Anatomy of elbow joint orthopedic exam
Reading File
Finding Sources
Finding Sources
Searching the Web
elbow joint anatomy orthopedic examination clinical tests
Finding Sources
Reading Web Page
elbow joint anatomy orthopedic examination special tests
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from Miller's Review of Orthopaedics and Firestein & Kelley's Textbook of Rheumatology. Let me compile the complete answer.
Elbow Joint - Anatomy & Orthopedic Examination
Sources: Miller's Review of Orthopaedics 9th Ed.; Firestein & Kelley's Textbook of Rheumatology
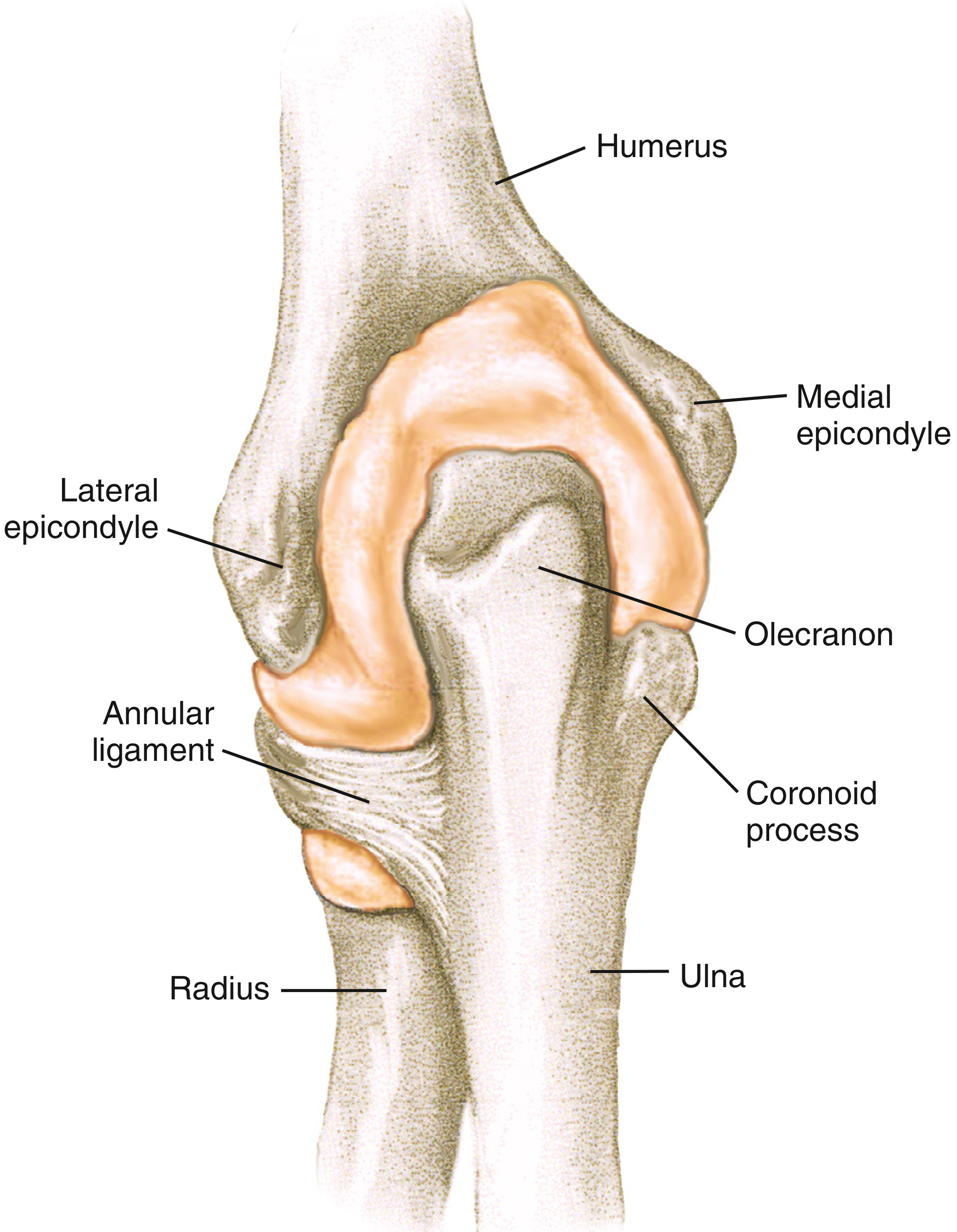
Bony Anatomy
The elbow is composed of three distinct articulations within a shared synovial cavity:
| Articulation | Bones | Function |
|---|---|---|
| Humeroulnar | Trochlea of humerus + trochlear notch of ulna | Primary hinge (flexion/extension) |
| Humeroradial (Radiocapitellar) | Capitulum of humerus + radial head | Flexion + rotation; transmits 60% of axial load in full extension |
| Proximal Radioulnar | Radial head + radial notch of ulna | Pronation/supination |
