Ventricular tachycardia with pulse management and workups
Reading File
Finding Sources
Searching PubMed
"ventricular tachycardia" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
I now have rich, authoritative content from multiple textbooks. Let me compile a comprehensive answer.
Ventricular Tachycardia with Pulse: Management and Workup
Definition and Classification
Ventricular tachycardia (VT) is defined as 3 or more consecutive ventricular depolarizations at a rate >100 beats/min. Classification matters clinically:
| Feature | Description |
|---|---|
| Sustained VT | Episodes lasting >30 seconds or requiring intervention |
| Nonsustained VT | Short runs (<30 sec) that terminate spontaneously |
| Monomorphic VT | Consistent QRS morphology beat-to-beat; most common (~70% of cases); rate typically 150-200 bpm |
| Polymorphic VT | Varying QRS morphology; suggests more severe underlying disease |
| Hemodynamically stable VT | Patient has pulse, is conscious, tolerating the rhythm |
| Hemodynamically unstable VT | Pulse present but signs of hemodynamic compromise (hypotension, altered mental status, chest pain, pulmonary edema) |
- Tintinalli's Emergency Medicine, p. 157
- Rosen's Emergency Medicine, p. 1061
ECG Workup - Diagnosing VT
The 12-lead ECG is the cornerstone of workup. VT must be differentiated from SVT with aberrant conduction (both produce wide-complex tachycardia, QRS >100-120 ms, rate >100 bpm).
