Portal hypertension.causes,clinical features and management.TIPSS
Reading File
Finding Sources
Searching PubMed
"portal hypertension" AND "TIPS" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Searching Images
portal hypertension pathophysiology diagram varices
Searching Images
TIPS transjugular intrahepatic portosystemic shunt procedure stent placement
I now have all the material needed for a comprehensive answer. Let me compile it.
Portal Hypertension: Causes, Clinical Features, and Management (including TIPSS)
Definition
Portal hypertension is defined as a portal venous pressure gradient (hepatic venous pressure gradient, HVPG) >5–7 mmHg. Clinically significant portal hypertension is present when HVPG exceeds 10 mmHg; varices develop and bleed when HVPG exceeds 12 mmHg.
The HVPG = Wedged Hepatic Venous Pressure (WHVP) − Free Hepatic Venous Pressure (FHVP).
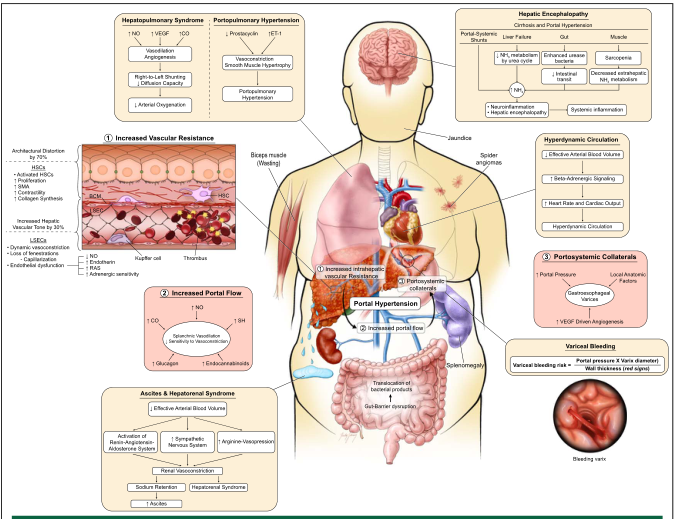
Pathophysiology
Portal hypertension arises from two interacting mechanisms:
- Increased intrahepatic resistance — architectural distortion from fibrosis/cirrhosis (mechanical component ~70%) plus dynamic hepatic stellate cell contraction and sinusoidal endothelial dysfunction (functional component ~30%)
- Increased portal venous inflow — splanchnic arterial vasodilation (driven by excess nitric oxide, glucagon, endocannabinoids) → hyperdynamic circulation, expanded blood volume, sodium and water retention
Causes / Classification
Classified by the site of increased resistance to portal blood flow:
| Location | Subcategory | Causes |
|---|---|---|
| Prehepatic | — | Portal vein thrombosis, splenic vein thrombosis, congenital portal vein thrombosis, arteriovenous fistula (excessive inflow), splenomegaly |
| Intrahepatic — Presinusoidal | Extrahepatic | Schistosomiasis (world's most common cause globally) |
| Intrahepatic | Primary biliary cholangitis, congenital hepatic fibrosis, nodular regenerative hyperplasia, idiopathic portal fibrosis, sarcoidosis, myeloproliferative disorders, graft-versus-host disease | |
| Intrahepatic — Sinusoidal | — | Cirrhosis (most common in North America/Europe), viral hepatitis, alcohol-associated liver disease, autoimmune hepatitis, NAFLD/NASH, primary sclerosing cholangitis, metabolic disorders (hemochromatosis, Wilson's disease) |
| Intrahepatic — Postsinusoidal | — | Hepatic veno-occlusive disease (sinusoidal obstruction syndrome) |
| Posthepatic | — | Budd-Chiari syndrome (hepatic vein thrombosis), IVC webs/thrombosis, congestive heart failure, constrictive pericarditis, tricuspid valve disease |
Key point: In North America, cirrhosis accounts for ~90% of cases. Worldwide, schistosomiasis and portal vein thrombosis are important additional causes. Alcohol-associated disease may elevate portal pressure even before cirrhosis develops.
