Hematuria
Reading File
Finding Sources
Searching PubMed
"hematuria" AND "evaluation" AND "guidelines"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile a thorough response.
Hematuria
Definition
Hematuria is the presence of blood in the urine. By convention:
- Gross (macroscopic) hematuria — visible to the naked eye
- Microscopic hematuria — detected only on urinalysis; defined as ≥3 RBCs/high-power field (HPF) on microscopic examination of a properly collected midstream clean-catch specimen
Urine dipstick alone is insufficient — it can be positive with myoglobinuria, hemoglobinuria, or oxidizing contaminants. Microscopic confirmation is required before initiating a full workup. — Campbell-Walsh-Wein Urology
Pseudohematuria (Red Urine Without RBCs)
Conditions that cause red/brown urine without true hematuria include:
- Drugs: phenazopyridine, rifampin, nitrofurantoin, chloroquine, hydroxychloroquine
- Foods: beets, blackberries, rhubarb
- Metabolic: porphyria, myoglobinuria, hemoglobinuria, urate crystals
- Dehydration (concentrated pigments)
Dipstick is positive in myoglobinuria/hemoglobinuria but microscopy shows no RBCs. — Rosen's Emergency Medicine
Classification by Origin
1. Glomerular Hematuria (Nephrologic)
Key features on urinalysis:
- Dysmorphic RBCs — specifically acanthocytes (vesicle-like protrusions); >5% acanthocytes strongly suggests glomerular origin
- Red cell casts (pathognomonic) or mixed RBC/WBC casts
- Concurrent proteinuria strongly supports glomerular disease
- This pattern constitutes nephritic urine
Nephritic syndrome = hematuria + impaired renal function + hypertension
Causes of glomerular hematuria:
| Category | Examples |
|---|---|
| Genetic/structural | Alport syndrome (COL4A3/A4/A5 mutations), Thin Basement Membrane Nephropathy |
| IgA-mediated | IgA nephropathy (most common primary GN worldwide), IgA vasculitis (HSP) |
| Immune complex | MPGN, C3 glomerulopathy, post-infectious GN |
| Autoimmune | Lupus nephritis (SLE), ANCA vasculitis, anti-GBM disease (Goodpasture) |
| Vascular | Thrombotic microangiopathy (HUS/TTP), malignant hypertension |
— Brenner & Rector's The Kidney
2. Non-Glomerular Hematuria (Urologic)
RBCs are eumorphic (normal shape); no casts. Bleeding from kidneys, ureters, bladder, prostate, or urethra.
Common urologic causes:
- Urolithiasis (most common cause in adults overall)
- Urinary tract infection / cystitis (most common cause in young women)
- Bladder cancer — most common cause of gross hematuria in patients >50 years; found in 20–25% with gross hematuria
- Renal cell carcinoma
- Urothelial carcinoma (upper tract)
- Benign prostatic hyperplasia (BPH — increased vascularity)
- Renal papillary necrosis (sickle cell, analgesic nephropathy, diabetes)
- Vascular: renal AV fistula, AAA (must exclude in ED)
- Exercise-induced (transient, resolves with rest)
- Trauma / urologic procedures
- Anticoagulation (supratherapeutic — does not cause hematuria at therapeutic levels)
- Hemorrhagic cystitis: cyclophosphamide, ifosfamide, radiation, BK virus (especially in immunocompromised/transplant patients), adenovirus
Localizing the Bleeding
Stream timing provides clues:
| Pattern | Likely source |
|---|---|
| Initial stream hematuria | Urethra or prostate |
| Terminal hematuria | Bladder neck (contracts at end of voiding) |
| Total stream hematuria | Bladder or upper tract |
Clot morphology:
- Vermiform (worm-shaped) clots → formed in upper urinary tract (ureter molds them)
- Cuboid/amorphous clots → formed in bladder
Risk Factors for Urologic Malignancy
- Age >35 years (cystoscopy warranted)
- Male sex
- Smoking (most important modifiable risk factor for bladder cancer)
- Industrial chemical exposure (aromatic amines, benzidine, dyes)
- Prior alkylating chemotherapy (cyclophosphamide, ifosfamide)
- Analgesic abuse (phenacetin)
- Chronic foreign body / indwelling catheter (squamous cell carcinoma risk)
- Schistosomiasis (squamous cell bladder cancer)
- Gross hematuria (higher yield than microscopic)
Evaluation
Initial Assessment
- Confirm true hematuria by microscopy (rule out pseudohematuria, menstruation, catheter artifact)
- History: UTI symptoms? Trauma? Recent urologic procedure? Family history of renal disease? Medications? Smoking/occupational exposure?