ECG Features Favoring VT
The following five features on ECG favor VT over SVT with aberrancy:
- AV dissociation - Atria and ventricles beat independently; P waves are "marching through" QRS complexes. Present in only ~10% but highly specific for VT when seen.
- Capture beats - An atrial impulse occasionally conducts through the AV node during VT, producing a narrow QRS complex - pathognomonic for VT.
- Fusion beats - A conducted sinus beat fuses with a ventricular beat, creating an intermediate QRS morphology - also pathognomonic for VT.
- QRS duration >160 ms - Extreme QRS widening makes SVT with aberrancy very unlikely.
- Concordance - All precordial leads (V1-V6) show the same deflection direction (all positive or all negative), strongly suggesting VT.
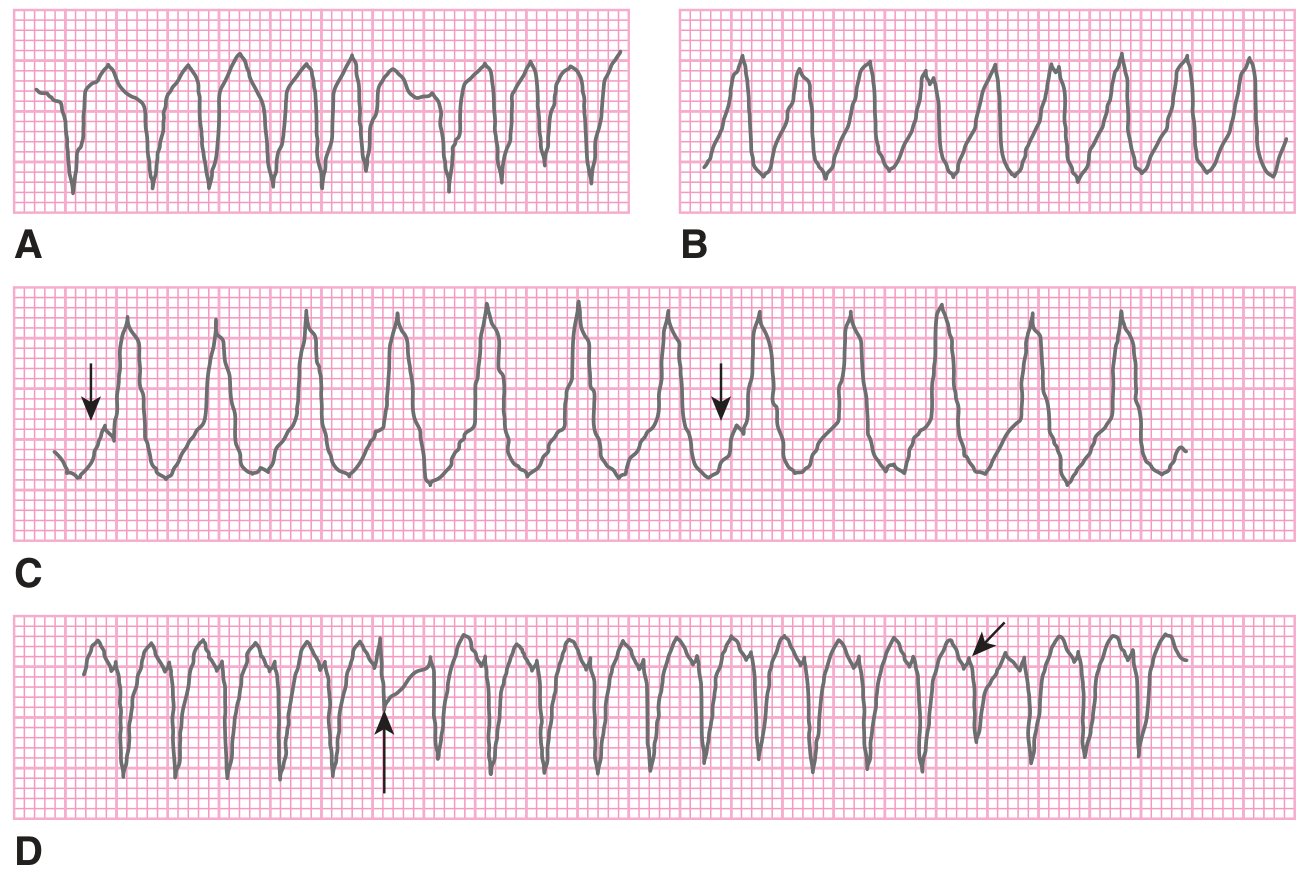
FIGURE: ECG considerations in the diagnosis of VT - A. Regular monomorphic VT; B. Irregular VT; C. AV dissociation; D. Capture and fusion beats (from Tintinalli's Emergency Medicine)
Brugada ECG Criteria for VT (Lead V1 or V2 vs V6)
- R wave in V1/V2 lasting >0.03 s
-
0.07 seconds from QRS onset to nadir of S wave
- Notched or slurred S wave descending limb
- QR or QS pattern in V6
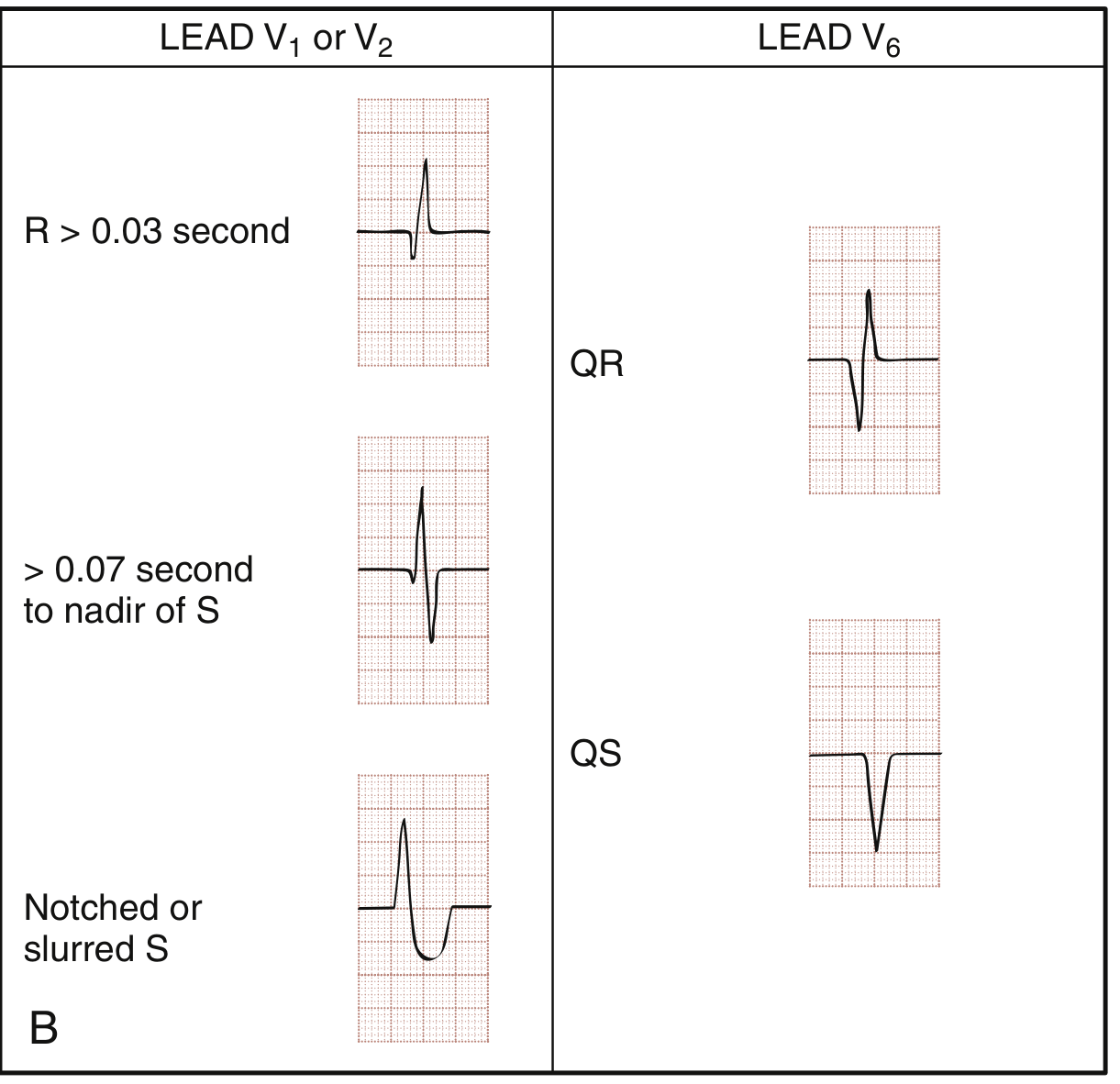
FIGURE: Brugada criteria ECG findings distinguishing VT from SVT with aberrancy (from Rosen's Emergency Medicine)
