Explain development of eye in full detail along with all clinicals
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive information from multiple textbooks. Let me compile the full detailed response.
Development of the Eye - Full Detail with Clinical Correlates
Sources: Langman's Medical Embryology, The Developing Human (Moore & Persaud), Histology: A Text and Atlas (Ross & Pawlina)
Tissue Origins of the Eye
The eye is derived from four tissue sources:
| Tissue Source | Structures Derived |
|---|---|
| Neuroectoderm of forebrain | Retina (both layers), optic nerve fibers, iris muscles (sphincter & dilator pupillae), iris and ciliary body epithelium |
| Surface ectoderm | Lens, corneal epithelium, conjunctival epithelium, lacrimal gland epithelium, eyelid epidermis |
| Mesoderm | Eye muscles (except iris muscles), vascular and connective tissue of cornea, choroid, sclera, ciliary body |
| Neural crest cells | Corneal endothelium and stroma, ciliary muscles, trabecular network, ciliary body, parts of uveal tract |
Step-by-Step Embryological Development
Day 22 - Optic Grooves (First Sign)
The first indication of eye development appears on day 22 as paired shallow grooves - the optic sulci (optic grooves) - in the neural folds at the cranial end of the embryo, on either side of the forebrain. These are visible even before neural tube closure.
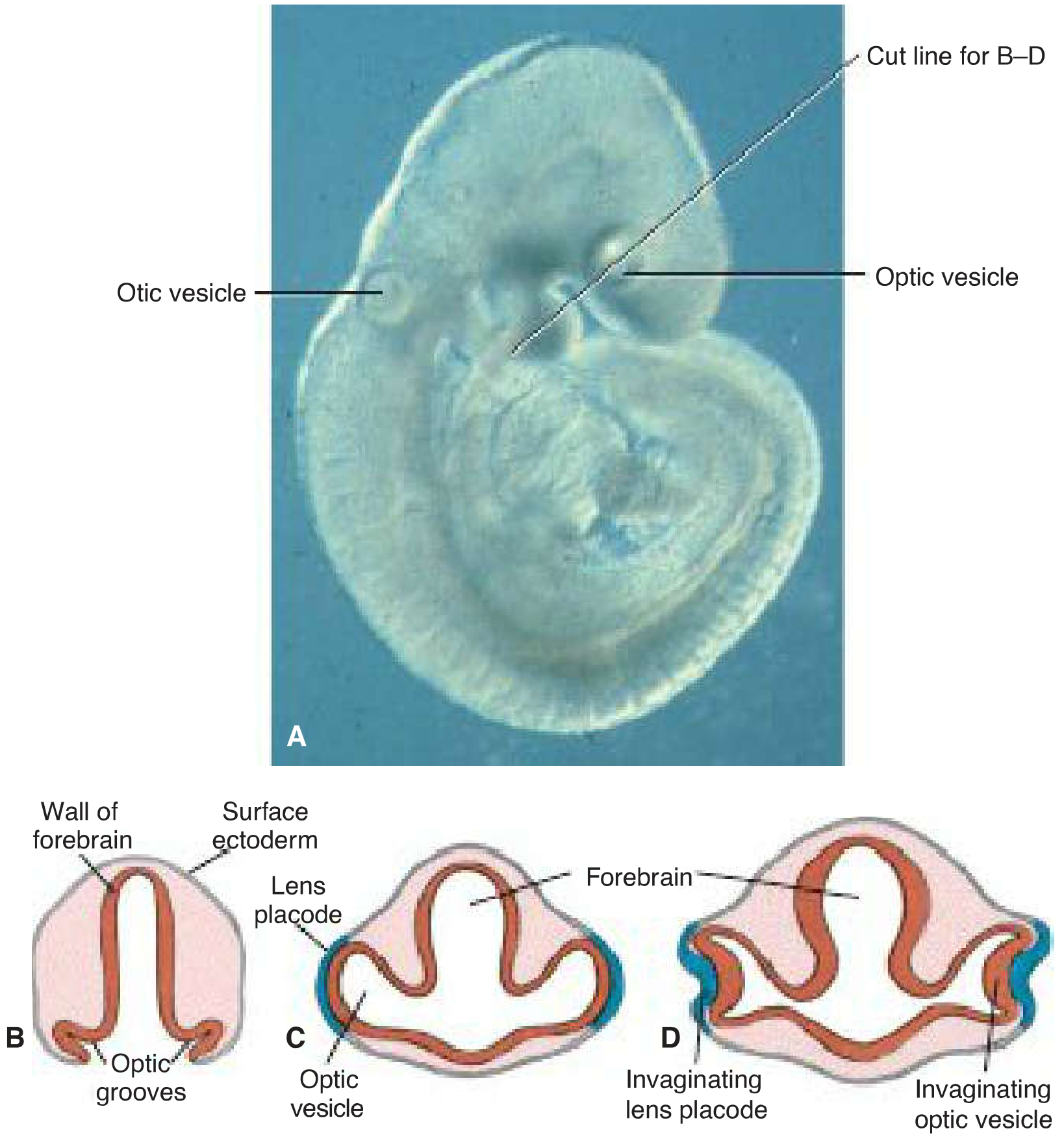
Fig: Early eye development - optic grooves (day 22), optic vesicles (day 28), lens placode contact, and invagination (5mm embryo). (Langman's Medical Embryology)
Week 4 - Optic Vesicles
As the neural tube closes, the optic grooves deepen and evaginate laterally as hollow outpocketings called optic vesicles from the lateral walls of the forebrain (prosencephalon). The connection of each vesicle to the forebrain narrows into the optic stalk. The vesicles grow outward until they contact the overlying surface ectoderm.
