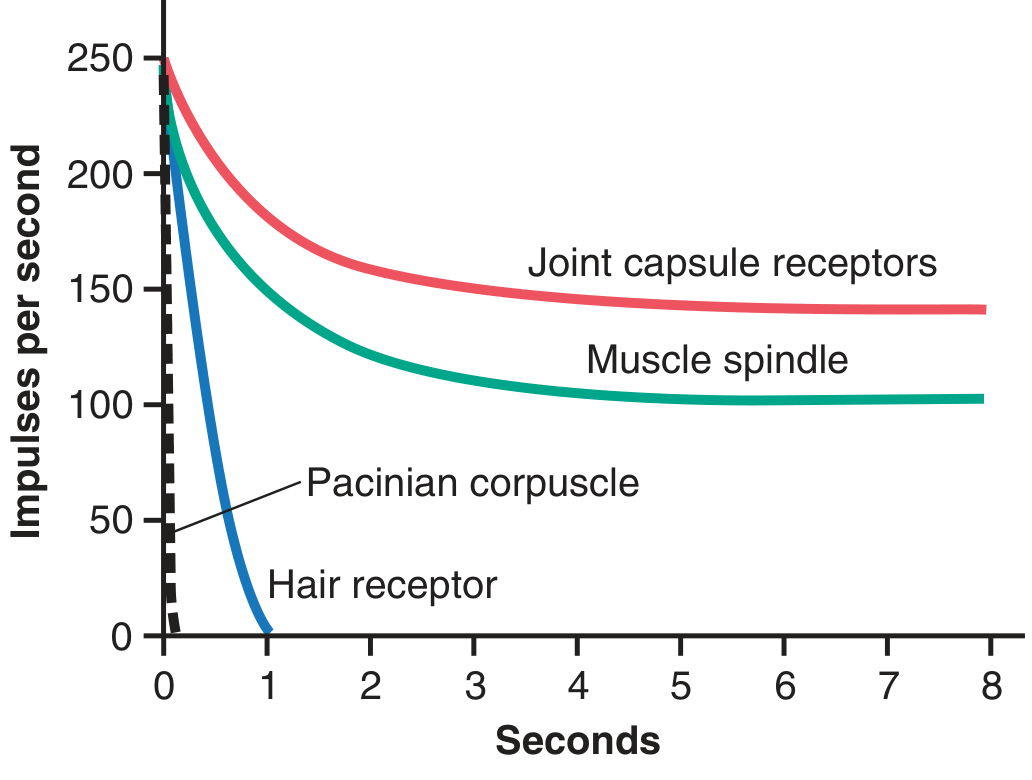
Figure 47.5 (Guyton & Hall): Impulses per second over 8 seconds for four receptor types. Pacinian corpuscle adapts to extinction within <1 second. Hair receptor adapts within ~1 second. Muscle spindle and joint capsule receptors maintain a high steady firing rate for the entire duration.
5. THE FOUR CUTANEOUS MECHANORECEPTORS - SA vs. RA Classification
(Kandel: Principles of Neural Science, 6th Ed. - Table 19-1)
| Feature | SA1 (Merkel) | RA1 (Meissner) | SA2 (Ruffini) | RA2 (Pacinian) |
|---|---|---|---|---|
| Adaptation | Slow | Fast | Slow | Fast |
| Location | Superficial (epidermis) | Superficial (dermal papillae) | Deep dermis, joints | Deep dermis/subcutaneous |
| Receptive field | Small, sharp borders | Small, sharp borders | Large, diffuse | Large, diffuse |
| Best stimulus | Edges, points, Braille | Lateral motion, tapping | Skin stretch | Vibration (200-300 Hz) |
| Frequency range | 0-100 Hz | 1-300 Hz | 0-100 Hz | 10-500 Hz |
| Firing during sustained pressure | Sustained (irregular) | Phasic at onset only | Sustained (regular) | Phasic at onset only |
| Function | Form, texture, fine detail | Grip, motion detection | Hand conformation, joint position | Vibration, tool use |
6. COMPARISON TABLE - FAST vs. SLOW ADAPTING RECEPTORS
| Feature | Fast-Adapting (Phasic) | Slow-Adapting (Tonic) |
|---|---|---|
| Other names | Rate/movement/phasic receptor | Tonic receptor |
| Response to sustained stimulus | Fires only at onset (and offset) | Fires throughout stimulus |
| Information conveyed | Rate of change, movement, velocity | Stimulus magnitude, steady state |
| What they detect | Change ("Is something changing?") | Continuation ("Is it still there?") |
| Adaptation speed | Milliseconds to ~1 second | Minutes to hours (or never) |
| Examples | Pacinian corpuscle, Meissner corpuscle, hair receptors, semicircular canals | Merkel cells, Ruffini endings, muscle spindles, GTOs, baroreceptors, nociceptors |