Key bony landmarks:
- Distal humerus: medial and lateral columns; articular surface angled 30° anterior to humeral shaft axis
- Medial epicondyle - attachment of common flexor tendon (FCR, FCU, palmaris longus, FDS, pronator teres)
- Lateral epicondyle - attachment of common extensor tendon (ECRB, EDC, ECU, anconeus)
- Olecranon - posterior projection of ulna forming the hinge
- Coronoid process - anterior ulna; resists posterior dislocation
- Radial head - secondary stabilizer against valgus stress
Normal Range of Motion
| Movement | Normal Range | Functional Range |
|---|---|---|
| Flexion | 0 - 150° | 30 - 130° |
| Extension | 0° (full) | 30 - 130° |
| Pronation | 0 - 80-85° | 50° |
| Supination | 0 - 80-85° | 50° |
- Valgus carrying angle: 5-10° in men; 10-15° in women
- Cubitus valgus (increased) vs. cubitus varus (decreased/"gunstock deformity")
Ligamentous Anatomy
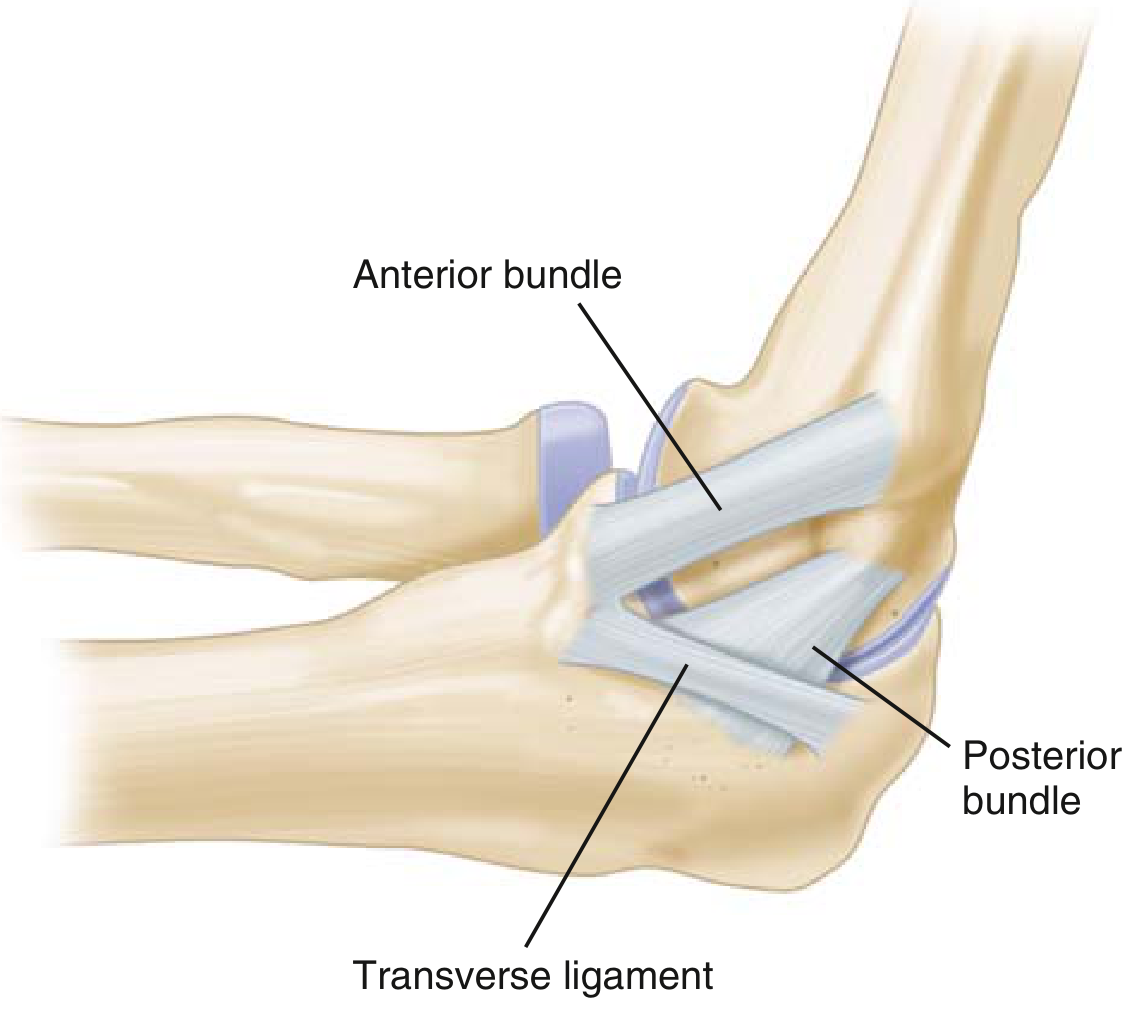
Medial (Ulnar) Collateral Ligament (MCL/UCL) Complex
Three bundles: anterior, posterior, and transverse.
