Abdominal Peritoneum
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Abdominal Peritoneum
Definition and Structure
The peritoneum is the largest and most complex serous membrane in the human body. Its surface area (~2 m²) nearly equals that of the skin. It consists of a single layer of flattened polyhedral cells called mesothelium, resting on a thin layer of fibroelastic tissue. Beneath the mesothelium lies a rich network of lymphatic vessels and capillary blood vessels through which all absorption and exudation occur.
The abdominal wall layers deep to the muscles are, from outside in:
- Transversalis fascia
- Extraperitoneal (preperitoneal) fascia/fat
- Parietal peritoneum (innermost lining)
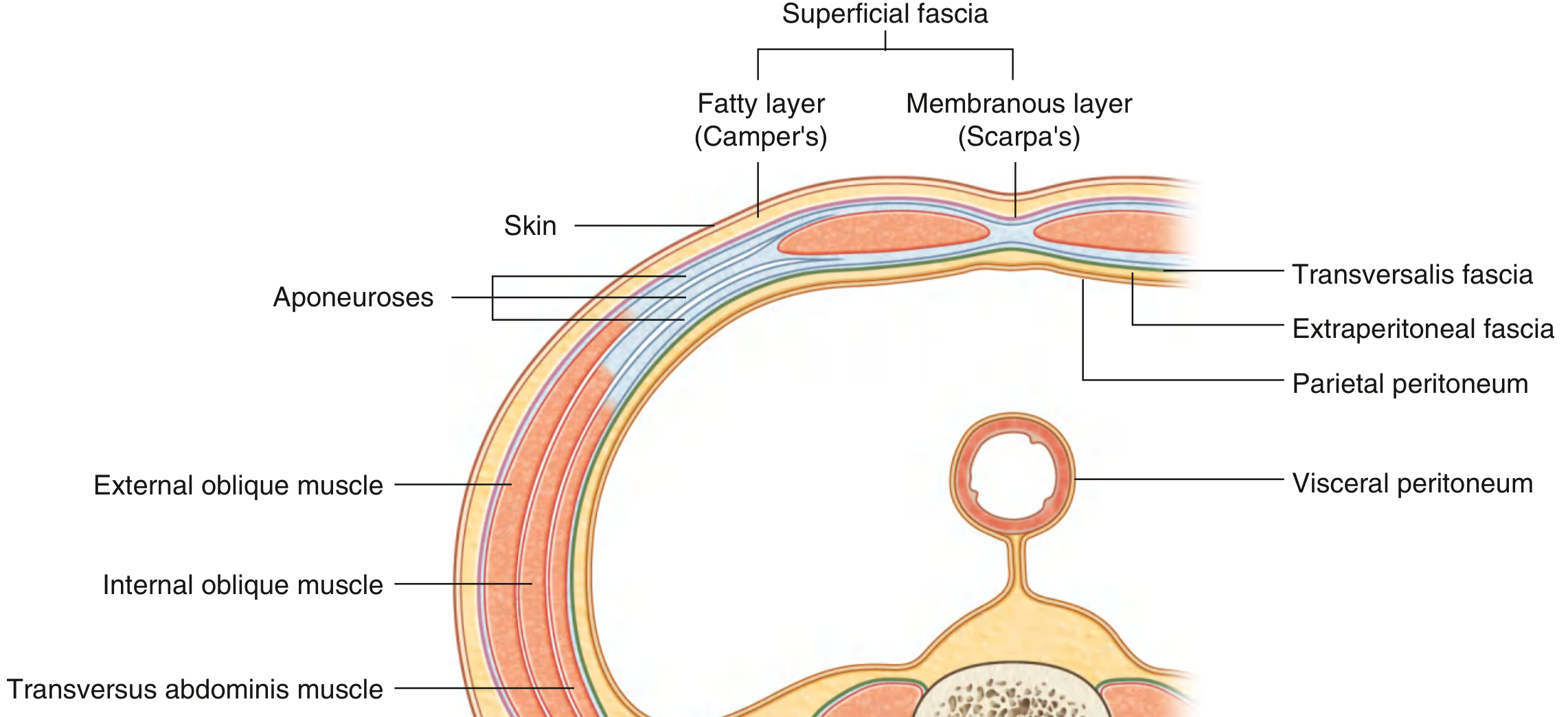
Fig: Transverse section showing abdominal wall layers - note the parietal peritoneum as the innermost layer, and visceral peritoneum wrapping the gut tube. (Gray's Anatomy for Students)
Two Layers of Peritoneum
| Layer | Location | Nerve Supply | Pain Character |
|---|---|---|---|
| Parietal peritoneum | Lines the abdominal and pelvic walls | Somatic afferents (T7-L1 spinal nerves) | Severe, well-localized pain |
| Visceral peritoneum | Covers the abdominal viscera | Visceral afferents (autonomic) | Poorly localized, referred to midline |
The Peritoneal Cavity
The parietal peritoneum forms a continuous sac. This sac is:
- Closed in men
- Has two openings in women - where the uterine tubes open, providing a pathway to the exterior (a common route for pelvic infection to ascend into the peritoneal cavity)
In health, only a few millilitres of pale yellow, slightly viscid peritoneal fluid are present. This fluid contains lymphocytes and other leukocytes and serves to lubricate the viscera, facilitating smooth movement and peristalsis.
