Seizure Types Management Differences
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have rich data from multiple authoritative sources. Let me compile the comprehensive answer.
Seizures: Types, Management, and Differences
What Is a Seizure?
A seizure is a transient occurrence of signs or symptoms due to abnormal excessive or synchronous neuronal activity in the brain. It is not synonymous with epilepsy - epilepsy requires recurrent unprovoked seizures from a chronic underlying process. About 5-10% of the population will have at least one seizure in their lifetime.
- Harrison's Principles of Internal Medicine 22E, p. 3452
ILAE 2017 Classification of Seizure Types
The International League Against Epilepsy (ILAE) 2017 classification is the current standard. It divides seizures into three major onset categories:
| Onset | Description |
|---|---|
| Focal | Originates within networks limited to one hemisphere |
| Generalized | Arises within and rapidly engages bilaterally distributed networks |
| Unknown | Onset cannot be determined |
- Bradley and Daroff's Neurology in Clinical Practice, p. 2233
1. FOCAL ONSET SEIZURES
Focal seizures arise from a neuronal network discretely localized within one brain region or broadly distributed but still within one cerebral hemisphere.
Classification by Awareness
| Type | Features |
|---|---|
| Focal Aware Seizure (FAS) | Awareness fully preserved throughout (old term: "simple partial seizure") |
| Focal Impaired Awareness Seizure (FIAS) | Any alteration of awareness at any point (old term: "complex partial seizure") |
Classification by Onset Type
Motor onset: tonic, clonic, myoclonic, automatisms, hyperkinetic, epileptic spasms
Non-motor onset: sensory (paresthesias, visual phenomena), autonomic (flushing, piloerection), cognitive, emotional (fear, deja vu), behavioral arrest
Key Features of Focal Seizures
-
Jacksonian march: Focal motor seizure starting in restricted region (e.g., fingers) spreading progressively - represents seizure activity spreading over motor cortex
-
Todd's paralysis: Localized paresis for minutes to hours after a focal motor seizure
-
Aura: Subjective experiential event (odors, tastes, rising epigastric sensation, fear, deja vu) - represents a focal seizure without cognitive disturbance preceding FIAS
-
Automatisms: Semi-purposeful, stereotyped movements (lip-smacking, picking, fumbling) common in temporal lobe origin
-
Focal to bilateral tonic-clonic (FBTC): Previously called "secondarily generalized seizure" - focal seizure that evolves into bilateral tonic-clonic activity
-
Harrison's Principles of Internal Medicine 22E, p. 3453-3454
2. GENERALIZED ONSET SEIZURES
Generalized seizures engage bilaterally distributed networks from the start.
Motor Types
| Seizure | Features |
|---|---|
| Tonic-Clonic (GTC) | Sudden loss of consciousness, tonic stiffening then rhythmic clonic jerking, post-ictal confusion (commonest "grand mal") |
| Tonic | Sustained muscle stiffening without clonic phase, often causes falls |
| Clonic | Rhythmic jerking movements only |
| Myoclonic | Brief, shock-like muscle jerks; often bilateral; common in JME (Juvenile Myoclonic Epilepsy) |
| Atonic | Sudden loss of muscle tone ("drop attacks"), high injury risk |
| Epileptic Spasms | Sudden flexion/extension of trunk and limbs; classic in infantile spasms (West syndrome) |
Non-Motor Types (Absence Seizures)
| Type | Features |
|---|---|
| Typical Absence | Abrupt staring, brief behavioral arrest (5-30 sec), no post-ictal confusion, 3-Hz spike-wave on EEG; common in childhood |
| Atypical Absence | Slower onset/offset, often with other features, slower spike-wave (<3 Hz), seen in Lennox-Gastaut |
3. UNKNOWN ONSET SEIZURES
When onset cannot be classified from available information. May be motor, non-motor, or unclassified.
