How to look for ptosisi in resting position
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed to give a thorough, well-illustrated answer.
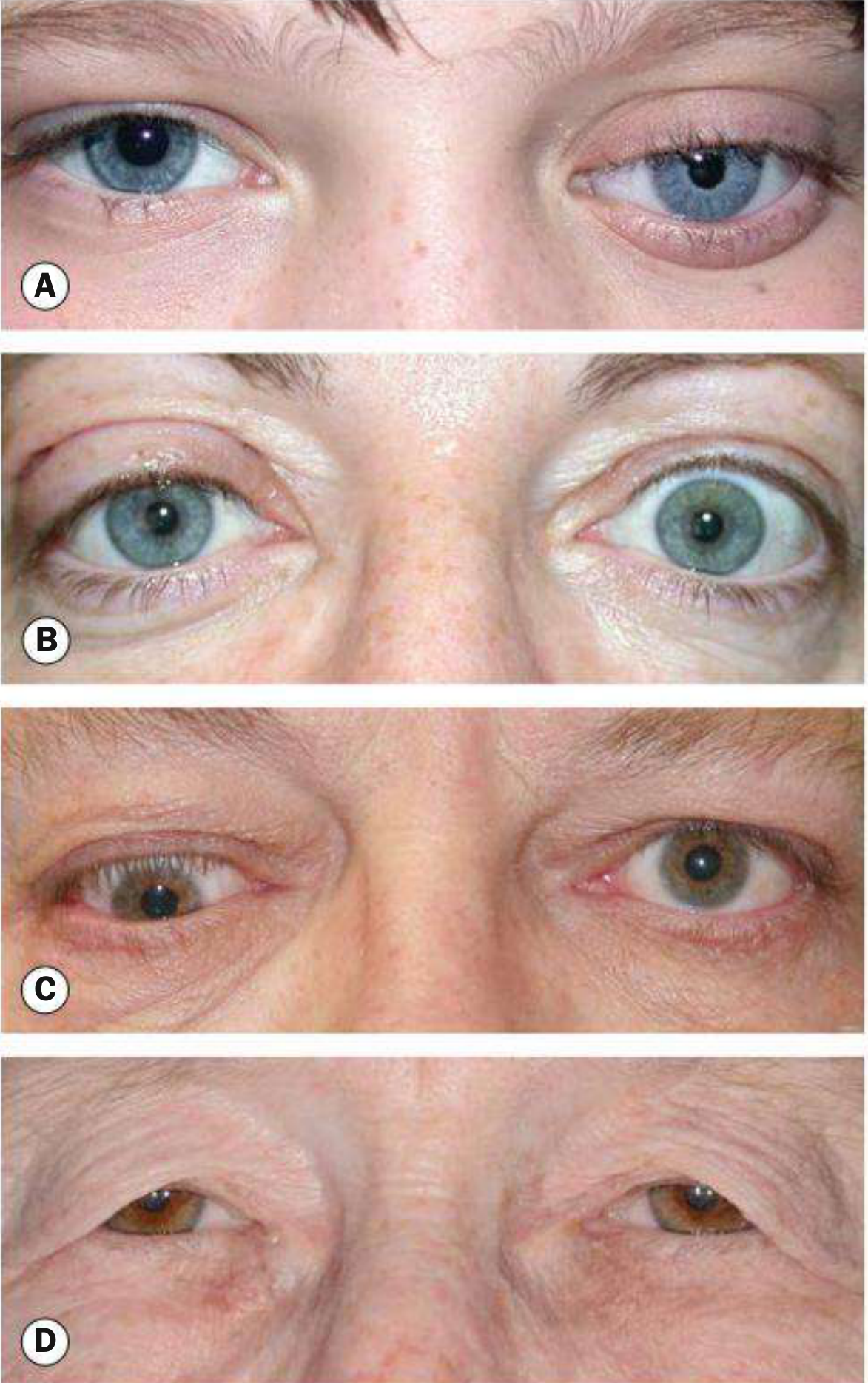
Examining Ptosis in the Resting (Primary) Position
Ptosis is an abnormally low position of the upper eyelid. Assessing it in the resting (primary gaze) position is the first and most important step of the clinical examination.
Step 1 - Know What Normal Looks Like
In primary gaze (eyes looking straight ahead at rest), the normal eyelid positions are:
- Upper lid: covers the upper 1-2 mm of the iris (sits just below the upper limbus)
- Lower lid: just touches the lower border of the iris (lower limbus)
- Palpebral fissure height: normally 12-15 mm (7-10 mm in males; 8-12 mm in females)

Normal Eyelid Position - Bradley & Daroff's Neurology
Step 2 - Observe in the Resting Position (Observe for at Least 1 Minute)
With the patient looking straight ahead in primary gaze, check for:
- Palpebral fissure asymmetry - compare the two sides
- Where the upper lid margin falls relative to the iris edge - if it covers more than 2 mm of the iris, suspect ptosis
- Margin-Reflex Distance (MRD1) - distance from the upper lid margin to the corneal light reflex when you shine a pen torch at the patient. Normal = 4-5 mm. A reduced MRD1 confirms ptosis
- Scleral show - if sclera is visible above the iris (upper scleral show), the lid is retracted, not ptotic; if visible below the iris, lower lid is retracted
- Brow elevation/frontalis contraction - patients with bilateral ptosis often raise their eyebrows reflexively to lift the lids. This can mask the degree of ptosis
Step 3 - Grade the Ptosis
Using palpebral fissure height compared to the normal side (for unilateral cases):
| Grade | Droop |
|---|---|
| Mild | up to 2 mm |
| Moderate | 3 mm |
| Severe | 4 mm or more |
Step 4 - Rule Out Pseudoptosis
A false appearance of ptosis can come from:
- Contralateral lid retraction - the other eye looks abnormally wide, making the normal eye look ptotic
- Ipsilateral hypotropia - the upper lid follows the depressed globe downward; disappears when that eye fixes
- Brow ptosis / dermatochalasis - excess forehead skin droops; elevate the brow manually to distinguish
- Small/absent globe - e.g., phthisis bulbi, artificial eye, enophthalmos
Causes of pseudoptosis - Kanski's Clinical Ophthalmology
Step 5 - Additional Observations in Resting Position
- Upper lid crease height: measured in downgaze. Normal ~10 mm (females), ~8 mm (males). A high crease suggests aponeurotic (involutional) ptosis; absent crease suggests poor levator function (often congenital)
- Pretarsal show: distance between lid margin and skin fold in primary position
- Fatiguability: if ptosis worsens after sustained upgaze or during the day - think myasthenia gravis
Quick Summary Table
| What to Look For | Normal Value | Abnormal Finding |
|---|---|---|
| Upper lid position | 1-2 mm below upper limbus | More than 2 mm below = ptosis |
| MRD1 (margin-reflex distance) | 4-5 mm | Reduced = ptosis |
| Palpebral fissure height | 12-15 mm | Asymmetry or reduced = ptosis |
| Lid crease | 8-10 mm | Absent or high crease |
| Brow position | Relaxed | Elevated = compensatory sign |
Sources: Bradley and Daroff's Neurology in Clinical Practice, Box 17.1 & pp. 279-280 | Kanski's Clinical Ophthalmology, 10th ed., pp. 89-90
This is a shared conversation. Sign in to Orris to start your own chat.