| Clinical/functional value | Vibration sense, motion, grip adjustment | Posture, proprioception, blood pressure control, sustained pain |
7. CLINICAL CORRELATIONS
- Vibration testing (128-Hz tuning fork): Tests Pacinian corpuscles (RA2) - rapidly adapting vibration detectors. Loss = dorsal column damage (diabetes, B12 deficiency, tabes dorsalis)
- Proprioception loss: Muscle spindles (SA) and joint receptors (SA) - tested by Romberg's sign; lost in posterior cord lesions
- Why pain persists: Nociceptors are non-adapting or very slowly adapting - this is protective (continued tissue damage must be signaled)
- Baroreceptor resetting: In chronic hypertension, baroreceptors gradually adapt to the new elevated pressure (over 1-2 days), explaining why they cannot maintain long-term blood pressure control
Key Sources:
- Guyton & Hall Textbook of Medical Physiology - Ch. 47, Adaptation of Receptors (pp. 585-586)
- Ganong's Review of Medical Physiology, 26th Ed. - pp. 173-174 (rapidly vs. slowly adapting, phasic vs. tonic)
- Kandel: Principles of Neural Science, 6th Ed. - Ch. 17 & 19 (SA1, SA2, RA1, RA2; Table 19-1)
Describe the connections and functions of thalamus and add a note on thalamic syndrome 15marks answer mbbs 1st year
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compile the complete 15-mark answer.
Connections and Functions of the Thalamus + Note on Thalamic Syndrome
(MBBS First Year - 15 Marks)
1. INTRODUCTION
The word thalamus comes from the Greek meaning "inner chamber". It is the largest component of the diencephalon, paired egg-shaped masses of gray matter located deep in the brain, forming the lateral walls of the third ventricle. It is the single most important relay station of the brain - nearly all sensory, motor, and limbic signals destined for the cerebral cortex pass through it. Notably, olfaction is the only sensory modality that reaches the cortex WITHOUT a thalamic relay.
