How will you classify anemia clinically by looking pallor and D/d of pallor with discussion
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching Images
pallor grading clinical examination anemia conjunctiva palm
Loading Image
Loading Image
I now have comprehensive material to give a thorough, well-structured answer. Let me compose it:
Clinical Classification of Anemia & Differential Diagnosis of Pallor
PART I — What is Pallor and How to Elicit It
Pallor is the abnormal paleness of skin and mucous membranes resulting from reduced blood flow, reduced hemoglobin, or reduced skin pigment in superficial vessels. In clinical medicine it is the single most important bedside sign of anemia.
Sites to Examine for Pallor
| Site | Technique | Significance |
|---|---|---|
| Palpebral conjunctiva | Pull down lower lid, examine inner mucosal surface | Most reliable sign; not affected by skin pigmentation |
| Palmar creases | Extend patient's hand, compare crease color to examiner's | Creases lose pink color when Hb < 7–8 g/dL |
| Nail beds | Compress nail, release — look at color return | Less reliable |
| Tongue / oral mucosa | Inspect under good light | Useful in dark-skinned patients |
| Lips | Compare to examiner | Useful supplementary site |
| Facial skin | General inspection | Unreliable in dark skin tones |
The palpebral conjunctiva is the gold standard — it is independent of racial skin pigmentation, vasoconstriction, or cold.
Clinical Grading of Pallor
| Grade | Description | Approximate Hb |
|---|---|---|
| Mild | Pallor detectable only at conjunctiva; not obvious elsewhere | ~9–11 g/dL |
| Moderate | Conjunctival + palmar pallor; patient symptomatic on exertion | ~7–9 g/dL |
| Severe | Pallor at all sites including tongue, lips; symptomatic at rest, dyspnea | < 7 g/dL |
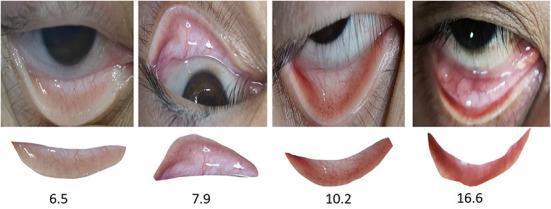
The second image below shows conjunctival pallor correlated with actual hemoglobin levels (Hb 6.5, 7.9, 10.2, 16.6 g/dL):

PART II — Clinical Classification of Anemia
Once pallor confirms anemia, classification guides workup. There are two complementary frameworks:
A. Morphological Classification (by MCV — Mean Corpuscular Volume)
Pioneered by Max Wintrobe; practical and directs the initial workup.
1. Microcytic Anemia (MCV < 80 fL)
Caused by any process interfering with hemoglobin synthesis — less Hb → smaller cells.
| Cause | Mechanism | Key Feature |
|---|---|---|
| Iron deficiency | Inadequate iron for heme synthesis | Hypochromic, low ferritin, low serum iron |
| Thalassemia | Defective globin chain synthesis | Target cells, Hb electrophoresis abnormal |
| Anemia of chronic disease | Hepcidin blocks iron delivery | Normal/high ferritin, low TIBC |
| Sideroblastic anemia | Defective heme synthesis (pyridoxine-B6 deficiency, lead) | Ring sideroblasts on marrow |
| Lead poisoning | Inhibits heme synthesis enzymes | Basophilic stippling |
2. Macrocytic Anemia (MCV > 100 fL)
Due to defective DNA synthesis (megaloblastic) or membrane/other causes.
| Sub-type | Causes |
|---|---|
| Megaloblastic (oval macrocytes) | Vitamin B12 deficiency, Folate deficiency, Methotrexate, Hydroxyurea, Myelodysplasia |
| Non-megaloblastic (round macrocytes) | Alcohol use disorder, Liver disease, Hypothyroidism, Reticulocytosis (hemolysis), Dysproteinemia |
3. Normocytic Anemia (MCV 80–100 fL)
Broad category; requires reticulocyte count to further subdivide.
