Optometry
Asking for Preferences
Asking for Preferences
When we do refraction
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough breakdown of refraction in optometry:
Refraction in Optometry
1. The Goal of Refraction
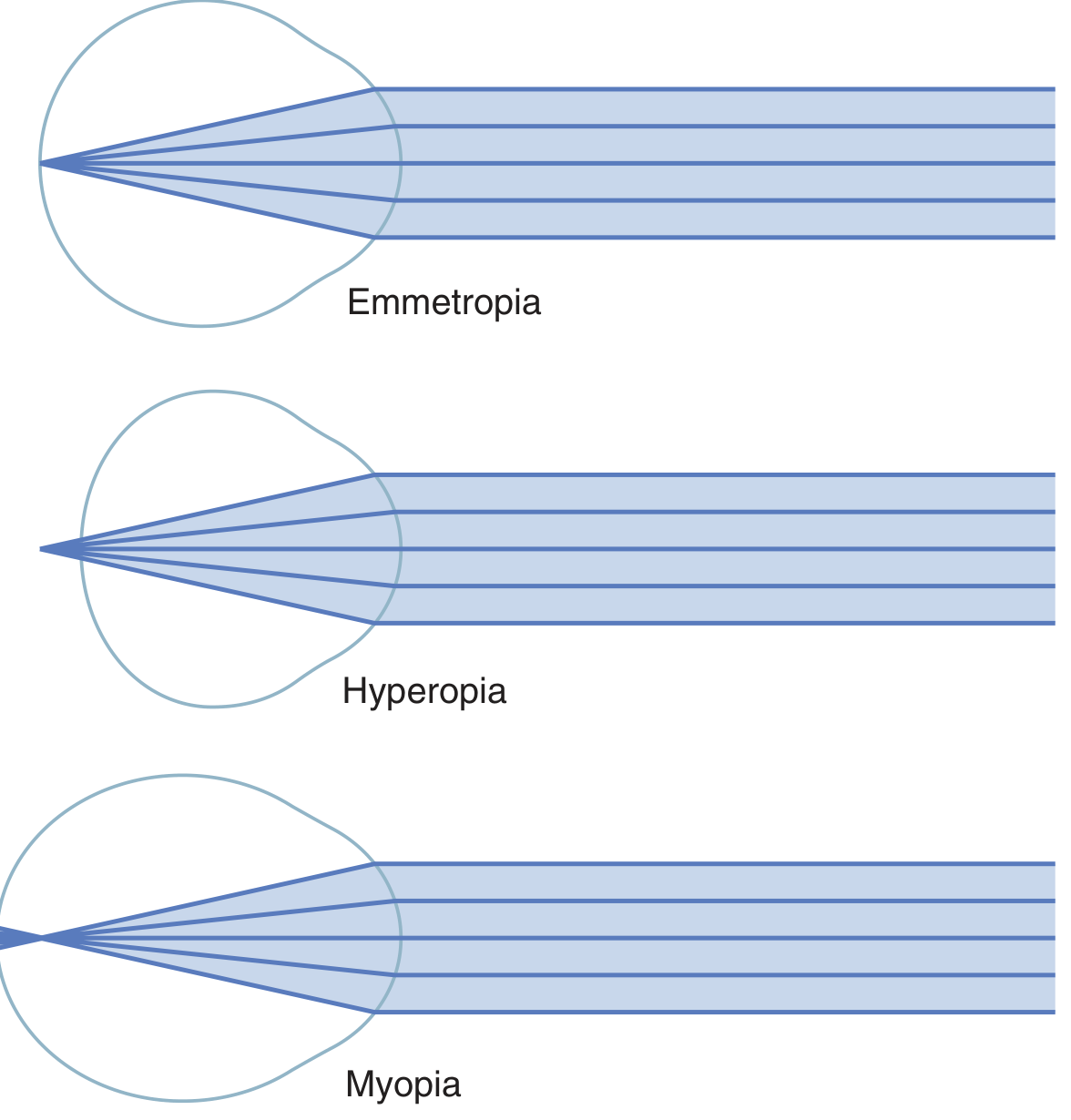
Refraction is the process of determining the lens power needed to bring parallel light rays to a sharp focus on the retina (fovea). The ideal outcome is emmetropia - where the relaxed eye focuses distant objects exactly on the retina. Any deviation from this is a refractive error.
2. Types of Refractive Error You Are Measuring For
| Condition | Mechanism | Correction |
|---|---|---|
| Emmetropia | Focal point lands on retina | No correction needed |
| Myopia (nearsightedness) | Eyeball too long OR lens too strong - image focuses in front of retina | Concave (minus) lens |
| Hyperopia (farsightedness) | Eyeball too short OR lens too weak - image focuses behind retina | Convex (plus) lens |
| Astigmatism | Uneven corneal/lens curvature - two focal points | Cylindrical lens |
| Presbyopia | Age-related loss of accommodation | Reading addition (bifocal/progressive) |
In myopia, the ciliary muscle cannot decrease lens power below its resting state, so no accommodation can compensate - a minus lens is required. In hyperopia, a patient may partially compensate through accommodation, so cycloplegia is sometimes needed to reveal the full amount of latent hyperopia.
- Guyton and Hall Textbook of Medical Physiology, p. 625
3. Steps in the Refraction Procedure
Step 1 - Visual Acuity Baseline
Record uncorrected (UCVA) and best corrected (BCVA) visual acuity using a Snellen or LogMAR chart at 6 m (20 ft). This establishes your starting point and target.