2. ANATOMICAL LOCATION AND STRUCTURE
- Part of the diencephalon, rostral to the midbrain
- Two ovoid thalamic masses, one on each side of the third ventricle, connected at the midline by the massa intermedia (interthalamic adhesion) in ~70% of individuals
- Lateral to each thalamus is the posterior limb of the internal capsule
- The thalamic nuclei are divided by a Y-shaped band of myelinated axons called the internal medullary lamina into:
- Anterior nuclear group
- Medial nuclear group
- Lateral nuclear group
- The external medullary lamina covers the lateral surface; between it and the internal capsule lies the thalamic reticular nucleus
- Nuclei embedded within the lamina itself are the intralaminar nuclei
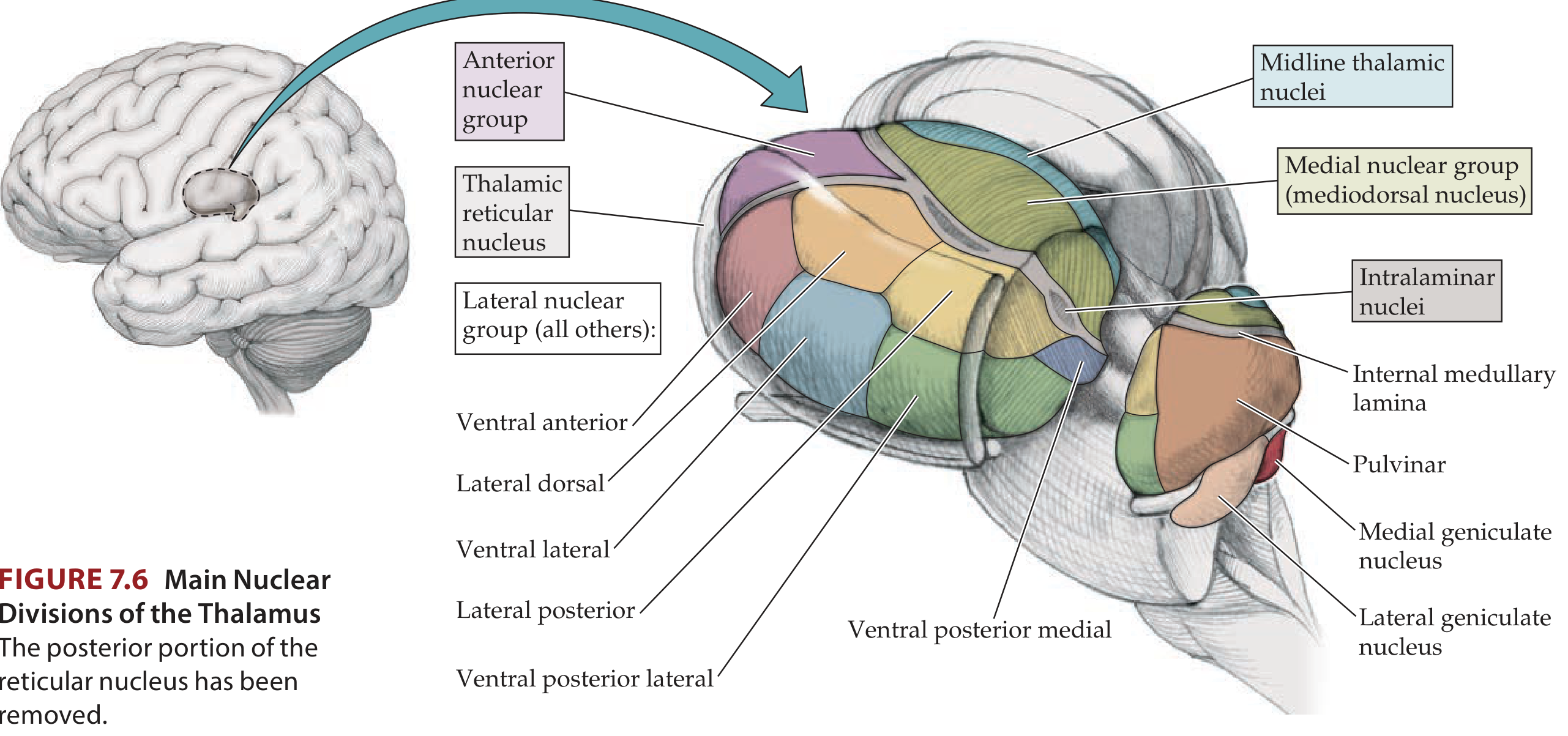
(Figure 7.6 - Neuroanatomy through Clinical Cases, 3rd Ed.: Main Nuclear Divisions of the Thalamus)
3. CLASSIFICATION OF THALAMIC NUCLEI
Thalamic nuclei fall into three major functional classes:
A. Relay Nuclei (Specific and Association)
- Receive inputs from defined pathways and project to specific cortical areas
- Have dense reciprocal feedback from the cortex (corticothalamic projections actually outnumber thalamocortical projections)
- Subdivided into specific relay nuclei and association relay nuclei
B. Intralaminar and Midline Nuclei (Non-specific / Diffuse projection)
- Project diffusely to wide areas of the cortex and striatum
- Involved in arousal and cortical excitability
C. Reticular Nucleus
- Unique: contains inhibitory (GABAergic) neurons
- Does NOT project to cortex; projects only to other thalamic nuclei
- Receives collaterals from both thalamocortical and corticothalamic axons
- Acts as a "gatekeeper" - samples traffic between thalamus and cortex and modulates thalamic relay
4. CONNECTIONS OF INDIVIDUAL THALAMIC NUCLEI
(Sources: Kaplan & Sadock's Comprehensive Textbook of Psychiatry; Neuroanatomy through Clinical Cases 3rd Ed.)