Important caveat: VT cannot be reliably differentiated from SVT with aberrancy based on clinical symptoms or vital signs alone - even hemodynamically stable patients can have VT.
- Tintinalli's Emergency Medicine, pp. 156-158
Clinical Workup
Initial Assessment (Simultaneous with Resuscitation if Needed)
| Study | Purpose |
|---|---|
| 12-lead ECG | Confirm VT; assess morphology; look for ischemia, prior MI, QT interval |
| Continuous cardiac monitoring | Ongoing rhythm tracking |
| Pulse oximetry / ABG | Hypoxia/alkalosis exacerbate ventricular ectopy |
| Basic metabolic panel | Hyperkalemia, hypokalemia worsen VT propensity |
| Magnesium level | Hypomagnesemia precipitates polymorphic VT and TdP |
| Cardiac troponin | Rule out acute MI as precipitant |
| BNP/NT-proBNP | Assess for decompensated heart failure |
| Chest X-ray | Cardiomegaly, pulmonary edema |
| Echocardiogram | Assess structural heart disease, EF, wall motion abnormalities |
| Drug levels / toxicology | Digoxin toxicity, QT-prolonging drugs, stimulant drugs |
Key Precipitating Causes to Identify and Correct
- Hypokalemia, hypomagnesemia, other electrolyte disturbances
- Hypoxia or alkalosis
- Acute myocardial ischemia or infarction
- QT-prolonging medications (class IA, IC, III antiarrhythmics; many others - see CredibleMeds/torsades.org)
- Heart failure decompensation
- Drug toxicity (digoxin, stimulants)
Prompt identification and reversal of precipitating causes is the most important factor in preventing early VT recurrence.