KEY DIFFERENCES: Old vs. New Terminology (1981 vs. 2017 ILAE)
| Old 1981 Term | New 2017 Term |
|---|---|
| Partial seizure | Focal seizure |
| Simple partial seizure | Focal aware seizure (FAS) |
| Complex partial seizure | Focal impaired awareness seizure (FIAS) |
| Secondarily generalized seizure | Focal to bilateral tonic-clonic (FBTC) |
| Localization-related epilepsy | Focal epilepsy |
| Cryptogenic epilepsy | Epilepsy of unknown cause |
| Symptomatic epilepsy | Structural/metabolic epilepsy |
- Bradley and Daroff's Neurology in Clinical Practice, Table 100.1
KEY DIFFERENCES: Focal vs. Generalized Seizures
| Feature | Focal | Generalized |
|---|---|---|
| Onset | One hemisphere | Both hemispheres simultaneously |
| Awareness | May be intact or impaired | Usually impaired (absent in GTC) |
| Aura | Common (represents ictal onset) | None (no focal prodrome) |
| EEG | Focal/unilateral discharge | Bilateral synchronous discharge |
| Post-ictal | Focal deficit (Todd's palsy) possible | Global confusion, fatigue |
| Etiology | Often structural (scar, tumor, dysplasia) | Often genetic/idiopathic |
| Automatisms | Common in temporal lobe origin | Absent (may see automatisms in absence) |
| Duration | Variable | Seconds (absence) to minutes (GTC) |
KEY DIFFERENCES: Absence vs. Tonic-Clonic
| Feature | Absence | Tonic-Clonic (GTC) |
|---|---|---|
| Duration | 5-30 seconds | 1-3 minutes |
| Onset | Abrupt stare, no warning | May have aura (if focal onset) |
| Motor activity | Minimal (subtle eye blinking) | Major convulsions |
| Post-ictal confusion | None - immediate recovery | Yes - prolonged drowsiness |
| Memory | No recollection | No recollection |
| EEG | 3-Hz generalized spike-wave | Polyspike then spike-wave during clonic phase |
| Age | Childhood (4-14 years) | Any age |
| Triggered by | Hyperventilation | Sleep deprivation, alcohol |
MANAGEMENT
Acute Seizure First Aid
- Position patient safely (lateral decubitus to prevent aspiration)
- Protect from injury
- Do NOT restrain, do NOT put anything in the mouth
- Time the seizure
- Call emergency services if >5 minutes or no return to baseline
Status Epilepticus (SE)
Definition: Single seizure ≥5 minutes OR two or more seizures without recovery of consciousness between them.
After 5 minutes, seizures are less likely to spontaneously terminate, less likely to respond to AEDs, and more likely to cause neuronal damage. After 20 minutes: hypotension, hypoxia, metabolic acidosis, hyperthermia, and cardiac dysrhythmias develop.