Step 2 - Objective Refraction
Before asking the patient any questions, you first get an objective estimate of the refractive error:
a) Retinoscopy (Skiascopy)
- The gold standard objective method, especially for children and non-verbal patients.
- A retinoscope projects a streak or spot of light into the eye. You observe the reflex in the pupil as you sweep the light beam:
- "With" motion (reflex moves same direction as beam) → add plus lenses to neutralize → indicates hyperopia or low myopia
- "Against" motion (reflex moves opposite to beam) → add minus lenses → indicates myopia
- Neutralization point: when the reflex appears to fill the entire pupil with no movement - this is your working distance correction
- A working distance correction of -1.50 D (for 67 cm) or -1.00 D (for 100 cm) is subtracted from the gross retinoscopy result to get the net refractive error
b) Autorefraction
- An automated instrument (autorefractor) projects an infrared target onto the retina and calculates the refractive error electronically
- Fast and reproducible, but not definitive - it is a starting point for subjective refinement
- Can be unreliable in patients with irregular corneas, cataracts, or poor fixation
Step 3 - Cycloplegic Refraction (when indicated)
In children and young hyperopes, the ciliary muscle is always partially contracted (latent hyperopia masked by accommodation). A cycloplegic agent paralyzes the ciliary muscle to reveal the full refractive error:
- Cyclopentolate 1% - one drop, repeated after 5 minutes; maximum cycloplegia within 30 minutes; accommodation recovers in 2-3 hours; preferred for most children
- Atropine 1% - stronger cycloplegia; used for heavy hyperopia, darkly pigmented irides, or when cyclopentolate is insufficient; instilled at home twice daily for 1-3 days before the exam; vision effects last up to 2 weeks; watch for systemic toxicity (flushing, fever, restlessness)
- Topical anesthetic (e.g., proxymetacaine) before cycloplegic drops reduces irritation and reflex tearing, ensuring better drug retention
After cycloplegia is confirmed (check by dynamic retinoscopy - compare readings for distance and near fixation), retinoscopy gives the full cycloplegic refraction.
- Kanski's Clinical Ophthalmology, p. (Strabismus chapter - Cycloplegia section)
Step 4 - Subjective Refraction
Using the objective result as a starting point, you refine the prescription interactively with the patient using a phoropter (refractor head) or trial frame + trial lenses:
a) Spherical refinement (Duochrome / Red-Green test)
- Start from the objective refraction
- Fogging technique: over-plus the patient to relax accommodation, then reduce plus (or increase minus) until best acuity
- Duochrome test: uses chromatic aberration - red and green wavelengths focus at slightly different points. When letters on the green side look sharper → over-minused (add plus). When letters on the red side look sharper → under-minused (add minus). End point: both sides appear equally clear
b) Cylinder refinement (Jackson Cross Cylinder)
- A Jackson Cross Cylinder (JCC) is a combined +0.25/-0.50 D crossed cylinder lens on a handle
- Axis check: flip the JCC around the axis of the trial cylinder - the patient picks which orientation gives clearer/sharper lines on the astigmatism chart
- Power check: flip JCC with its axes at 45° to the trial cylinder - patient picks which gives clearer vision; add or reduce cylinder power accordingly
- Repeat axis and power checks iteratively until the patient cannot distinguish between the two JCC positions
c) Binocular balance
- Once monocular refraction is complete, balance the two eyes so accommodation is equal bilaterally
- Methods: fogging one eye and testing the other, or alternating occlusion with Risley prisms
d) Near addition (for presbyopia)
- For patients over ~40 years with reduced near vision
- Start with an age-appropriate add (typically +1.00 D at 40 years, increasing ~+0.25 D per 2 years)
- Refine by testing near acuity at the patient's habitual reading distance
4. Special Considerations
In children (under 6 years): Prescribe the full cycloplegic hypermetropic refraction (from retinoscopy), deducting only a working distance allowance. This is essential to prevent amblyopia and to correct accommodative esotropia. Recheck at least annually since refraction changes with age - most infants are hypermetropic, astigmatism tends to decrease after age 2, and hypermetropia may peak around age 6.
After age 8: Perform refraction without cycloplegia and prescribe the maximum "plus" the patient can accept (manifest hypermetropia).
Astigmatism in children: Correct fully if causing amblyopia or significant visual symptoms.
Anisometropia: A difference in refractive power between the two eyes - important to correct fully in children to prevent anisometropic amblyopia.
- Kanski's Clinical Ophthalmology, p. (Strabismus/Amblyopia chapter)
5. The Final Prescription
The prescription is written in the standard form:
Sphere / Cylinder × Axis
Example: -2.50 / -1.00 × 180 means:
- -2.50 D sphere (myopic)
- -1.00 D cylinder at axis 180° (astigmatism)
A near addition is written separately: Add +2.00
Summary Flow
Uncorrected VA
↓
Objective refraction (retinoscopy / autorefractor)
↓
Cycloplegia if needed (children, latent hyperopia)
↓
Subjective refraction (fogging → duochrome → JCC)
↓
Binocular balance
↓
Near addition (if presbyopic)
↓
Final prescription
The key principle throughout is to find the least minus (or most plus) lens that gives the best visual acuity, so you don't over-accommodate the patient or mask latent hyperopia.
This is a shared conversation. Sign in to Orris to start your own chat.