- Goldman-Cecil Medicine, p. 590
- Tintinalli's Emergency Medicine, p. 157
Management Algorithm
Step 1: Is the Patient Pulseless?
- Pulseless VT = cardiac arrest - Treat as VF: unsynchronized defibrillation, CPR, ACLS protocol. This is NOT covered in "VT with pulse."
Step 2: VT with Pulse - Hemodynamically Stable or Unstable?
Signs of hemodynamic instability:
- Hypotension / shock
- Altered mental status
- Ongoing chest pain / ischemia
- Acute pulmonary edema
- Signs of hypoperfusion
Hemodynamically UNSTABLE VT with Pulse
Synchronized cardioversion is the treatment of choice.
-
Starting energy: 100 J biphasic (preferred)
-
If unsuccessful, escalate to 200 J biphasic or up to 360 J monophasic
-
Administer procedural sedation/analgesia if the patient's clinical status allows (e.g., midazolam + fentanyl or ketamine)
-
Ensure "synchronized" mode is selected (not defibrillation mode) to avoid delivering shock during T wave, which could precipitate VF
-
Rosen's Emergency Medicine, p. 1062
-
Tintinalli's Emergency Medicine, p. 157
Hemodynamically STABLE VT with Pulse
Pharmacologic therapy is first-line. Three main agents:
1. Procainamide (Preferred)
- Dose: 20-50 mg/min IV infusion; maximum total 17-18 mg/kg (or up to 1000 mg over 20 minutes), or until VT terminates, QRS widens >50%, or hypotension occurs
- Mechanism: Class IA antiarrhythmic (Na+ channel blockade)
- Evidence: Randomized trial data show procainamide is superior to amiodarone for promptly terminating wide-complex tachycardia with fewer adverse effects
- Key disadvantage: Relatively slow infusion required due to hypotension risk; must be given slowly
- Contraindications: QT prolongation, structural heart disease with severe LV dysfunction (risk of proarrhythmia), known sensitivity
2. Amiodarone (Alternative / Second-Line for acute conversion)
- Dose: 150 mg IV over 10 minutes (some sources: 3-5 mg/kg over 20 minutes, commonly 250-350 mg); can repeat; followed by infusion of 1 mg/min for 6 hours, then 0.5 mg/min
- Mechanism: Class III antiarrhythmic with Class I, II, IV properties
- Note: More effective for preventing recurrence after sinus rhythm is restored (particularly at slower heart rates), rather than acute termination. Reported success rates of up to 90% for acute VT termination.
- Advantage: Can be used in structural heart disease / heart failure
3. Lidocaine (Alternative)
- Dose: 1.0-1.5 mg/kg IV bolus, up to 3 mg/kg maximum, followed by continuous infusion (2-4 mg/min)
- Mechanism: Class IB antiarrhythmic (Na+ channel blockade; more efficacious at faster heart rates)
- Note: Effective for termination but not for preventing recurrences, except in the context of acute ischemia. Similar success rates to amiodarone in some studies.