- Anterior bundle = PRIMARY restraint to valgus stress throughout functional ROM
- Origin: posterior medial epicondyle → Insertion: sublime tubercle of medial coronoid process
- Secondary restraint: radial head
- Posterior bundle = primary restraint to valgus in maximal flexion
- Transverse bundle = minimal contribution to stability
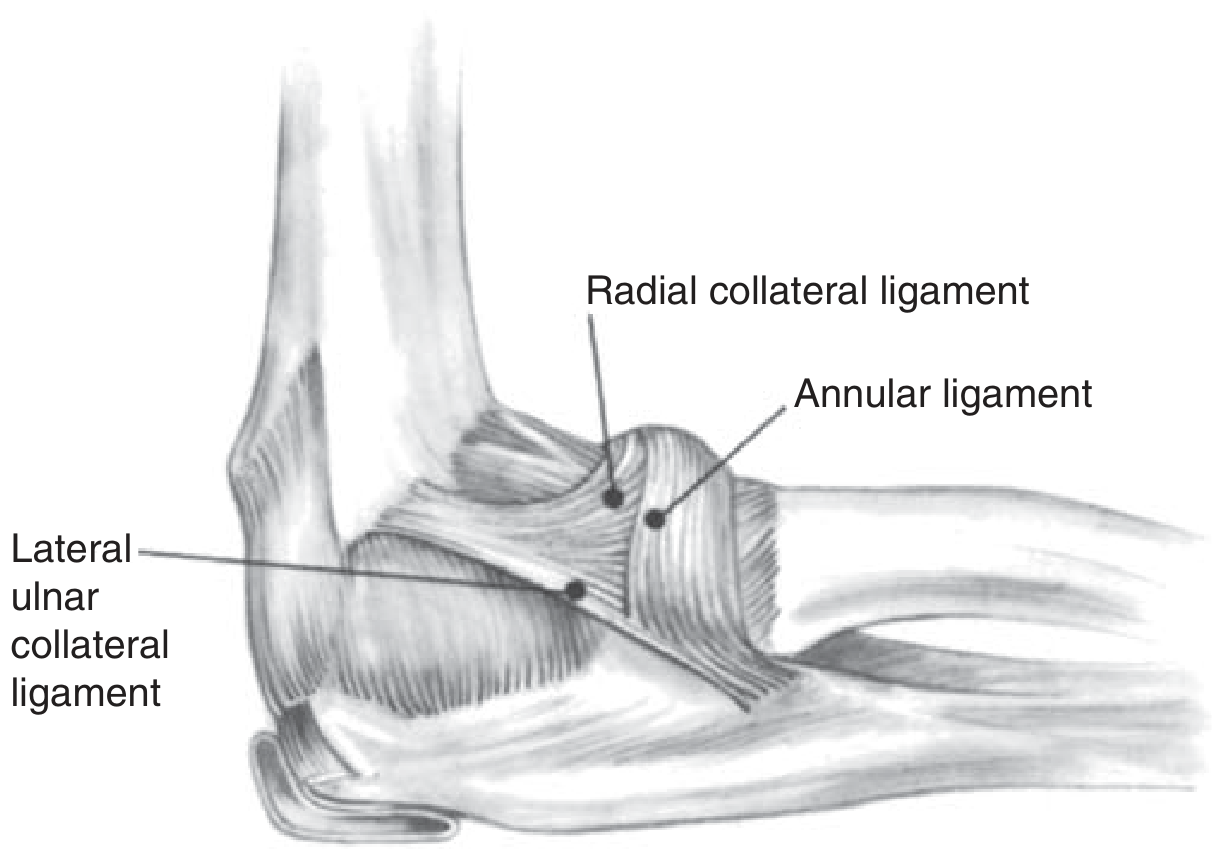
Lateral Collateral Ligament (LCL) Complex
Four components:
- Radial collateral ligament (RCL)
- Lateral ulnar collateral ligament (LUCL) - PRIMARY restraint to varus stress and external rotational stress (posterolateral rotatory instability/PLRI)
- Accessory collateral ligament
- Annular ligament - encircles radial head; maintains radioulnar articulation
Musculature
Flexors (nerve root C5-C6)
- Biceps brachii (musculocutaneous n.) - primary supinator, secondary flexor
- Brachialis (musculocutaneous n.) - primary flexor
- Brachioradialis (radial n.)