SPECIFIC RELAY NUCLEI (Lateral Nuclear Group)
| Nucleus | Afferents (Inputs) | Efferents (Outputs) | Function |
|---|---|---|---|
| Ventral Posterior Lateral (VPL) | Medial lemniscus, spinothalamic tract (from spinal cord) | Primary somatosensory cortex (SI, areas 3,1,2) | Pain, temperature, touch, pressure, proprioception from body |
| Ventral Posterior Medial (VPM) | Trigeminal lemniscus/trigeminothalamic tract; taste pathway (via NTS) | Somatosensory cortex + taste cortex (insula) | Pain, temperature, touch from face; taste |
| Lateral Geniculate Nucleus (LGN) | Optic tract (retina) | Primary visual cortex (area 17, calcarine sulcus) | Vision |
| Medial Geniculate Nucleus (MGN) | Inferior colliculus (via brachium) | Primary auditory cortex (areas 41/42, superior temporal gyrus) | Hearing |
| Ventral Lateral (VL) | Dentate nucleus of cerebellum (crossed) | Motor cortex (area 4), premotor cortex (area 6) | Control of voluntary movement (cerebellar input) |
| Ventral Anterior (VA) | Globus pallidus (internal), substantia nigra pars reticulata | Premotor cortex, supplementary motor area, frontal eye fields | Movement control via basal ganglia; eye/face/head movement |
ANTERIOR NUCLEAR GROUP
| Nucleus | Afferents | Efferents | Function |
|---|---|---|---|
| Anterior nucleus | Mammillary bodies of hypothalamus (via mammillothalamic tract); hippocampal formation | Cingulate cortex, parahippocampal gyrus | Emotion, learning, memory (part of Papez circuit) |
MEDIAL NUCLEAR GROUP
| Nucleus | Afferents | Efferents | Function |
|---|---|---|---|
| Mediodorsal (MD) nucleus | Amygdala, hypothalamus, brainstem, prefrontal cortex | Prefrontal cortex, premotor cortex, temporal cortex | Emotion, integration of sensory information, personality, executive function |
ASSOCIATION RELAY NUCLEI (Lateral Nuclear Group - Dorsal Tier)
| Nucleus | Afferents | Efferents | Function |
|---|---|---|---|
| Pulvinar | Superior colliculus, cerebellum, parieto-temporo-occipital cortices | Association cortex (parieto-temporo-occipital) | Integration of visual, auditory, and somatosensory information; behavioral orientation to relevant stimuli |
| Lateral Posterior (LP) | Superior colliculus, parietal cortex, pretectal area | Association cortex | Sensory integration (functions with pulvinar) |
| Lateral Dorsal (LD) | Pretectal area, hippocampus | Cingulate cortex, retrosplenial cortex | Emotion (functions with anterior nucleus) |
DIFFUSE PROJECTION (NON-SPECIFIC) NUCLEI
| Nucleus | Afferents | Efferents | Function |
|---|---|---|---|
| Intralaminar nuclei (central median, parafascicular) | Reticular formation, spinothalamic tract, globus pallidus | Basal ganglia, widespread cortex | Arousal, cortical activation, pain (crude) |
| Midline nuclei | Reticular formation, hypothalamus, striatum | Striatum, hippocampus, limbic cortex | Modulation of cortical excitability |
| Reticular nucleus | Cerebral cortex (collaterals), other thalamic nuclei | Other thalamic nuclei (not cortex) | Integration and gating of thalamic activity (inhibitory) |
5. FUNCTIONS OF THE THALAMUS
(a) Sensory Relay - "Gateway to Consciousness"
All sensory modalities except olfaction relay in the thalamus before reaching the cortex:
- Somatosensory (body) - VPL
- Somatosensory (face) and taste - VPM
- Vision - LGN
- Hearing - MGN
(b) Motor Integration
- VL nucleus relays cerebellar signals to motor cortex
- VA nucleus relays basal ganglia signals to premotor and supplementary motor cortices
- Thalamus is thus a critical link in both the corticopontocerebellar and corticostriatothalamic circuits
(c) Limbic and Emotional Functions
- Anterior nucleus is part of the Papez circuit (hypothalamus → mammillothalamic tract → anterior thalamus → cingulate cortex → hippocampus → fornix → hypothalamus)
- Mediodorsal nucleus connects amygdala and hypothalamus with prefrontal cortex - involved in emotion, motivation, and executive function
(d) Arousal and Consciousness
- Intralaminar and midline nuclei receive input from the ascending reticular activating system (ARAS)
- They project diffusely to the cortex and maintain the waking state and cortical excitability
- Bilateral thalamic damage can cause coma or akinetic mutism
(e) Memory
- Anterior nucleus and mediodorsal nucleus: damage to these (e.g., in Wernicke-Korsakoff syndrome affecting mammillothalamic tract) causes profound anterograde amnesia
(f) Gating and Filtering
- The thalamus does not simply relay signals - it acts as a gatekeeper, filtering and modulating what reaches the cortex depending on the behavioral state (sleep vs. wakefulness, attention, arousal)
- During deep sleep, reticular nucleus-mediated inhibition produces thalamic spindles (as seen on EEG)
(g) Topographic Organization
All specific relay pathways maintain precise somatotopic / tonotopic / retinotopic maps through the thalamus to the cortex, ensuring spatial fidelity of sensory information.
6. NOTE ON THALAMIC SYNDROME (Dejerine-Roussy Syndrome)
(Sources: Harrison's Principles of Internal Medicine 22nd Ed.; Localization in Clinical Neurology 8th Ed.; Kandel: Principles of Neural Science 6th Ed.)