Inductive interaction: The optic vesicle induces the overlying surface ectoderm to thicken, forming the lens placode (thickened ectodermal disc). This is a critical epithelial-mesenchymal induction event.
Week 5 - Optic Cup and Lens Vesicle Formation
The optic vesicle invaginates from its center inward, forming the double-walled optic cup. Simultaneously, the lens placode invaginates to form the lens pit, which then closes off as the lens vesicle. By the end of week 5, the lens vesicle detaches completely from the surface ectoderm and sits in the mouth of the optic cup.
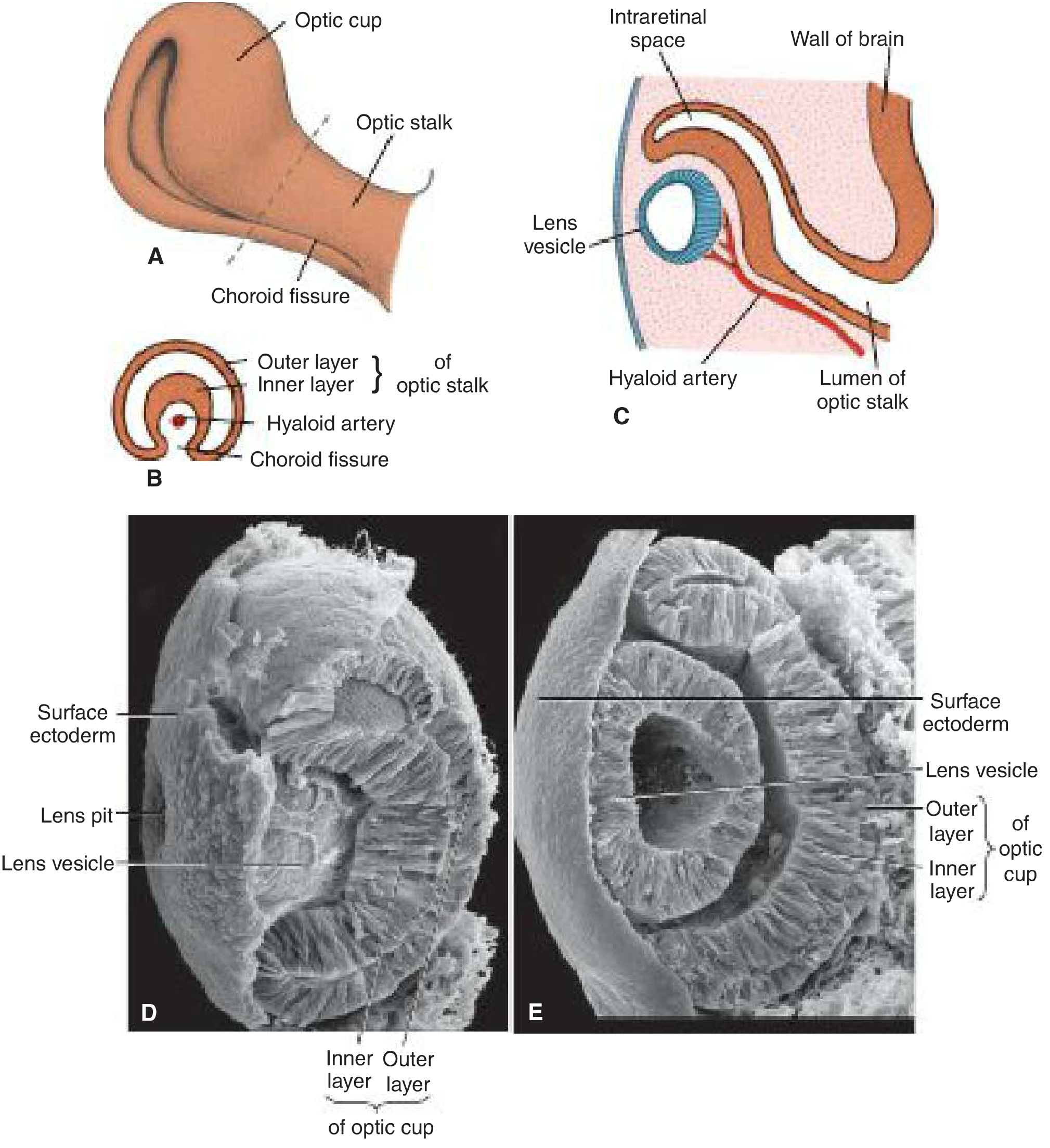
Fig: Ventrolateral view of optic cup and stalk at 6 weeks (A), cross-section showing hyaloid artery in choroid fissure (B,C), and scanning electron micrographs at 6 and 6.5 weeks (D,E). (Langman's)
The two walls of the optic cup:
- Outer layer (thin): becomes the retinal pigment epithelium (RPE). Small pigment granules appear by the end of week 5. Pigmentation begins at the end of the fifth week.
- Inner layer (thick, neural): differentiates into the neural retina (9 layers of the photosensitive retina)
An intraretinal space initially separates the two layers - it is derived from the cavity of the original optic cup and gradually obliterates as the layers appose. The fusion is never truly firm, explaining the anatomical basis of retinal detachment.
The Choroid Fissure (Retinal Fissure)
Invagination is not limited to the center of the cup. It also affects the inferior surface of the optic cup and stalk, creating a groove called the choroid fissure (retinal fissure). This fissure:
- Contains vascular mesenchyme from which the hyaloid artery develops (a branch of the ophthalmic artery)
- Supplies the inner optic cup, lens vesicle, and mesenchyme in the cavity
- Also carries the developing ganglion cell axons (future optic nerve fibers) toward the brain
During the 7th week, the lips of the choroid fissure fuse, enclosing the hyaloid vessels within the primordial optic nerve. The mouth of the optic cup becomes a round opening - the future pupil. Distal portions of the hyaloid vessels degenerate; proximal portions persist as the central artery and vein of the retina.