Greater Sac vs. Lesser Sac (Omental Bursa)
The greater and lesser omentum divide the peritoneal cavity into two compartments:
- Greater sac: The main peritoneal space
- Lesser sac (omental bursa): Located behind the lesser and greater omentum, stomach, and transverse colon. Communicates with the greater sac through the omental (epiploic) foramen of Winslow
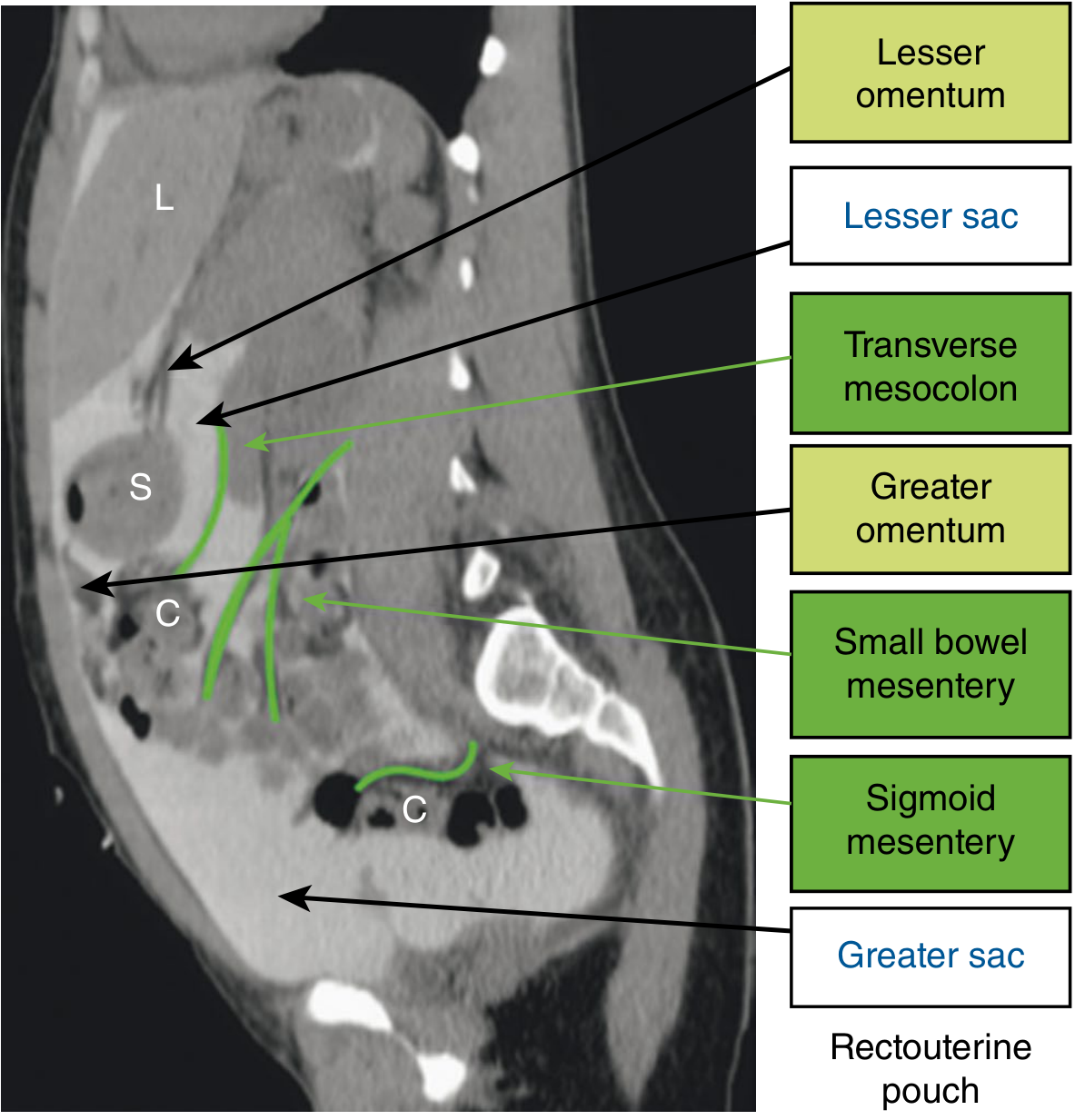
Fig: CT peritoneogram (sagittal) illustrating the mesenteries, greater and lesser sacs, and omenta. L = Liver, S = Stomach, C = Colon. (Sabiston Textbook of Surgery)
Intraperitoneal vs. Retroperitoneal Organs
Abdominal viscera are classified based on their relationship to the peritoneum:
- Intraperitoneal - suspended in the cavity by mesenteries (e.g., stomach, jejunum, ileum, transverse colon, sigmoid colon, spleen, liver)
- Retroperitoneal - outside the peritoneal cavity, covered by peritoneum on only one surface (e.g., kidneys, ureters, aorta, ascending and descending colon, duodenum 2nd-4th parts, pancreas, rectum)
A further subdivision:
- Preperitoneal: Between the anterior abdominal wall muscles and the peritoneum (e.g., preperitoneal fat in the inguinal region)
- Retroperitoneal: Between the peritoneum and the posterior abdominal wall
Peritoneal Folds
Throughout the peritoneal cavity, folds of peritoneum connect organs to each other or to the abdominal wall. They develop from the embryonic dorsal and ventral mesenteries. There are three types:
1. Omenta
Two-layered peritoneal folds passing from the stomach/duodenum to other viscera:
Greater Omentum (from dorsal mesentery):
- A large, apron-like fold attached to the greater curvature of the stomach and first part of the duodenum
- Drapes inferiorly over the transverse colon and loops of small bowel
- Turns posteriorly, ascending to fuse with the superior surface of the transverse colon and anterior layer of the transverse mesocolon
- Always contains fat (which can become substantial); carries the right and left gastro-omental vessels
- Clinically known as the "policeman of the abdomen" - it migrates to inflamed areas, walling off infection/inflammation
- A major site for transcoelomic metastatic spread (especially ovarian carcinoma → "omental cake")
Lesser Omentum (from ventral mesentery):
- Extends from the lesser curvature of the stomach and first part of the duodenum to the inferior surface of the liver
- Divided into:
- Hepatogastric ligament (medial part - between stomach and liver)
- Hepatoduodenal ligament (lateral part - between duodenum and liver; free right border forms the anterior boundary of the omental foramen)
- The hepatoduodenal ligament encloses three vital structures: portal vein, hepatic artery proper, and bile duct (Pringle's manoeuvre compresses this)
2. Mesenteries
Double-layered peritoneal folds attaching viscera to the posterior abdominal wall; carry vessels, nerves, and lymphatics:
| Mesentery | Associated Organ | Attachment |
|---|---|---|
| Mesentery (proper) | Jejunum and ileum | Duodenojejunal flexure → ileocaecal junction (~15 cm root, oblique) |