Definition
Thalamic syndrome, first described by Joseph Dejerine and Gustave Roussy in 1906, is a clinical syndrome resulting from a lesion (most commonly an ischemic infarct) in the lateral thalamus - specifically the ventroposterior nuclei (VPL/VPM) and the thalamogeniculate territory supplied by branches of the posterior cerebral artery.
Cause
- Most common cause: ischemic stroke in the thalamogeniculate (lateral thalamic) territory - branches from the P2 segment of the posterior cerebral artery
- Less common: thalamic hemorrhage, tumor, demyelination
Clinical Features (All Contralateral to the Lesion Side)
-
Contralateral hemisensory loss (hemianesthesia) - all modalities affected: touch, pain, temperature, vibration, proprioception. The sensory loss may stop abruptly at the midline ("thalamic midline split")
-
Transient contralateral hemiparesis - mild and usually short-lived (due to involvement of corticospinal fibers in adjacent internal capsule)
-
Hemiataxia - contralateral cerebellar-type incoordination (involvement of dentatorubrothalamic tract)
-
Thalamic pain (central post-stroke pain) - the most characteristic feature:
- Appears at the time of injury or, more typically, weeks to months later as sensory loss begins to improve
- Described as spontaneous, burning, agonizing, searing pain over the entire contralateral half of the body
- Allodynia - normally non-painful stimuli (e.g., light touch, cold) provoke intense pain
- Hyperpathia - exaggerated and prolonged pain response to any stimulus
- Dysesthesias - unpleasant, abnormal sensations in the affected areas
- Pain is persistent and responds poorly to conventional analgesics
- The phenomenon of pain with reduced sensation is called "anesthesia dolorosa" (painful anesthesia)
- Prolonged latency between stimulus and pain perception suggests polysynaptic pathways are involved
-
Choreoathetoid movements - involuntary writhing movements of the contralateral limbs (due to involvement of VL nucleus/subthalamic connections)
-
"Thalamic hand" - abnormal athetoid posture of the contralateral hand
-
Disequilibrium ("thalamic astasia") - impaired balance and gait
-
Homonymous hemianopia - if there is simultaneous involvement of the optic radiation or medial occipital cortex
Pathophysiology of Thalamic Pain
- Destruction of VPL/VPM causes loss of normal inhibitory gating of pain signals
- The medial thalamic nuclei, which project to the limbic system (anterior cingulate cortex), become disinhibited
- This results in abnormal, unregulated activation of affective pain pathways
- Metabolic imaging shows enhanced activation of somatosensory cortex upon stimulation in these patients
Management
Thalamic pain is notoriously difficult to treat:
- Tricyclic antidepressants (amitriptyline) - first line
- Anticonvulsants (gabapentin, pregabalin, carbamazepine)
- Opioids - limited efficacy
- Deep brain stimulation (DBS) of the periaqueductal gray or thalamus - in refractory cases
- Motor cortex stimulation - shows some benefit in selected patients
7. SUMMARY TABLE
| Nucleus | Input | Output | Function |
|---|---|---|---|
| VPL | Medial lemniscus, STT (body) | Somatosensory cortex | Body sensation |
| VPM | Trigeminal tract (face) | Somatosensory cortex | Face sensation, taste |
| LGN | Optic tract | Visual cortex | Vision |
| MGN | Inferior colliculus | Auditory cortex | Hearing |
| VL | Cerebellum | Motor cortex | Voluntary movement |
| VA | Basal ganglia | Premotor cortex | Movement via BG |
| Anterior | Mammillary bodies | Cingulate cortex | Memory/emotion (Papez) |
| MD | Amygdala, hypothalamus | Prefrontal cortex | Emotion/personality |
| Pulvinar | Superior colliculus | Association cortex | Sensory integration |
| Intralaminar | Reticular formation | Widespread cortex | Arousal |
| Reticular | Thalamus + cortex | Thalamus only | Gating/inhibition |
Key Sources:
- Neuroanatomy through Clinical Cases, 3rd Ed. - Ch. 7 (Table 7.3, Figure 7.6)
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry - Table 1.2-3 (Connections of Thalamic Nuclei)
- Harrison's Principles of Internal Medicine, 22nd Ed. - Dejerine-Roussy syndrome
- Localization in Clinical Neurology, 8th Ed. - Thalamic infarction syndromes, thalamic pain
- Kandel: Principles of Neural Science, 6th Ed. - Thalamic relay of nociception and thalamic pain syndrome
This is a shared conversation. Sign in to Orris to start your own chat.