BMP, SHH, and FGF signaling are all required for proper closure of the retinal fissure.
Development of Individual Ocular Structures
1. Retina
The retina develops from the two walls of the optic cup:
- Outer layer → single layer of pigment epithelium (RPE) - firmly attached to the choroid in postnatal life
- Inner (neural) layer → differentiates into the 9-layer neural retina
The inner layer is divided into:
-
Pars optica retinae (posterior 4/5): contains cells bordering the intraretinal space that differentiate into photoreceptors (rods and cones). The adjacent mantle layer gives rise to neurons and supporting cells - the outer nuclear layer, inner nuclear layer, and ganglion cell layer. The surface contains a fibrous layer with axons converging toward the optic stalk.
- Rods: ~120 million; more sensitive; responsible for night/peripheral vision
- Cones: 6-7 million; detect color; concentrated in the fovea
-
Pars caeca retinae (anterior 1/5): remains one cell layer thick; subdivides into:
- Pars iridica retinae: inner epithelial layer of the iris
- Pars ciliaris retinae: participates in ciliary body formation, marked by pronounced folding
Because the optic vesicle invaginates, the neural retina is inverted: light-sensitive parts of photoreceptors face the RPE, meaning light must traverse most of the retinal thickness before reaching rods and cones.
Retinal precursor cell proliferation is regulated by forkhead transcription factors; Lhx2, Six2, Pax6, and Rax are involved in retinal neurogenesis.
2. Iris
The iris is composed of:
- Outer pigmented layer (from outer layer of optic cup)
- Inner unpigmented layer (from inner layer of optic cup - pars iridica retinae)
- Richly vascularized connective tissue layer (from mesenchyme) containing the pupillary muscles
Sphincter pupillae: circular smooth muscle; derived from the ectoderm of the optic cup rim (unusual - a muscle from ectoderm); innervated by CN III parasympathetics; constricts pupil in bright light.