Extensors
- Triceps brachii (radial n., C7-C8) - primary extensor
- Anconeus (radial n.) - assists extension; intact anconeus may preserve some extension even after distal triceps rupture
Common Extensor Tendon (from lateral epicondyle)
- ECRB (most commonly implicated in lateral epicondylitis), ECRL, EDC, ECU, anconeus
Common Flexor-Pronator Mass (from medial epicondyle)
- FCR, FCU, palmaris longus, FDS, pronator teres
Neurovascular Anatomy
| Structure | Location | Clinical Relevance |
|---|---|---|
| Ulnar nerve | Medial - cubital tunnel (behind medial epicondyle) | Cubital tunnel syndrome; at risk in medial approaches |
| Radial nerve (divides → PIN + superficial branch) | Lateral, deep to brachioradialis | At risk in lateral epicondylitis surgery; radial tunnel syndrome |
| Median nerve | Anterior | Pronator syndrome; anterior interosseous nerve (AIN) syndrome |
| Lateral antebrachial cutaneous nerve (LABCN) | Lateral | At risk in single-incision distal biceps repair |
| Brachial artery | Anterior cubital fossa | Splits into radial + ulnar arteries at level of radial neck |
Orthopedic Examination
1. Inspection
- Carrying angle deformity (cubitus valgus/varus)
- Swelling, ecchymosis, skin changes
- Olecranon bursa prominence (bursitis)
- Skin: psoriatic plaques, rheumatoid nodules, tophi
- Muscle bulk asymmetry (biceps "Popeye" sign in distal biceps rupture)
2. Palpation
Technique: Examiner places thumb between lateral epicondyle and olecranon in the lateral para-olecranon groove; one or two fingers in the corresponding medial groove. Passively move through flexion, extension, and rotation while palpating.
Key structures to palpate:
- Medial epicondyle - tenderness = medial epicondylitis (golfer's elbow)
- Lateral epicondyle - tenderness = lateral epicondylitis (tennis elbow)
- Olecranon / olecranon bursa - fluctuance, nodules, tophi
- Radial head - rotation palpation; tenderness after radial head fracture
- Cubital tunnel - ulnar nerve tenderness/Tinel's
- Synovial swelling bulges under examiner's thumb on passive extension; synovitis most easily palpated posteriorly between olecranon and distal humerus
3. Range of Motion
- Active then passive in all planes (compare bilateral)
- Limitation of extension = synovitis/effusion (most sensitive sign)
- Mechanical block to rotation = assess for radial head fracture or loose body
4. Strength Testing
| Muscle/Motion | Nerve Root | Test |
|---|---|---|
| Elbow flexion (biceps) | C5-C6 | Resisted supinated flexion |
| Elbow flexion (brachialis) | C5-C6 | Resisted pronated flexion |
| Elbow extension (triceps) | C7-C8 | Resisted extension from 90° |
| Wrist extension | C6-C7 | Resisted dorsiflexion |
| Wrist flexion | C7-C8 | Resisted palmar flexion |
Special Tests
Lateral Elbow
| Test | Technique | Positive Sign | Diagnosis |
|---|---|---|---|
| Cozen's Test | Elbow at 90°, patient makes fist, pronates forearm, extends wrist against resistance | Pain at lateral epicondyle | Lateral epicondylitis |
| Mill's Test | Passive wrist flexion with elbow extended + forearm pronated | Pain at lateral epicondyle | Lateral epicondylitis |
| Middle Finger Extension Test | Examiner resists extension of middle finger at PIP with elbow extended | Pain at lateral epicondyle/common extensor origin | Lateral epicondylitis (ECRB) |
| Pivot Shift Test of the Elbow | Supinate forearm, apply valgus stress + axial load through elbow while moving from extension to flexion | Palpable subluxation/apprehension of radial head at ~40° flexion | LUCL injury / PLRI |
