Oral pathology
Reading File
Asking for Preferences
Asking for Preferences
Finding Sources
Searching PubMed
"odontogenic cysts"[MeSH Terms] AND classification
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content to write a detailed, well-structured answer. Let me compile it all.
Odontogenic Cysts - Comprehensive Overview
Classification
Odontogenic cysts arise from remnants of the tooth-forming apparatus. They are classified into two broad categories based on pathogenesis:
WHO Classification (Table 16.3 - Robbins; Table 25.3 - Scott-Brown's)
| Category | Cyst Type | Subtype |
|---|---|---|
| Inflammatory | Radicular (periapical/dental) cyst | Apical, lateral, residual |
| Inflammatory | Paradental (inflammatory collateral) cyst | - |
| Developmental | Dentigerous (follicular) cyst | Eruption cyst |
| Developmental | Odontogenic keratocyst (OKC) | - |
| Developmental | Gingival cyst of adults | - |
| Developmental | Lateral periodontal cyst | Botryoid variant |
| Developmental | Glandular odontogenic (sialo-odontogenic) cyst | - |
| Developmental | Calcifying odontogenic cyst (Gorlin cyst) | - |
| Developmental | Orthokeratinized odontogenic cyst | - |
Epithelial Origins
Three distinct epithelial remnants persist after odontogenesis and give rise to specific cysts:
- Rests of Malassez - from fragmentation of Hertwig's root sheath at root completion → Radicular cysts
- Reduced enamel epithelium - fusion of inner/outer enamel epithelia covering the unerupted crown → Dentigerous, eruption, and paradental cysts
- Rests (glands) of Serres - remnants of the dental lamina → Lateral periodontal, gingival, and keratocystic odontogenic tumour (OKC)
(Scott-Brown's Otorhinolaryngology, p. 443-444)
Individual Cysts in Detail
1. Radicular Cyst (Periapical / Dental Cyst)
- Most common jaw cyst overall
- Pathogenesis: Pulpitis (usually from caries or trauma) → pulp necrosis → periapical inflammation → stimulation of Rests of Malassez → epithelial proliferation → cyst formation
- Location: Root apex of a non-vital tooth (or lateral root canal in lateral variant; residual cyst remains after tooth extraction)
- Radiology: Unilocular radiolucency at tooth apex, with a radiopaque rim
- Treatment: Root canal treatment (enucleation if residual cyst remains)
- Note: The term "periapical granuloma" is still used despite the fact that the lesion does not show true granulomatous inflammation - it is actually epithelialized in true radicular cysts (Robbins, p. 687)
2. Dentigerous (Follicular) Cyst
- Second most common jaw cyst (accounts for ~15-18% of jaw cysts)
- Pathogenesis: Expansion of the dental follicle around the crown of an unerupted tooth; attached at the cemento-enamel junction (CEJ)
- Commonly associated teeth (in decreasing frequency): mandibular third molars ("wisdom teeth"), maxillary canines, mandibular second premolars, maxillary third molars
- Peak age: 2nd-3rd decades
- Clinical features: Often asymptomatic, found incidentally on X-ray for a missing tooth; may cause swelling, tooth displacement, secondary infection. Can reach up to 5 cm diameter.
- Radiology: Unilocular radiolucency attached to/surrounding the CEJ of an unerupted tooth
- Histology: Thin non-keratinized squamous or cuboidal/columnar lining; focal keratinization and mucous/ciliated cells possible via metaplasia
- Complications: Root resorption of adjacent teeth; transformation to ameloblastoma is a recognized (though rare) complication - ameloblastomas can form in the cyst wall
- Differential diagnosis for larger lesions: OKC, unicystic ameloblastoma
- Eruption cyst variant: Superficially located dentigerous cyst; presents as a bluish gum swelling over an erupting tooth, especially in children; cyclosporin therapy is a predisposing factor
(Scott-Brown's, pp. 444-445; Robbins, p. 686)
3. Odontogenic Keratocyst (OKC) / Keratocystic Odontogenic Tumour (KCOT)
- Derived from: Rests of Serres (dental lamina remnants)
- Important: Previously reclassified by the WHO (2005) as "Keratocystic Odontogenic Tumour (KCOT)" due to aggressive behavior; the 2017 WHO classification reverted to OKC terminology
- Location: Most often in the posterior mandible (angle/ramus region); can occur in a dentigerous relationship or independent of any tooth
- Clinical behavior: Locally aggressive; recurrence rates for inadequately removed lesions can be as high as 60%. About 80% of lesions are solitary.