Dilator pupillae: radially oriented contractile processes of pigmented myoepithelial cells constituting the anterior pigment epithelium of the iris; innervated by sympathetic nerves from the superior cervical ganglion; dilates pupil in dim light.
The region between the optic cup and the overlying surface epithelium is filled by loose mesenchyme from which these muscles form.
3. Ciliary Body
The pars ciliaris retinae is the embryological origin of the inner epithelial lining of the ciliary body. Externally, it is covered by mesenchyme that forms the ciliary muscle. The ciliary body has three functional muscle groups:
- Meridional (longitudinal) fibers: stretch the choroid; help open the iridocorneal angle
- Radial (oblique) fibers: flatten the lens for distant vision
- Circular (sphincteric) fibers: round for near vision
Internally, the ciliary body connects to the lens via the zonula (suspensory ligament) - a network of elastic fibers. Contraction of the ciliary muscle changes zonular tension and controls lens curvature (accommodation).
4. Lens
After the lens vesicle detaches from surface ectoderm:
- Anterior cells (cuboidal epithelium) remain as the lens epithelium
- Posterior cells elongate enormously to form primary lens fibers, which fill the cavity of the vesicle with transparent crystallin proteins
- These primary fibers lose their nuclei and form the embryonic nucleus of the lens
- New (secondary) lens fibers are continuously added from the equatorial lens epithelium; this continues throughout life
The lens is avascular throughout its development and remains so in adult life, deriving nutrition from the aqueous humor.
5. Cornea
After the lens vesicle detaches from surface ectoderm, the same ectodermal site re-thickens to form the corneal epithelium (anterior, stratified squamous). Mesenchymal cells then migrate in from the periphery to form:
- Corneal endothelium (posterior single layer; derived from neural crest cells)
- Corneal stroma (fibrous middle layer; also neural crest derived)
The corneal epithelium, stroma, and endothelium together constitute the three main structural layers of the cornea.
6. Vitreous Body
The primary vitreous body is formed by the hyaloid vasculature and associated mesenchyme, initially filling the eye cavity. The secondary vitreous (transparent gel) develops from the optic cup neuroectoderm and gradually replaces it. After birth, the hyaloid vasculature regresses, leaving the hyaloid canal (Cloquet's canal) as an empty channel from the optic disc to the posterior lens surface.
7. Optic Nerve
Axons of the ganglion cells of the retinal nerve fiber layer converge toward the optic disc and enter the optic stalk, converting it into the optic nerve. The optic nerve is surrounded by three meningeal sheaths that evaginate with the optic vesicle and are continuous with the brain meninges:
- Outer dural sheath: thick, fibrous; blends with the sclera
- Intermediate arachnoid sheath: thin
- Inner pial sheath: vascular; closely invests the nerve; contains central retinal vessels to the optic disc
Cerebrospinal fluid is present in the subarachnoid space between the arachnoid and pial sheaths - this is why raised ICP causes papilledema.
Myelination begins in the late fetal period and completes approximately 10 weeks after birth. Normally stops at the optic disc (where optic nerve leaves the eyeball).
8. Sclera and Choroid
- Sclera: derived from mesenchyme surrounding the optic cup; continuous with corneal stroma
- Choroid: richly vascularized layer between the sclera and retina; derived from neural crest-cell mesenchyme
9. Eyelids
Eyelids develop from surface ectodermal folds and mesoderm. Upper and lower eyelid folds grow over the cornea and fuse together at approximately week 9-10, remaining fused until about week 26-28, when they separate. The lacrimal glands, conjunctival epithelium, and eyelid epidermis are all surface ectoderm derivatives.
Molecular Regulation of Eye Development
| Gene/Molecule | Role |
|---|---|
| PAX6 | Master regulatory gene for eye development. Initially expressed in a band across the anterior neural ridge (single eye field). Required for lens placode differentiation and optic cup expression. Mutations → aniridia, microphthalmia, anophthalmia |
| SHH (Sonic Hedgehog) | Secreted by the prechordal plate; separates the single eye field into two optic primordia. Upregulates PAX2 in the midline while downregulating PAX6 |
| PAX2 | Expressed in optic stalks (where PAX6 is suppressed by SHH). Regulates optic stalk differentiation. Mutations → optic nerve coloboma and renal coloboma syndrome |
| FGF (Fibroblast Growth Factors) | From surface ectoderm; promotes differentiation of the neural (inner) retinal layer |
| TGF-β | From surrounding mesenchyme; directs formation of the pigmented (outer) retinal layer |
| MITF | Downstream transcription factor for pigmented retinal layer differentiation |
| CHX10 | Downstream transcription factor for neural retinal layer differentiation |
| BMP / FGF | Essential for signaling optic vesicle and closure of the retinal fissure |
| PITX2 | Important in molecular development of the eye (mesenchymal patterning) |
The lens ectoderm is essential for proper optic cup formation: without a lens placode, no cup invagination occurs.