- Physical exam: BP, edema (nephrotic/nephritic), abdominal mass/bruit, flank tenderness, genital/rectal exam
- Urinalysis with microscopy: RBC morphology, casts, proteinuria
- Urine culture: to exclude infection
- Renal function tests (serum creatinine, eGFR)
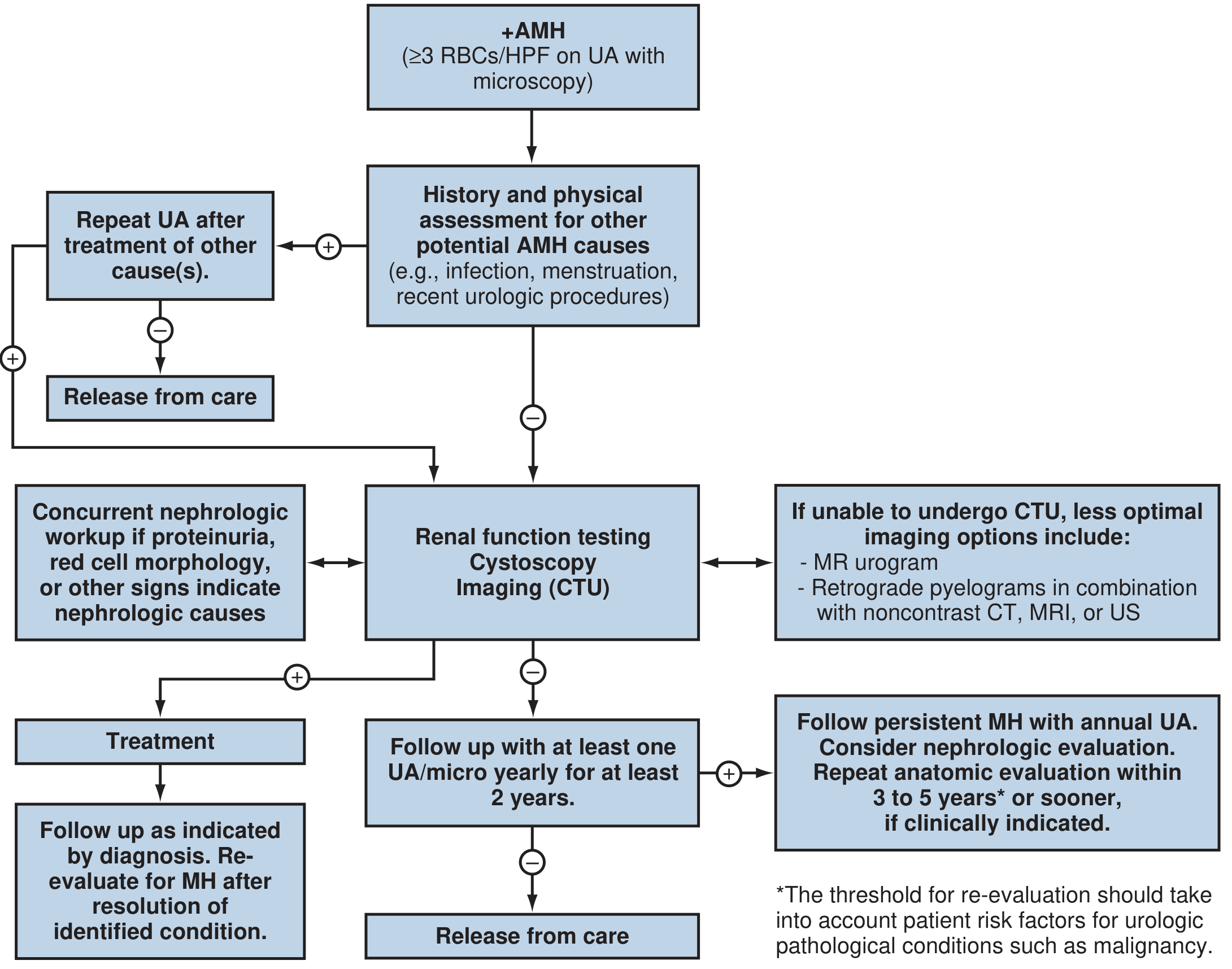
AUA Guidelines for Asymptomatic Microhematuria (AMH)
Step 1: Exclude benign causes (UTI, menstruation, recent procedure) → treat and repeat UA. If clears → release from care.