- Gorlin syndrome (Nevoid Basal Cell Carcinoma Syndrome): Multiple OKCs = strong indicator; caused by germline loss-of-function mutations in PTCH (Patched tumor suppressor gene). Patients with multiple cysts must be evaluated for this syndrome.
- EGFR: Recent studies show EGFR signaling plays a role in OKC behavior and growth (PMID 37314601)
- Radiology: Unilocular or multilocular radiolucency; can mimic dentigerous cyst when associated with a tooth root; may expand along the medullary cavity with little cortical expansion (characteristic)
- Histology: Thin, uniform parakeratinized stratified squamous epithelium (typically 6-8 cell layers thick); flat epithelial-connective tissue interface; prominent palisaded basal cells with hyperchromatic nuclei ("tombstone" appearance); corrugated parakeratotic surface
- Treatment: Excision; curettage and partial excision result in high recurrence. Some advocate marsupialization followed by enucleation. Peripheral ostectomy and Carnoy's solution used adjunctively.
(Robbins, p. 686-688; Scott-Brown's, p. 445; K.J. Lee's Essential Otolaryngology)
4. Lateral Periodontal Cyst
- Derived from Rests of Serres
- Located lateral to the root of a vital tooth (distinguishes it from lateral radicular cyst of non-vital tooth)
- Botryoid variant: Multilocular / polycystic form; higher recurrence rate
5. Glandular Odontogenic Cyst (Sialo-Odontogenic Cyst)
- Rare but locally aggressive developmental cyst
- Contains gland-like structures (mucous cells, ciliated cells) within its lining - hence "glandular"
- Higher recurrence rate; must be distinguished from central mucoepidermoid carcinoma
6. Calcifying Odontogenic Cyst (Gorlin Cyst / CCOT)
- Contains "ghost cells" - keratinized cells lacking nuclei
- May contain calcifications
- Some cases progress to "dentinogenic ghost cell tumor" (solid variant)
- Recent reviews support reclassification into cystic vs. solid forms (PMID 39217025)
7. Orthokeratinized Odontogenic Cyst
- Distinct from OKC; lining shows orthokeratin (not parakeratin)