Timeline Summary
| Week | Key Events |
|---|---|
| Day 22 | Optic grooves appear in neural folds |
| Week 4 | Optic vesicles form; contact surface ectoderm; lens placode thickens |
| Week 5 | Optic vesicle invaginates → optic cup; lens placode invaginates → lens vesicle; lens vesicle detaches from ectoderm; corneal epithelium forms |
| Week 6 | Melanin appears in RPE; hyaloid artery present in choroid fissure; primary lens fibers form |
| Week 7 | Choroid fissure fuses, forming round pupil; optic nerve begins to form |
| Week 9–10 | Eyelids fuse |
| Week 26 | Fetuses blink in response to bright light; eyelids separate |
| Week 34 | Color perception begins |
| Birth + 10 weeks | Myelination of optic nerve fibers complete |
Clinical Correlates
1. Coloboma
Cause: Failure of the choroid fissure (retinal fissure) to close during the 7th week
Types (depending on extent of the unclosed fissure):
- Coloboma iridis (most common): keyhole-shaped defect in the inferior sector of the iris - because the fissure is on the inferior surface, any defects are always inferonasal
- Coloboma of the ciliary body
- Retinochoroidal coloboma: localized gap in the retina, usually inferior to the optic disc; bilateral in most cases
- Coloboma of the optic nerve
Genetics: Simple coloboma is often autosomal dominant. Mutations in PAX2 are linked with optic nerve coloboma and renal coloboma syndrome (renal hypoplasia + optic nerve coloboma). Part of CHARGE syndrome (Coloboma, Heart defects, Atresia choanae, Retarded growth, Genital anomalies, Ear anomalies) - caused by mutations in CHD7.
2. Congenital Cataracts
Cause: Opacity of the lens during intrauterine life, from disturbance during lens fiber formation
Etiology:
- Most are inherited (autosomal dominant most common)
- Rubella virus (German measles): if maternal infection occurs in weeks 4-7 (lens-sensitive period), congenital cataracts result. Infection after week 7 spares the lens but may cause cochlear damage (hearing loss). The MMR vaccine has nearly eradicated this.
- Other TORCH infections: cytomegalovirus, toxoplasmosis
- Clinical: Dense white opacity visible in the pupil; requires surgical removal (lensectomy) followed by optical rehabilitation. Amblyopia (lazy eye) develops rapidly if untreated due to sensory deprivation during the visual critical period.
3. Congenital Glaucoma (Buphthalmos)
Cause: Failure of proper development of the trabecular meshwork and anterior chamber drainage angle (derived from neural crest cells), leading to obstruction of aqueous humor outflow and elevated IOP.
Clinical features: Corneal enlargement (buphthalmos - "ox eye"), corneal clouding, photophobia, excessive tearing, elevated IOP, optic nerve damage.
Genetics: Can be associated with PAX6 mutations, Axenfeld-Rieger syndrome, Peters anomaly, aniridia.
4. Retinal Detachment
Embryological basis: The intraretinal space (between neural retina and RPE, derived from the original optic cup cavity) never fully disappears. Fusion of the two retinal layers is never firm.
Mechanism: Fluid accumulates in the potential space between the neural retina and RPE, separating them. The RPE remains attached to the choroid; the neural retina separates from the RPE (not from the choroid).
Note: The neural retina retains its blood supply from the central retinal artery (derived from the hyaloid artery) even when detached, as the vessels travel with the neural layer.
Associations: Down syndrome, Marfan syndrome, myopia, trauma, lattice degeneration.
5. Persistent Hyaloid Artery
Cause: Failure of the distal portion of the hyaloid artery to regress after birth.