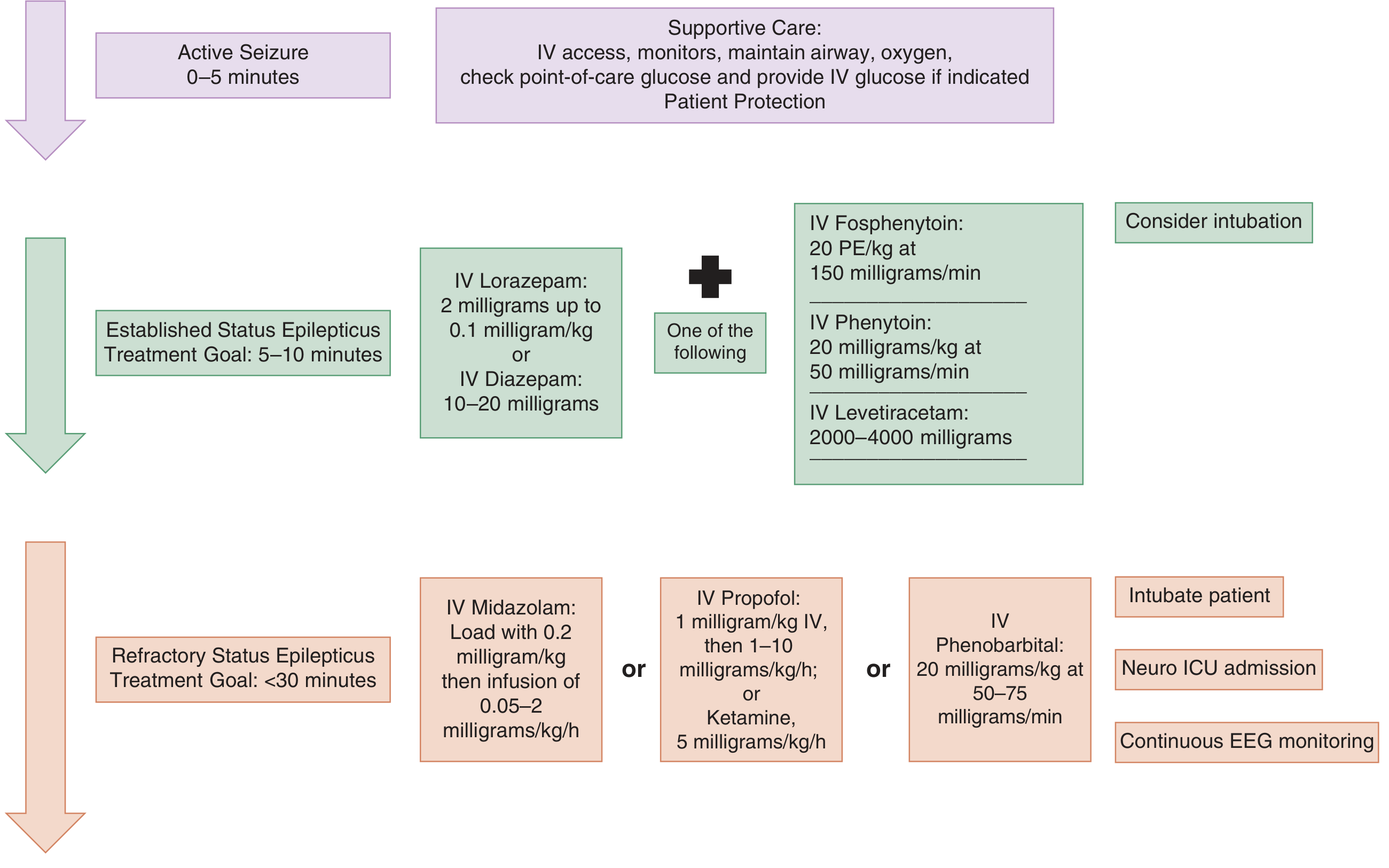
Three-tier treatment approach:
Tier 1 - Active Seizure (0-5 min): Stabilize
- Airway, breathing, circulation
- IV access, O2, cardiac monitor
- Bedside glucose; give IV glucose if hypoglycemic
- Patient protection
Tier 2 - Established SE (5-10 min): Benzodiazepines (First-Line)
- IV Lorazepam 2-4 mg (preferred if IV access available) - onset 3 min, duration 12-24 hours
- IV Diazepam 5-10 mg - onset 2 min, but shorter duration (15-60 min)
- IM Midazolam - preferred if no IV access; non-inferior to IV lorazepam
- Repeat benzodiazepine once if no response
Then add a second-line agent within 20 minutes:
- Fosphenytoin 20 PE/kg at 150 PE/min (preferred over phenytoin - fewer infusion-site reactions)
- Phenytoin 20 mg/kg IV (no faster than 25 mg/min; risk of cardiac depression)
- Levetiracetam 2000-4000 mg IV
- Valproate or Lacosamide - current guidelines do not favor one second-line agent over another
Tier 3 - Refractory SE (<30 min): Anesthetic agents
-
IV Midazolam infusion: 0.2 mg/kg load, then 0.05-2 mg/kg/h
-
IV Propofol: 1 mg/kg, then 1-10 mg/kg/h
-
IV Phenobarbital: 20 mg/kg at 50-75 mg/min
-
Ketamine: 5 mg/kg/h (NMDA antagonist - useful as glutamate receptors upregulate in prolonged SE)
-
Intubation + Neuro ICU + continuous EEG monitoring
-
Tintinalli's Emergency Medicine, p. 1198-1199
Chronic Epilepsy: Antiepileptic Drug (AED) Selection
| Seizure Type | First-Line | Second-Line | Third-Line |
|---|---|---|---|
| Generalized Tonic-Clonic | Valproate, Carbamazepine | Lamotrigine, Oxcarbazepine | Phenytoin |
| Absence | Valproate | Ethosuximide, Levetiracetam, Topiramate | Lamotrigine |
| Myoclonic | Valproate, Levetiracetam | Lamotrigine | Phenobarbital, Clobazam |
| Focal | Carbamazepine, Phenytoin | Valproate, Levetiracetam, Oxcarbazepine | Lamotrigine, Topiramate |
| Infantile Spasms | ACTH, Vigabatrin, Valproate | Valproate | Lamotrigine |
| Lennox-Gastaut | Valproate | Topiramate, Lamotrigine | Levetiracetam |
- Adams and Victor's Principles of Neurology 12E, Table 15-7
Key pharmacology note: Carbamazepine, phenytoin, and oxcarbazepine are sodium channel blockers - effective for focal and GTC seizures but can worsen absence and myoclonic seizures. Valproate is broad-spectrum (all types). Ethosuximide works only for absence (T-type Ca²+ channel blockade).
Special Considerations
- Pregnancy: Levetiracetam and Lamotrigine are the safest options; most AEDs are teratogenic
- Phenytoin kinetics: Nonlinear (zero-order) above 10 mg/mL - small dose increases cause disproportionate toxicity