| Cause |
|---|
| Aplastic anemia |
| Anemia of chronic disease (early/pure) |
| Renal disease (↓ EPO) |
| Endocrinopathies (hypothyroidism, hypoadrenalism) |
| Bone marrow infiltration (leukemia, myeloma, metastases) |
| Pure red cell aplasia |
| Early iron/B12/folate deficiency (before MCV changes) |
B. Pathophysiological Classification (by Mechanism)
The reticulocyte count is the key discriminator:
↑ Reticulocytes → Hyperproductive (bone marrow responding normally)
↓ Reticulocytes → Hypoproductive (bone marrow failing to respond)
1. Decreased Red Cell Production (Hypoproliferative)
(Reticulocyte count LOW)
| Category | Examples |
|---|---|
| Nutritional deficiency | Iron, B12, folate, copper, vitamin C |
| Erythropoietin deficiency | Chronic kidney disease |
| Bone marrow failure | Aplastic anemia (immune-mediated, drug-induced, radiation) |
| Marrow infiltration | Leukemia, myeloma, metastatic cancer, myelofibrosis |
| Pure red cell aplasia | Parvovirus B19, thymoma, Diamond–Blackfan syndrome |
| Chronic inflammation | Hepcidin ↑ → iron sequestration |
| Endocrine | Hypothyroidism, hypopituitarism, Addison's disease |
2. Increased Red Cell Destruction — Hemolytic Anemia
(Reticulocyte count HIGH; unconjugated bilirubin ↑, LDH ↑, haptoglobin ↓)
| Sub-type | Examples |
|---|---|
| Intrinsic (corpuscular) | |
| — Membrane defects | Hereditary spherocytosis, elliptocytosis |
| — Enzyme defects | G6PD deficiency, pyruvate kinase deficiency |
| — Hemoglobinopathies | Sickle cell disease, thalassemia major |
| — Acquired | Paroxysmal nocturnal hemoglobinuria (PNH) |
| Extrinsic (extracorpuscular) | |
| — Immune-mediated | Autoimmune (warm/cold), drug-induced, transfusion reactions |
| — Microangiopathic | HUS, TTP, DIC, malignant hypertension |
| — Infections | Malaria, babesiosis, Clostridium septicemia |
| — Mechanical | Prosthetic heart valves, march hemoglobinuria |
3. Blood Loss
(Reticulocyte count HIGH after 3–7 days)
| Type | Examples |
|---|---|
| Acute hemorrhage | Trauma, GI bleed, ruptured ectopic pregnancy |
| Chronic blood loss | GI lesions, menorrhagia → eventually leads to iron deficiency |
PART III — Differential Diagnosis of Pallor
Pallor ≠ Anemia. Pallor has multiple causes. The clinical distinction is critical.
Causes of Pallor (with and without Anemia)
I. Anemic Causes (reduced RBC mass / Hb)
(Confirmed by CBC — low Hb)
| Category | Examples |
|---|---|
| Iron deficiency anemia | Dietary, blood loss (GI, menstrual) |
| Megaloblastic anemia | B12/folate deficiency |
| Hemolytic anemias | Hereditary spherocytosis, sickle cell, G6PD |
| Aplastic anemia | Idiopathic, drugs (chloramphenicol, benzene) |
| Anemia of chronic disease | TB, rheumatoid arthritis, malignancy, CKD |
| Thalassemia | α or β thalassemia |
| Leukemia / bone marrow infiltration | Acute leukemia, myeloma |
II. Non-Anemic Causes (normal Hb — pallor from reduced skin blood flow)
| Cause | Mechanism | Key Distinguishing Feature |
|---|---|---|
| Shock (hypovolemic, cardiogenic, septic) | Sympathetic catecholamine release → cutaneous vasoconstriction | Tachycardia, hypotension, cold clammy skin — Robbins: "shocky skin coolness and pallor" |
| Vasovagal syncope | Vagally mediated hypotension + peripheral vasoconstriction | Preceded by prodrome (nausea, light-headedness), bradycardia |
| Raynaud's phenomenon | Episodic digital vasospasm | Cold-triggered; affects digits in white–blue–red color sequence |
| Hypothyroidism | Reduced cardiac output + myxedematous skin thickening | Dry skin, cold intolerance, bradycardia, raised TSH |
| Hypopituitarism / Addison's disease | Loss of MSH (in Addison's, paradoxically can cause pallor due to failure of adrenal androgen) | Other features of endocrine failure |
| Chronic renal failure | Pallor + sallow yellow (urochrome) + concurrent anemia | Elevated creatinine/urea |
| Congestive heart failure | Reduced skin perfusion | Dyspnea, elevated JVP, S3 |
| Constitutionally pale individuals | Reduced skin melanin | Normal CBC, normal exam |
| Fear / anxiety | Adrenaline-induced vasoconstriction | Situational |