Presentations:
- Bergmeister's papilla: tuft of fibrous tissue at the optic disc
- Mittendorf dot: small opacity on the posterior lens capsule at the former artery attachment
- Persistent hyaloid artery: visible cord or cyst extending through the vitreous
6. Microphthalmia
Definition: Abnormally small eye (eyeball may be only two-thirds normal volume)
Causes and timing:
- Arrest before/just after optic vesicle formation (week 4): severe microphthalmia, no lens, marked ocular defects
- Arrest before retinal fissure closes (before week 6): larger eye but with gross ocular defects
- Arrest at week 8 or early fetal period: simple microphthalmia (small eye, minor abnormalities)
Etiology: Rubella, CMV, toxoplasmosis, HSV, genetic (autosomal dominant/recessive/X-linked). Also associated with PAX6 mutations.
7. Anophthalmia
Definition: Complete absence of the eye; eyelids still form but no eyeball develops.
Types:
- Primary anophthalmia: optic vesicle fails to form (week 4 arrest); histological analysis may still reveal residual ocular tissue
- Secondary anophthalmia: forebrain development is suppressed; part of severe craniocerebral malformation
Because orbital growth depends on stimulation from the developing eye, orbital hypoplasia is always present.
8. Aniridia
Definition: Absence of the iris
Cause: Mutations in PAX6 (haploinsufficiency); can also contribute to anophthalmia and microphthalmia.
Clinical: Associated with Wilms tumor (WAGR syndrome - Wilms tumor, Aniridia, Genitourinary anomalies, intellectual disability/Retardation) when the deletion at chromosome 11p13 includes both PAX6 and WT1 genes.
9. Cyclopia and Synophthalmia
Cyclopia: Single median eye enclosed in a single orbit, typically with a tubular nose (proboscis) superior to the eye.
Synophthalmia: Partial or complete fusion of two eyes.
Cause: Loss of midline tissue as early as days 19-21 → underdevelopment of forebrain and frontonasal prominence → failure of the single eye field to separate into two optic primordia.
Association: Always associated with holoprosencephaly (cerebral hemispheres partially or completely fused); linked to SHH mutations, maternal diabetes, alcohol. Incompatible with life.
10. Persistent Iridopupillary Membrane
Cause: Failure of the anterior vascular mesenchyme (iridopupillary membrane) to resorb during formation of the anterior chamber.
Clinical: Strands of membrane visible crossing the pupil; usually incidental; may reduce visual acuity if dense.
11. Congenital Aphakia and Congenital Absence of Structures
- Congenital aphakia (absence of lens): disturbance in lens vesicle induction; very rare
- Aniridia (absence of iris): PAX6 mutation
- Both represent failures in the inductive cascade between optic vesicle and surface ectoderm
12. Papilledema and the Optic Nerve Sheath
Clinical relevance: Because the optic nerve sheaths are continuous with the brain meninges, CSF extends in the subarachnoid space around the optic nerve. Raised ICP transmits directly along this space, compressing the central retinal vein at the disc, causing papilledema (optic disc swelling visible on fundoscopy).
13. Teratogenic Sensitivity
The critical period for eye development (weeks 4-8) overlaps with sensitivity to teratogens:
- Rubella virus: cataracts, glaucoma, microphthalmia (weeks 4-7 are most critical)
- CMV and Toxoplasma gondii: microphthalmia, chorioretinitis
- Treponema pallidum: interstitial keratitis, chorioretinitis
- Thalidomide: microphthalmia
- Alcohol: microphthalmia, cyclopia spectrum (SHH pathway disruption)
- Vitamin A (retinoic acid) excess: craniofacial malformations including ocular defects
Key Facts to Remember
- The eye is first visible as optic grooves on day 22
- The outer layer of optic cup → RPE; inner layer → neural retina
- The choroid fissure is always on the inferior surface - hence all colobomas are inferonasal
- Coloboma = failure of fissure closure in week 7
- PAX6 = master eye gene; PAX6 mutations → aniridia
- PAX2 = optic stalk gene; PAX2 mutations → renal coloboma syndrome
- SHH separates the single eye field into two primordia; SHH loss → cyclopia
- Rubella cataracts occur with infection in weeks 4-7 (lens-sensitive period)
- Iris muscles (sphincter + dilator) are derived from neuroectoderm (unique - muscle from ectoderm)
- The intraretinal space is the embryological basis for retinal detachment
- Hyaloid artery proximal portion → central retinal artery (persists); distal portion normally degresses
- Optic nerve sheaths are continuous with brain meninges → papilledema in raised ICP
- Langman's Medical Embryology, 14th ed., Chapter 20
- The Developing Human: Clinically Oriented Embryology (Moore & Persaud), Chapter 18
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Ross & Pawlina), Chapter 24
This is a shared conversation. Sign in to Orris to start your own chat.