- Carbamazepine: Auto-induces its own metabolism; doses that control seizures initially may become inadequate after weeks
- Valproate interactions: Displaces phenytoin and phenobarbital from plasma proteins; elevates carbamazepine-epoxide via epoxide hydrolase inhibition
Special Seizure Types
Febrile Seizures
- Age 6 months - 5 years, associated with fever
- Simple: <15 min, generalized, no recurrence within 24h - NOT associated with increased epilepsy risk
- Complex: >15 min, focal features, or multiple within 24h - epilepsy risk 2-5%
Non-Convulsive Status Epilepticus (NCSE)
- No overt convulsions; presents as coma, fluctuating mental status, subtle twitching/eye deviation
- Diagnosis requires EEG
- A prolonged postictal period after a GTC should raise suspicion
Juvenile Myoclonic Epilepsy (JME)
- Adolescence onset; morning myoclonic jerks + GTC seizures on awakening + absence
- Highly responsive to valproate; lifelong treatment usually required
Sources: Harrison's Principles of Internal Medicine 22E | Bradley and Daroff's Neurology in Clinical Practice | Adams and Victor's Principles of Neurology 12E | Tintinalli's Emergency Medicine
Difference between seizure and epilepsy
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I have all the information needed. Here is the clear, comprehensive answer:
Seizure vs. Epilepsy
These two terms are often used interchangeably in everyday language, but they are clinically distinct concepts.
Seizure
"A transient occurrence of signs or symptoms due to abnormal excessive or synchronous neuronal activity in the brain."
- Harrison's Principles of Internal Medicine 22E, p. 3452
A seizure is a single event - a symptom, not a diagnosis. It is the brain's electrical "storm." It tells you something happened, but not why or whether it will happen again.
- About 5-10% of the general population will experience at least one seizure in their lifetime
- A seizure can occur in any person given the right circumstances (fever, drugs, metabolic imbalance)
- Having a seizure does not automatically mean you have epilepsy
Epilepsy
"A disorder of the brain characterized by recurrent unprovoked seizures - at least 2 seizures occurring >24 hours apart, OR 1 unprovoked seizure with ≥60% probability of a second seizure over the next 10 years."
- Frameworks for Internal Medicine
Epilepsy is a chronic condition - a diagnosis, not just an event. It implies an ongoing, underlying predisposition of the brain to generate seizures.