Approach to a Patient with Pallor: Key Differentiating Features
PALLOR
│
├── Check CBC + reticulocyte count
│ │
│ ├── Hb LOW → ANEMIA confirmed
│ │ │
│ │ ├── MCV LOW (microcytic)
│ │ │ → Iron studies, Hb electrophoresis
│ │ │ DDx: IDA, thalassemia, chronic disease
│ │ │
│ │ ├── MCV HIGH (macrocytic)
│ │ │ → B12/folate levels, peripheral smear
│ │ │ DDx: Megaloblastic, liver disease, hypothyroidism
│ │ │
│ │ └── MCV NORMAL (normocytic)
│ │ → Reticulocytes:
│ │ HIGH → hemolysis or hemorrhage
│ │ LOW → aplasia, CKD, marrow infiltration
│ │
│ └── Hb NORMAL → NON-ANEMIC pallor
│ → Check vitals, thyroid, cardiac, renal function
│ DDx: Shock, vasovagal, hypothyroidism, Raynaud's
│
└── Look for associated features:
Jaundice → Hemolytic anemia
Splenomegaly → Hemolysis, portal hypertension
Koilonychia, glossitis, angular stomatitis → Iron deficiency
Peripheral neuropathy → B12 deficiency
Bony deformity (frontal bossing) → Thalassemia major
Petechiae/bruising → Aplastic anemia or leukemia
Lymphadenopathy → Malignancy, leukemia
Summary Table: Anemia Type by Clinical Clues
| Clinical Clue | Likely Anemia Type |
|---|---|
| Koilonychia, glossitis, angular stomatitis, Plummer–Vinson syndrome | Iron deficiency |
| Subacute combined degeneration (posterior column signs) | B12 deficiency |
| Jaundice + splenomegaly + family history | Hereditary hemolytic (spherocytosis, sickle cell) |
| Lemon-yellow skin (pallor + mild jaundice) | Megaloblastic (B12/folate) |
| Bony deformity (frontal bossing, maxillary hypertrophy) + hepatosplenomegaly in child | β-Thalassemia major |
| Petechiae, recurrent infections, easy bruising | Aplastic anemia |
| Chronic illness (TB, RA, CKD, malignancy) | Anemia of chronic disease |
| Sickle cell crises, dactylitis | Sickle cell disease |
| Dark urine, Coombs test + | Autoimmune hemolytic anemia |
| Pancytopenia + marrow infiltration | Leukemia/myeloma/myelofibrosis |
References:
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025) — Anemia Definition and Classification, p. 492
- Robbins & Kumar Basic Pathology — Red Cell Disorders, Table 10.1
- Robbins, Cotran & Kumar Pathologic Basis of Disease — Table 14.1 (Classification of Anemia by Mechanism)
- Tintinalli's Emergency Medicine, Table 144-2 — Classification of Anemia
Anemia classification according to amount of Hb
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
WHO classification anemia severity hemoglobin levels mild moderate severe very severe g/dL
Searching Images
WHO anemia classification severity hemoglobin levels table
I now have all the data needed — WHO 2024 guidelines, textbook reference ranges, and clinical correlations. Here is the comprehensive answer:
Classification of Anemia According to Amount of Hemoglobin (Hb)
This is the severity-based (quantitative) classification — the most clinically practical, as it directly guides management decisions including transfusion thresholds and treatment urgency.
WHO Definition of Anemia (Baseline)
The World Health Organization (WHO) defines anemia at sea level as:
| Population | Hb Threshold for Anemia |
|---|---|
| Adult men (≥15 years) | < 13.0 g/dL (130 g/L) |
| Adult non-pregnant women (≥15 years) | < 12.0 g/dL (120 g/L) |
| Pregnant women | < 11.0 g/dL (110 g/L) |
— WHO Guideline on Haemoglobin Cutoffs, 2024; Tietz Textbook of Laboratory Medicine, 7th Ed.
WHO 2024 Severity Classification — By Hemoglobin (g/dL)
Adults
| Severity | Men (Hb g/dL) | Non-pregnant Women (Hb g/dL) |
|---|---|---|
| Normal | ≥ 13.0 | ≥ 12.0 |
| Mild anemia | 11.0 – 12.9 | 11.0 – 11.9 |
| Moderate anemia | 8.0 – 10.9 | 8.0 – 10.9 |
| Severe anemia | < 8.0 | < 8.0 |
Source: WHO 2024 Haemoglobin Cutoffs Guideline; StatPearls (NCBI Bookshelf, 2026)
Pregnant Women (Trimester-specific)
| Trimester | No Anemia | Mild | Moderate | Severe |
|---|---|---|---|---|
| 1st trimester | ≥ 11.0 | 10.0 – 10.9 | 7.0 – 9.9 | < 7.0 |
| 2nd trimester | ≥ 10.5 | 9.5 – 10.4 | 7.0 – 9.4 | < 7.0 |
| 3rd trimester | ≥ 11.0 | 10.0 – 10.9 | 7.0 – 9.9 | < 7.0 |
Note: Hb physiologically falls in pregnancy due to dilution (plasma volume expands more than RBC mass).