Step 2: If no benign cause → proceed with full evaluation:
- Renal function testing
- Cystoscopy — recommended for all adults ≥35 years old and/or those with malignancy risk factors; may be omitted in patients <35 without risk factors
- CT Urogram (CTU) — preferred upper tract imaging (multiphasic CT with pre-contrast, nephrographic, and excretory phases); highest sensitivity/specificity for renal parenchymal and upper tract lesions
- Alternatives if CTU contraindicated (pregnancy, contrast allergy, renal insufficiency): MR urogram, retrograde pyelograms + non-contrast CT/US
If nephrologic signs (proteinuria, dysmorphic RBCs, red cell casts, AKI) → concurrent nephrology referral
Step 3 — Follow-up:
- Negative evaluation: annual UA for ≥2 years
- Persistent MH after negative evaluation: consider nephrology referral; repeat anatomic evaluation in 3–5 years or sooner if clinically indicated
Symptomatic Microhematuria
- Malignancy risk higher (~10.5% vs <5% asymptomatic)
- Cystoscopy recommended regardless of age
- Urine cytology is an option (but does not replace cystoscopy)
Gross Hematuria
- Malignancy in 20–25%; cause found in ~50%
- Assess hemodynamic stability, CBC (anemia), coagulation parameters if on anticoagulation
- Full evaluation: cystoscopy + upper tract imaging (CTU) + urine cytology
- If culture-documented UTI → treat first, then repeat UA to confirm clearance
Special Situations
| Scenario | Key Point |
|---|---|
| Children | Microscopic hematuria defined as >5 RBCs/HPF on ≥2 weekly samples; most common cause is glomerular; evaluate for IgA nephropathy, Alport syndrome, hypercalciuria |
| Young women | Exclude UTI first — most common cause |
| Renal transplant recipients | Follow AUA AMH guidelines; additionally include BK virus in the differential (confirm with urine cytopathology and BK virus titers) |
| Anticoagulated patients | Therapeutic anticoagulation does NOT cause hematuria; persistent hematuria requires full workup |
| Post-exercise | Transient, benign; resolves within 24–72 hours with rest |
| Hemorrhagic cystitis | Cyclophosphamide/ifosfamide (acrolein metabolite) — prevented with mesna + hydration; treatment: irrigation, intravesical agents, embolization, or cystectomy in refractory cases |
Urine Cytology and Tumor Markers
- Routine cytology is NOT recommended for asymptomatic MH workup
- High sensitivity for high-grade/CIS bladder cancer; low sensitivity for low-grade lesions
- Blue-light cystoscopy (with ALA or HAL) — AUA recommends against use for MH evaluation (not validated in MH populations)
- Urine NMP22, BTA, and other biomarkers: not recommended as standalone substitutes for cystoscopy
Key Statistics
- Up to 25% of adults with hematuria are found to have a urologic malignancy
- 2.6% malignancy rate in screening studies of asymptomatic MH
- ~61% of hematuria patients have no significant pathology identified
- Bladder cancer accounts for 97% of malignancies found in patients >35 with AMH
- Gross hematuria: 30–40% have urinary tract malignancy (vs 5% in asymptomatic MH)
Sources: Campbell-Walsh-Wein Urology | Brenner & Rector's The Kidney | Rosen's Emergency Medicine | Textbook of Family Medicine 9e | National Kidney Foundation Primer on Kidney Diseases
Recent evidence: A 2023 systematic review and meta-analysis in J Urol (PMID 36883858) specifically evaluated diagnostic imaging modalities for asymptomatic microhematuria, supporting CTU as the preferred modality.
This is a shared conversation. Sign in to Orris to start your own chat.