- Affects approximately 1-3% of the population
- It is a clinical phenomenon, not a single disease - many forms and causes exist
- Can be resolved if seizure-free for ≥10 years (without AEDs for the last 5 years)
The Relationship: Seizure → Epilepsy
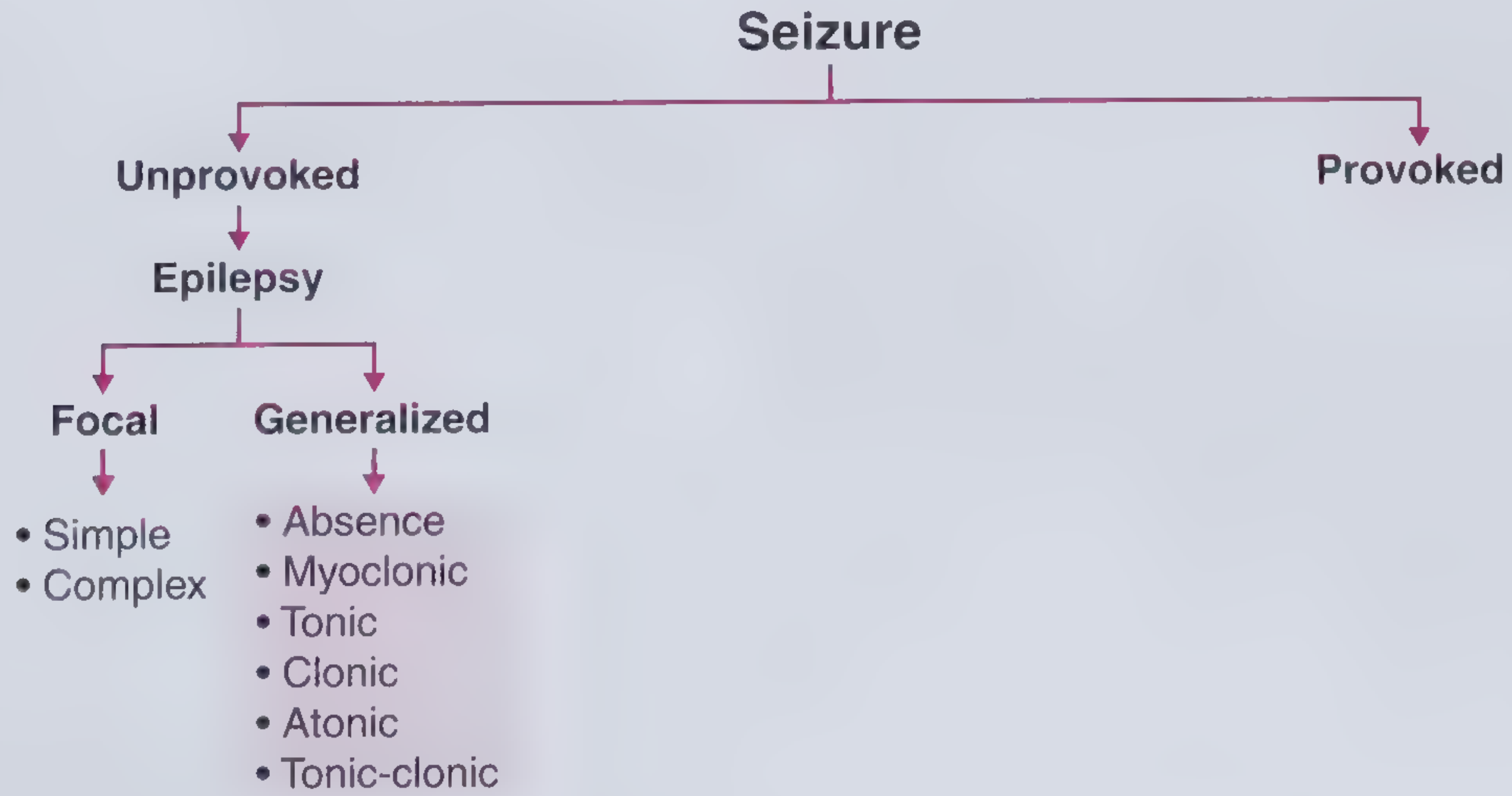
The key bridge concept is whether a seizure is provoked or unprovoked:
| Provoked Seizure | Unprovoked Seizure | |
|---|---|---|
| Definition | Occurs in close temporal relationship with a reversible/temporary precipitant | Occurs without a temporary or reversible cause |
| Also called | Acute symptomatic seizure | Primary seizure |
| Examples of causes | Hypoglycemia, alcohol withdrawal, fever, electrolyte imbalance, drug toxicity, acute stroke | Structural brain lesion, genetic mutation, unknown cause |
| Does it = Epilepsy? | No | Potentially yes (if recurrent or high recurrence risk) |
| AED treatment? | Generally not started | Started after 2nd unprovoked seizure |
- The Washington Manual of Medical Therapeutics
Side-by-Side Comparison
| Feature | Seizure | Epilepsy |
|---|---|---|
| Nature | A single event/symptom | A chronic disorder/diagnosis |
| Number | Can be just one | Requires ≥2 unprovoked, OR 1 with high recurrence risk |
| Cause | Can be provoked (reversible) OR unprovoked | Always unprovoked; underlying chronic process |
| Brain abnormality | Not necessarily permanent | Implies a persistent tendency/predisposition |
| Recurrence risk | After 1st unprovoked seizure: ~40-50% over 2-8 years | After 2nd unprovoked seizure: ~60-90% over 4 years |
| Treatment | Treat the underlying cause (if provoked) | Long-term AED therapy |
| Prognosis | Provoked seizures - good if cause corrected | Variable; many achieve remission; some lifelong |
| Prevalence | 5-10% lifetime | 0.3-0.5% (epilepsy); ~3% lifetime |
The Important Clinical Nuance
A single seizure does NOT equal epilepsy - unless:
- There is an EEG or imaging finding indicating a high probability (≥60%) of recurrence, OR
- The patient has a diagnosed epilepsy syndrome (e.g., Juvenile Myoclonic Epilepsy)
Similarly, a person can have recurrent seizures (e.g., from repeated alcohol withdrawal) without having epilepsy, because those are provoked seizures with a correctable cause.
"A person with a single seizure, or recurrent seizures due to correctable or avoidable circumstances, does not necessarily have epilepsy."
- Harrison's Principles of Internal Medicine 22E
Memory Aid