— Current Surgical Therapy 14e, p. 455; Schwartz's Principles of Surgery 11e, p. 1393–1394
Clinical Features
Consequences of raised portal pressure
| Feature | Mechanism |
|---|---|
| Gastroesophageal varices | Portosystemic collaterals open; fed mainly by the left gastric (coronary) vein. ~50% of cirrhotics develop varices; ~1/3 bleed within 1 year |
| Gastric varices | ~25% of patients; GOV1 most common (~70%). Isolated gastric varices (IGV) suggest splenic vein thrombosis |
| Anorectal varices | ~45% of cirrhotics; must be distinguished from hemorrhoids (which are not in communication with the portal system) |
| Splenomegaly & hypersplenism | Congestion of splenic vessels → pancytopenia (thrombocytopenia, leukopenia, anemia) |
| Ascites | Portal hypertension + hepatocyte dysfunction → splanchnic vasodilation → RAAS/SNS activation → Na⁺ and water retention |
| Hepatic encephalopathy | Portosystemic shunting → ammonia bypass of liver |
| Caput medusae | Recanalisation and dilatation of the umbilical vein → visible abdominal wall collaterals |
| Hepatorenal syndrome | Effective arterial hypovolemia → renal vasoconstriction |
| Hepatopulmonary syndrome | Intrapulmonary vascular dilation → hypoxaemia |
| Portopulmonary hypertension | Sustained increased pulmonary vascular resistance |
| Spontaneous bacterial peritonitis (SBP) | Bacterial translocation in ascitic fluid |
| Hyperdynamic circulation | ↑ cardiac output, ↓ SVR, tachycardia |
Signs of chronic liver disease (usually co-present)
- Jaundice, spider naevi, palmar erythema, leukonychia
- Gynaecomastia, testicular atrophy
- Muscle wasting (sarcopenia), asterixis (hepatic encephalopathy)
Variceal hemorrhage: mortality ranges from 5% (Child A) to >68% (Child C). — Current Surgical Therapy 14e, p. 455
Measurement
- HVPG via hepatic vein balloon catheterisation — gold standard
- Non-invasive: liver stiffness (transient elastography), platelet count/spleen size ratios
- Endoscopy: gold standard for variceal detection and grading
- Doppler ultrasound: assesses portal vein flow direction and velocity, splenomegaly, ascites
Management
1. Treat the underlying cause
Where reversible: antiviral therapy (hepatitis B/C), abstinence (alcohol), anticoagulation (portal vein thrombosis, Budd-Chiari)
2. Primary prevention of variceal bleeding (no prior bleed)
- Non-selective beta-blockers (NSBBs): propranolol, nadolol — reduce heart rate by 25% or to 55 bpm; reduce HVPG; also reduce risk of ascites and SBP
- Endoscopic variceal band ligation (EVL): for medium-to-large varices; preferred over sclerotherapy for primary prophylaxis
- Carvedilol (non-selective BB + anti-alpha1) increasingly used
3. Acute variceal hemorrhage
- Resuscitation: cautious transfusion (target Hb 7–8 g/dL; over-transfusion raises portal pressure)
- Vasoactive agents: octreotide, somatostatin, terlipressin (or vasopressin + nitroglycerin) — started immediately, continued 3–5 days
- Endoscopy within 12 hours: EVL first-line; sclerotherapy when visualization is difficult
- Antibiotic prophylaxis: short-course (norfloxacin or ceftriaxone) — reduces risk of SBP and mortality
- Balloon tamponade (Sengstaken-Blakemore or Minnesota tube): temporary bridge (max 24h), risk of aspiration and esophageal necrosis — only when endoscopy unavailable or fails
- TIPSS: indicated in 10–20% of cases refractory to medical/endoscopic therapy; success rate >90%
4. Secondary prevention of rebleeding
- NSBBs + EVL combination
- TIPSS for refractory or high-risk patients
5. Management of ascites
- Low-sodium diet (<88 mmol/day)
- Diuretics: spironolactone ± furosemide
- Large-volume paracentesis with IV albumin for refractory ascites
- TIPSS: effective for refractory ascites
6. Liver transplantation
Gold standard — curative for both underlying liver dysfunction and all complications of portal hypertension.
TIPSS (Transjugular Intrahepatic Portosystemic Shunt)
What it is
A catheter-based, endovascular procedure that creates a side-to-side portocaval shunt through the hepatic parenchyma, functionally lowering portal pressure.