- Less aggressive than OKC; lower recurrence
- Not associated with Gorlin syndrome
- Important to distinguish histologically from OKC due to different prognosis
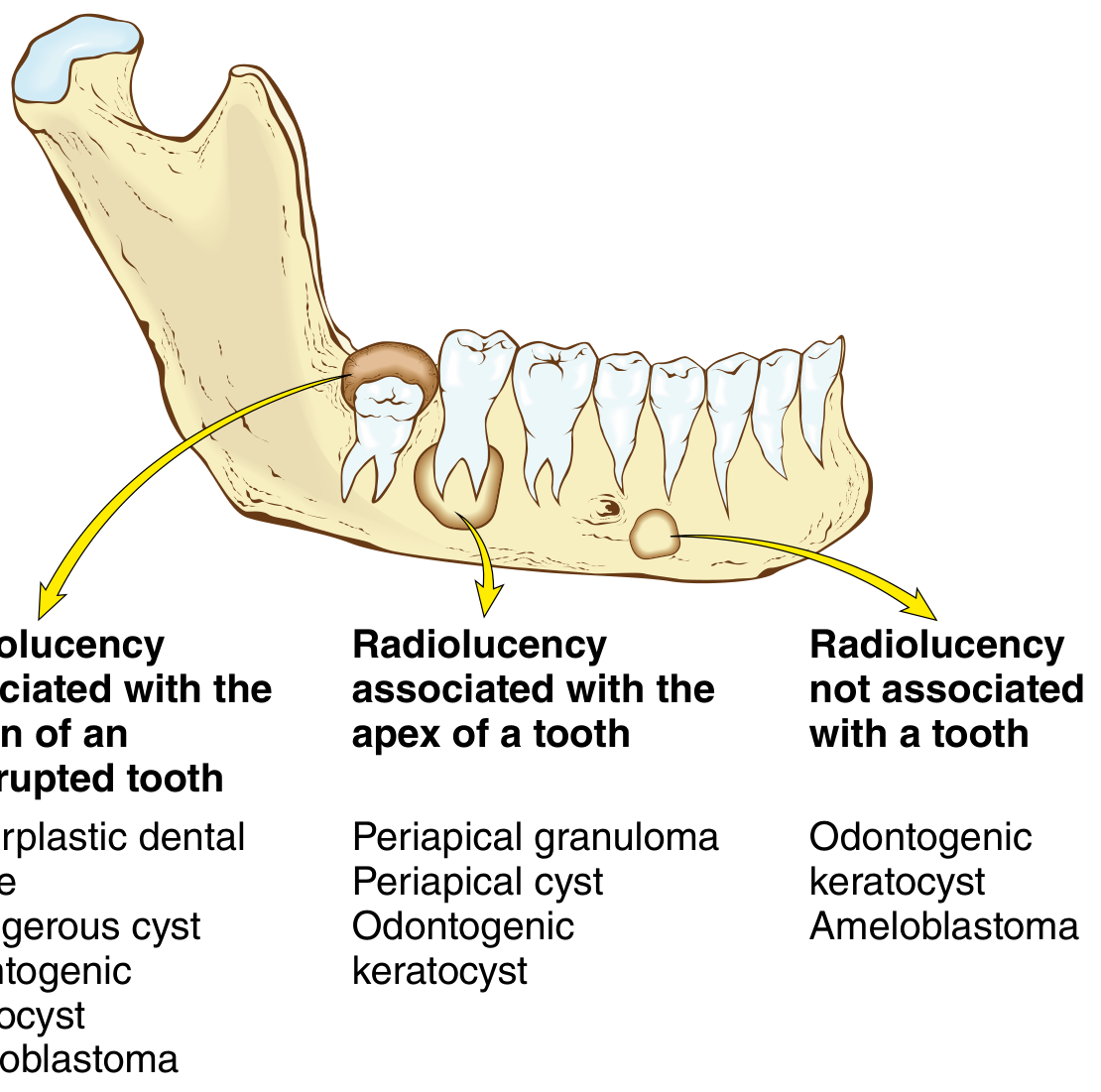
Radiology Summary - Differential Approach
| Radiolucency Pattern | Consider |
|---|---|
| Associated with crown of unerupted tooth | Dentigerous cyst, OKC, hyperplastic dental follicle, unicystic ameloblastoma |
| Associated with apex of a (non-vital) tooth | Radicular/periapical cyst, periapical granuloma, OKC |
| Not associated with a tooth | OKC, ameloblastoma, lateral periodontal cyst |
(Robbins, Fig. 16.8)
Key Distinguishing Features at a Glance
| Feature | Radicular | Dentigerous | OKC |
|---|---|---|---|
| Origin | Rests of Malassez | Reduced enamel epithelium | Rests of Serres |
| Category | Inflammatory | Developmental | Developmental |
| Tooth vitality | Non-vital | Unerupted tooth | Any (or independent) |
| Location | Apex | CEJ of crown | Posterior mandible |
| Recurrence | Low | Low | High (up to 60%) |
| Histology | Non-keratinized lining | Thin cuboidal/squamous | Parakeratinized, uniform, palisaded basal layer |
| Gorlin syndrome | No | No | Yes (multiple OKCs) |
Recent Evidence
- A 2024 systematic review and meta-analysis (PMID 38530559) evaluated machine learning accuracy in diagnosing odontogenic cysts and tumors - showing promising diagnostic performance for AI-assisted radiographic classification.
- A 2023 review (PMID 37314601) highlights the significance of EGFR investigation in OKC, with EGFR overexpression contributing to the aggressive behavior and recurrence potential of OKC.
- A 2025 review (PMID 39217025) proposes a novel outlook on classification, diagnosis, and management of calcifying odontogenic cysts.
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease (pp. 686-688) | Scott-Brown's Otorhinolaryngology Head & Neck Surgery (pp. 443-450) | K.J. Lee's Essential Otolaryngology | Cummings Otolaryngology Head & Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.