4. Magnesium Sulfate (for polymorphic VT/TdP)
- Dose: 1-2 g IV over 5-20 minutes
- Indication: Polymorphic VT, known hypomagnesemia, QT prolongation, or torsades de pointes
- Note: Class IA/IC drugs are contraindicated in torsades de pointes
Summary: Drug Dosing Table
| Drug | Dose | Notes |
|---|---|---|
| Procainamide | 20-50 mg/min IV, max 17-18 mg/kg or 1000 mg | Preferred; slow due to hypotension risk |
| Amiodarone | 150 mg IV over 10 min; repeat PRN | Better for preventing recurrence |
| Lidocaine | 1.0-1.5 mg/kg IV bolus (max 3 mg/kg), then infusion | Useful in acute ischemia |
| Magnesium | 1-2 g IV over 5-20 min | For polymorphic VT / TdP |
- Rosen's Emergency Medicine, p. 1062
- Tintinalli's Emergency Medicine, p. 157
- Goldman-Cecil Medicine, p. 590
If Stable VT Does Not Respond to Pharmacotherapy
- Escalate to synchronized cardioversion
- Obtain cardiology consult - unusual forms of VT may require electrophysiologic evaluation
- Consider whether the rhythm is truly VT vs SVT with aberrancy; avoid IV calcium channel blockers or adenosine in suspected VT (verapamil can cause hemodynamic collapse in true VT)
Special Scenario: Torsades de Pointes (TdP)
TdP is a polymorphic VT with rate >200 bpm, undulating QRS axis ("twisting of the points"), paroxysms <90 seconds, and occurs in the setting of prolonged QT interval.
| Feature | Management |
|---|---|
| Correct electrolytes | Replete K+ to >4 mEq/L, Mg2+ to >2 mEq/L |
| Magnesium sulfate | 1-2 g IV - first-line for TdP |
| Stop offending drugs | Remove all QT-prolonging agents |
| Increase heart rate | Isoproterenol infusion OR overdrive pacing to shorten QT and suppress TdP; transcutaneous or transvenous pacing at 90-110 bpm |
| Avoid class IA/IC drugs | These worsen QT prolongation and TdP |
| Unstable TdP | Unsynchronized cardioversion if hemodynamically compromised |
- Rosen's Emergency Medicine, p. 1062-1063
- Tintinalli's Emergency Medicine, p. 157
Electrical Storm
Defined as recurrent VT/VF requiring repeated defibrillation (typically >3 episodes in 24 hours). Management includes:
- IV beta-blocker (esmolol: 500 mcg/kg load over 1 min, then 50-200 mcg/kg/min infusion)
- IV amiodarone (0.5-1.0 mg/min) or lidocaine (2-4 mg/min)
- Correct precipitating ischemia (urgent revascularization if ischemia-driven)
- Intra-aortic balloon pump if needed
- Catheter ablation (reduces recurrence and may improve survival)
- Goldman-Cecil Medicine, p. 590
Outpatient / Long-Term Management After VT
| Intervention | Indication |
|---|---|
| ICD (implantable cardioverter-defibrillator) | VT with structural heart disease; prior MI with EF <35%; nonischemic cardiomyopathy with EF <35% |
| Catheter ablation (RF or cryoablation) | Recurrent VT refractory to medications; idiopathic VT; VT electrical storm |
| Beta-blockers | All structural heart disease patients; also for idiopathic VT (RVOT) |
| Antiarrhythmic drugs (amiodarone, sotalol) | Adjunct to ICD; reduce ICD shocks |
| Treat underlying cause | Revascularization for ischemia; optimize heart failure management |
Key Points for Clinical Practice
- Hemodynamic instability (not the diagnosis of VT) is the primary indication for immediate electrical cardioversion.
- Never give IV verapamil to a patient with wide-complex tachycardia unless VT has been definitively excluded - it can precipitate hemodynamic collapse.
- Procainamide is preferred over amiodarone for acute termination of stable VT based on randomized data.
- Amiodarone is preferred over lidocaine for preventing VT recurrence after restoration of sinus rhythm.
- Always look for and correct reversible causes: electrolytes (K+, Mg2+), ischemia, drugs, hypoxia.
- Cardiology consult is indicated for all patients with VT, especially those refractory to initial therapy.
Recent guideline update: The 2025 AHA ACLS Guidelines (PMID 41122884, Circulation 2025) include updated guidance on VT management in the context of adult advanced life support - consult for the latest ACLS-specific protocol details.
Sources: Rosen's Emergency Medicine | Tintinalli's Emergency Medicine | Goldman-Cecil Medicine | Braunwald's Heart Disease | AHA ACLS 2025 Guidelines (PMID 41122884)
This is a shared conversation. Sign in to Orris to start your own chat.