Medial Elbow
| Test | Technique | Positive Sign | Diagnosis |
|---|---|---|---|
| Valgus Stress Test | Elbow at 20-30° flexion (to unlock olecranon from fossa), apply valgus force | Medial pain or laxity > contralateral | MCL injury |
| Moving Valgus Stress Test | Stabilize humerus, apply constant valgus force, rapidly move elbow from full flexion to 30° extension | Reproduction of medial pain between 70-120° of flexion ("shear angle") | MCL insufficiency (highly sensitive in throwers) |
| Valgus Extension Overload Test | Extend elbow rapidly while applying valgus stress | Posteromedial olecranon pain | Posteromedial impingement / valgus overload syndrome |
| Milking Maneuver | Patient reaches under affected arm to pull their own thumb with elbow in flexion; examiner applies valgus stress | Medial pain/instability | MCL injury |
| Golfer's Elbow Test | Resisted wrist flexion + forearm pronation with elbow extended | Pain at medial epicondyle | Medial epicondylitis |
Nerve Tests
| Test | Technique | Positive Sign | Diagnosis |
|---|---|---|---|
| Tinel's Sign (cubital tunnel) | Tap ulnar nerve in cubital tunnel (posterior medial epicondyle) | Tingling in ring + little fingers | Cubital tunnel syndrome (ulnar neuropathy) |
| Elbow Flexion Test | Full elbow flexion + wrist extension for 60 sec | Ulnar paresthesias | Cubital tunnel syndrome |
| Tinel's Sign (radial tunnel) | Tap over radial tunnel (5 cm distal to lateral epicondyle) | Tingling/deep ache in dorsal forearm | Radial tunnel syndrome / PIN compression |
Tendon Tests
| Test | Technique | Positive Sign | Diagnosis |
|---|---|---|---|
| Hook Test | With elbow at 90° + forearm supinated, hook finger under biceps tendon from lateral side | Inability to hook cord-like structure | Distal biceps tendon rupture (100% sensitive) |
| Biceps Squeeze Test | Squeeze biceps muscle belly with elbow at 60-80° flexion | No forearm supination | Distal biceps rupture |
| Triceps Squeeze Test | Squeeze triceps with elbow at 90° | No extension | Distal triceps rupture |
| "Flake Sign" on X-ray | Bone fragment at posterior olecranon on lateral radiograph | Present | Pathognomonic for distal triceps avulsion; warrants MRI |
High-Yield Clinical Correlations
| Finding | Key Anatomy | Implication |
|---|---|---|
| MCL incompetence | Anterior bundle UCL | Valgus instability; Tommy John surgery (UCL reconstruction); ~80% of athletes return to sport at 1 year |
| LUCL incompetence | LUCL | Posterolateral rotatory instability (PLRI); diagnosed by lateral pivot-shift |
| "Terrible Triad" | Radial head + coronoid + capsule + LCL | Elbow dislocation with radial head and coronoid fractures; treat all three |
| Anteromedial coronoid fracture | Coronoid process anteromedial facet | Varus posteromedial rotatory instability |
| Distal biceps rupture | Radial tuberosity footprint (radial side) | Supination strength > flexion strength lost; abnormal Hook test |
| Lateral epicondylitis | ECRB tendon origin (degenerative tendinopathy) | Angiofibroblastic hyperplasia on histology; no inflammatory infiltrate |
| Chronic MCL incompetence | UCL + olecranon fossa | Valgus overload syndrome: posteromedial osteophytes, loose bodies, capitellar wear |
| Postoperative positioning | After LUCL repair | Immobilize in PRONATION to protect lateral repair |
References: Miller's Review of Orthopaedics 9th Edition, p. 723-740; Firestein & Kelley's Textbook of Rheumatology, p. 765
This is a shared conversation. Sign in to Orris to start your own chat.