Children (WHO 2024)
| Age Group | No Anemia (g/dL) | Mild (g/dL) | Moderate (g/dL) | Severe (g/dL) |
|---|---|---|---|---|
| 6–23 months | ≥ 10.5 | 9.5 – 10.4 | 7.0 – 9.4 | < 7.0 |
| 24–59 months | ≥ 11.0 | 10.0 – 10.9 | 7.0 – 9.9 | < 7.0 |
| 5–11 years | ≥ 11.5 | 11.0 – 11.4 | 8.0 – 10.9 | < 8.0 |
| 12–14 years (boys & girls) | ≥ 12.0 | 11.0 – 11.9 | 8.0 – 10.9 | < 8.0 |
Clinical Correlation: Symptoms by Hb Level
The severity classification directly predicts symptomatology:
| Hb (g/dL) | Degree | Typical Clinical Features |
|---|---|---|
| 11–13 (men) / 11–12 (women) | Mild | Usually asymptomatic; pallor may be absent; detected incidentally on CBC |
| 8–11 | Moderate | Pallor (conjunctival, palmar); fatigue, exertional dyspnea, palpitations, reduced exercise tolerance; compensatory tachycardia |
| 6–8 | Moderate–Severe | All of above + dyspnea at rest, prominent pallor at all sites, systolic flow murmur (hyperdynamic circulation), headache, dizziness |
| < 6 | Severe / Profound | High-output cardiac failure, angina (even without coronary disease), severe dyspnea, altered sensorium, anasarca in extreme cases; life-threatening |
Physiological Compensation in Anemia
As Hb falls, the body compensates through:
- ↑ Cardiac output — tachycardia, increased stroke volume → hyperdynamic circulation, flow murmur
- ↑ Respiratory rate — to maximize oxygen delivery
- ↑ 2,3-DPG (diphosphoglycerate) in RBCs — shifts oxygen–hemoglobin dissociation curve rightward → more O₂ released to tissues
- Redistribution of blood flow — vital organs (brain, heart) preferentially perfused over skin/muscles
These adaptive mechanisms work well in mild–moderate anemia in healthy individuals but fail in those with pre-existing cardiopulmonary disease. — Robbins & Kumar Basic Pathology
Transfusion Thresholds Based on Hb Severity
Severity classification directly determines transfusion decisions:
| Clinical Context | Transfuse When Hb |
|---|---|
| Stable hospitalized patients (most) | < 7.0 g/dL (restrictive strategy) |
| Pre-existing cardiovascular disease / orthopedic surgery / cardiac surgery | < 8.0 g/dL |
| Active ACS / acute coronary syndromes | Consider at < 10.0 g/dL |
| Symptomatic anemia at any level | Transfuse regardless of absolute value |
Goldman–Cecil Medicine; Tintinalli's Emergency Medicine; Miller's Anesthesia, 10th Ed.
Altitude Adjustment (WHO 2024)
Hb thresholds must be adjusted upward at altitude (higher altitude = higher normal Hb):
| Altitude (metres) | Add to Hb threshold (g/L) |
|---|---|
| 0–499 m | 0 |
| 500–999 m | +4 |
| 1000–1499 m | +8 |
| 1500–1999 m | +11 |
| 2000–2499 m | +14 |
| ≥ 2500 m | +18 and above |
(e.g., at 1500 m altitude, the anemia threshold for adult men becomes 13.0 + 1.1 = 14.1 g/dL)
Summary Box
ANEMIA SEVERITY (Adults)
─────────────────────────────────────────────────────
Mild │ Hb 11.0–12.9 (men) / 11.0–11.9 (women)
│ Usually asymptomatic; found on routine CBC
──────────┼──────────────────────────────────────────
Moderate │ Hb 8.0–10.9
│ Exertional dyspnea, fatigue, pallor, tachycardia
──────────┼──────────────────────────────────────────
Severe │ Hb < 8.0
│ Rest dyspnea, flow murmur, severe pallor
│ Requires urgent treatment / transfusion
──────────┼──────────────────────────────────────────
Profound │ Hb < 6.0
│ High-output CCF, angina, life-threatening
─────────────────────────────────────────────────────
References:
- WHO Guideline on Haemoglobin Cutoffs, 2024 (who.int)
- Tietz Textbook of Laboratory Medicine, 7th Ed.
- Miller's Anesthesia, 10th Ed. — Anemia, p. 3981
- Robbins & Kumar Basic Pathology — Red Cell Disorders
- Goldman–Cecil Medicine — Red Blood Cell Transfusions
- StatPearls: Normal and Abnormal CBC, NCBI 2026
Edema - clinically how will you evaluate
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.