| Transverse mesocolon | Transverse colon | Anterior surface of pancreas/posterior abdominal wall |
| Sigmoid mesocolon | Sigmoid colon | Posterior abdominal/pelvic wall |
All three are derivatives of the dorsal mesentery.
3. Peritoneal Ligaments
Folds connecting organs to the abdominal wall or to each other (e.g., falciform ligament connecting liver to anterior wall, coronary ligament, splenorenal ligament, gastrosplenic ligament).
Peritoneal Fluid Circulation
Peritoneal fluid circulates in a clockwise orientation. During expiration, intra-abdominal pressure falls and fluid travels upward toward the diaphragm. Particulate matter and bacteria are absorbed within minutes into the lymphatic network via "pores" in the diaphragmatic peritoneum. This circulation pattern explains why abscesses can develop at sites remote from the primary disease. The most common collection sites are:
- Pelvis (rectovesical/recto-uterine pouch - pouch of Douglas) - gravity when upright
- Right subphrenic/subhepatic space (pouch of Morrison/hepatorenal fossa) - gravity when supine
- Right paracolic gutter
Innervation of the Peritoneum
- Parietal peritoneum of the abdominal wall: T7-T12 and L1 spinal nerves (somatic) - pain is well-localised to the affected quadrant; stimulation causes protective guarding and rigidity
- Visceral peritoneum: Visceral afferents via autonomic nerves - pain is poorly localised, typically referred to the midline, described as dull/crampy
- The pelvic parietal peritoneum is innervated by obturator nerve branches and sacral nerves
Functions of the Peritoneum
In health:
- Visceral lubrication (frictionless movement)
- Fluid and particulate absorption
- Immunological surveillance
In disease:
- Pain perception (primarily parietal component)
- Inflammatory and immune responses
- Fibrinolytic activity
- Can produce large volumes of fluid (ascites) or inflammatory exudate (peritonitis)
Clinical Relevance
Peritonitis - inflammation of the peritoneum; classified as localised or diffuse. Causes include:
- Gastrointestinal perforation (peptic ulcer, appendix, diverticulum)
- Transmural translocation (pancreatitis, ischaemic bowel, primary bacterial peritonitis)
- Exogenous contamination (trauma, drains, peritoneal dialysis)
- Female genital tract infection (pelvic inflammatory disease)
- Haematogenous spread (rare)
Peritoneal dialysis: The large vascular surface area (~2 m²) makes the peritoneum an effective dialysis membrane.
Peritoneal metastases: Direct transcoelomic spread is common from GI and gynaecological cancers; fluid circulation determines implant distribution (pelvis, right paracolic gutter, hepatorenal fossa most affected).
Sources: Gray's Anatomy for Students (9780323934237); Bailey and Love's Short Practice of Surgery, 28th ed. (9780367548117); Sabiston Textbook of Surgery, 21st ed. (9780443124341); Schwartz's Principles of Surgery, 11th ed. (9781259835346)
This is a shared conversation. Sign in to Orris to start your own chat.