Seizure = the lightning bolt (the event) Epilepsy = the storm-prone weather pattern (the condition that keeps producing lightning)
Sources: Harrison's Principles of Internal Medicine 22E | Frameworks for Internal Medicine | Neuroanatomy through Clinical Cases 3E | The Washington Manual of Medical Therapeutics
Aura in epilepsy
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
I have comprehensive material. Here is the complete answer:
Aura in Epilepsy
Definition
"An epileptic aura is a simple partial (focal aware) seizure manifesting as sensory, autonomic, or psychic symptoms."
- The Washington Manual of Medical Therapeutics
An aura is not merely a warning - it IS a seizure. It represents the initial phase of a focal seizure in which abnormal electrical discharge is limited to one cortical region, and the patient remains conscious and aware throughout. In some cases, the aura may constitute the entire epileptic attack with no further progression.
- Adams and Victor's Principles of Neurology 12E, p. 338
Aura vs. Prodrome - An Important Distinction
These two terms are often confused:
| Feature | Aura | Prodrome |
|---|---|---|
| Nature | IS the seizure (focal aware seizure) | A pre-seizure feeling before the seizure starts |
| Timing | Seconds to minutes before ictal spread | Hours to days before a seizure |
| Mechanism | Focal cortical electrical discharge | Non-epileptic, possibly hormonal/autonomic changes |
| Consciousness | Fully preserved | Fully preserved |
| Examples | Rising epigastric sensation, flashing lights, déjà vu | Irritability, headache, mood change, anxiety |
| Localizing value | Yes - points to seizure focus | No |
- The Washington Manual of Medical Therapeutics
Clinical Significance of the Aura
- It is a seizure - not just a warning signal
- It has localizing value - the type of aura identifies which cortical region the seizure originates from (see table below)
- It can be the sole manifestation - if the discharge stays contained, the aura is the entire event
- It distinguishes focal from generalized onset - generalized tonic-clonic seizures have no aura (bilateral onset from the start); identifying a preceding aura reclassifies a seizure as focal to bilateral tonic-clonic (FBTC)
"Often, the focal onset is not clinically evident and may be established only through careful EEG analysis. Nonetheless, distinguishing between these two entities is extremely important, because there are substantial differences in the evaluation and treatment."