Procedure
- Access the right internal jugular vein → advance catheter under fluoroscopic guidance into a hepatic venous branch
- Pass a needle through the hepatic vein wall into the portal vein
- Dilate the intrahepatic tract
- Deploy a PTFE-covered stent across the tract
- Target post-procedure HVPG <12 mmHg

Indications
- Acute variceal hemorrhage refractory to medical/endoscopic therapy
- Secondary prevention of variceal rebleeding (when endoscopic/pharmacological therapy fails)
- Refractory ascites (not responsive to diuretics)
- High-risk variceal bleeding: acute TIPSS after endoscopy in patients with HVPG >20 mmHg reduces re-bleeding
- Budd-Chiari syndrome: bridge to transplantation
- Ectopic variceal bleeding, hepatic hydrothorax, hepatorenal syndrome
Contraindications
| Absolute | Relative |
|---|---|
| Congestive heart failure | MELD score >18 |
| Moderate-severe pulmonary hypertension | Portal vein thrombosis (may still be feasible) |
| Tricuspid regurgitation | Hepatocellular carcinoma |
| Severe liver failure (advanced Child C) | Pre-existing hepatic encephalopathy |
| Uncontrolled systemic infection | Polycystic liver disease |
Advantages
- Effective in >90% of cases for variceal control
- Reduces ascites production
- Better portal decompression than medical therapy alone
- Can be used as a bridge to liver transplantation; removed with the explanted liver at transplant
- Improved patency with PTFE stents (1-year patency ~93%, 3-year ~75%)
Complications
| Complication | Notes |
|---|---|
| Hepatic encephalopathy | ~20–30% risk; due to portosystemic shunting bypassing hepatic clearance of ammonia. Managed with lactulose, rifaximin |
| Stent dysfunction (stenosis/thrombosis) | Requires regular Doppler ultrasound surveillance; up to 80% need ≥1 post-procedural intervention |
| Right heart failure | Increased venous return overwhelms compensatory capacity |
| Intra-abdominal hemorrhage | ~1–2% (major complication) |
| Contrast-induced nephropathy | |
| Biliary injury / biloma | Stent may traverse biliary radicles |
| Haemolytic anaemia | |
| Sepsis |
Monitoring after TIPSS
- Regular Doppler ultrasound to assess shunt patency (flow velocity, direction)
- Hepatic encephalopathy assessment
- Repeat HVPG measurement if clinically indicated
- Rebleeding in 5–15% occurs mainly in the context of stent occlusion
Surgical Shunts (for context)
When TIPSS is not feasible, surgical shunts provide an alternative:
- Non-selective (total) shunts: portocaval (end-to-side or side-to-side), mesocaval — decompress varices effectively but high encephalopathy risk
- Selective shunt — Distal Splenorenal Shunt of Warren: decompresses gastroesophageal varices via retrograde splenic flow while preserving mesenteric portal perfusion. >90% effective for variceal control; low encephalopathy; contraindicated in massive ascites (does not lower sinusoidal pressure)
- Mesoatrial shunt: historical — used when IVC is obstructed (e.g., Budd-Chiari with IVC thrombosis)
Surgically placed shunts require ligation or revision at time of liver transplantation — a disadvantage over TIPSS.
Recent Evidence (PubMed, last 2 years)
- TIPSS for ectopic variceal bleeding — Systematic Review (PMID 38935315): supports TIPSS as effective management for ectopic (non-oesophageal) variceal bleeding
- TIPSS in hepatocellular carcinoma — Meta-analysis (PMID 39126599): demonstrates efficacy and safety in HCC patients with portal hypertension
- Cardiovascular risk and cardiac decompensation post-TIPSS (PMID 40741106, 2025): identifies predictors of cardiac decompensation — underscores importance of pre-procedural cardiac assessment
Sources: Current Surgical Therapy 14e, pp. 455–458; Schwartz's Principles of Surgery 11e, pp. 1393–1394; Sleisenger & Fordtran's Gastrointestinal and Liver Disease, Chapter 92; Miller's Anesthesia 10e, pp. 1540–1541
This is a shared conversation. Sign in to Orris to start your own chat.