- Harrison's Principles of Internal Medicine 22E, p. 3453
Types of Aura and Their Cortical Localization
| Aura Type | Symptoms | Seizure Origin |
|---|---|---|
| Epigastric / Visceral | Rising sensation from abdomen to chest/throat (most common aura) | Mesial temporal lobe (amygdala, hippocampus) |
| Psychic / Experiential | Déjà vu, jamais vu, depersonalization, dreamy state, autoscopy | Temporal lobe (hippocampus, parahippocampal gyrus) |
| Emotional | Fear, anxiety (most common emotion), rarely anger, ecstasy | Amygdala / mesial temporal lobe |
| Olfactory | Unpleasant, unidentifiable burning or rotten smell | Uncus / mesial temporal lobe ("uncinate fits") |
| Gustatory | Bitter or metallic taste | Frontoparietal (supra-sylvian) cortex or uncal region |
| Auditory | Simple sounds (buzzing, ringing) or complex voices | Superior temporal gyrus (Heschl's gyrus) |
| Visual | Unformed flashes, colors, zigzag lines | Occipital cortex (primary visual cortex) |
| Visual (formed) | Complex formed hallucinations (faces, scenes) | Temporal-occipital association cortex |
| Somatosensory | Focal tingling, numbness, paresthesias | Contralateral parietal lobe (somatosensory cortex) |
| Autonomic | Flushing, sweating, piloerection, palpitations | Insular cortex / temporal lobe |
| Vertiginous | Sense of spinning or falling | Posterior temporal / parietal cortex |
| Visual distortion | Micropsia (objects shrink), macropsia (objects grow), palinopsia | Temporal-occipital junction |
- Harrison's Principles of Internal Medicine 22E, p. 3453
- Adams and Victor's Principles of Neurology 12E, p. 338-339
The Temporal Lobe Aura - Most Common and Most Varied
Temporal lobe seizures produce the richest range of auras, including:
- Epigastric rising sensation - the most characteristic and common
- Déjà vu - intense feeling of familiarity in an unfamiliar situation
- Jamais vu - strangeness or unfamiliarity in a previously known place
- Autoscopy - the patient views themselves as an external observer
- Memory fragments - vivid recollection of old memories or scenes
- Fear/anxiety - the most common affective aura
- Olfactory hallucinations - typically unpleasant, unidentifiable smells
"Each of these subjective psychic states may constitute the entire seizure or some combination may occur and immediately precede a period of altered awareness. These auras represent electrical seizures and have the same localizing significance as motor convulsions do for the frontal cortex."
- Adams and Victor's Principles of Neurology 12E, p. 339
What Happens After the Aura?
The aura may be followed by:
- Nothing - aura is the entire seizure (focal aware seizure only)
- Focal impaired awareness seizure (FIAS) - consciousness becomes impaired; automatisms (lip smacking, picking, fumbling) appear
- Focal to bilateral tonic-clonic seizure - seizure spreads to both hemispheres; full convulsion follows
The transition is often marked by a motionless stare signaling the onset of impaired awareness.
Key Points Summary
| Point | Detail |
|---|---|
| An aura IS a seizure | Focal aware seizure - not merely a warning |
| Consciousness | Fully preserved during the aura |
| Memory | Patient remembers the aura (unlike the ictal phase of FIAS) |
| Generalized seizures | Have NO aura (no focal onset) |
| Clinical value | Localizes seizure focus; critical for surgical planning |
| Stereotypy | Each patient's aura is typically identical each time |
Sources: Harrison's Principles of Internal Medicine 22E | Adams and Victor's Principles of Neurology 12E | The Washington Manual of Medical Therapeutics | Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.