Cleft palate
Reading File
Finding Sources
Searching PubMed
"cleft palate"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have rich content from multiple textbooks. Let me compile the comprehensive answer.
Cleft Palate
A cleft palate is a congenital midline defect of the palate resulting from failure of the lateral palatine processes (palatal shelves) to fuse during embryonic development. It is one of the most common craniofacial birth defects.
Epidemiology
-
Cleft lip with or without cleft palate: ~1 in 1,000 births; more common in males (60-80% of cases)
-
Cleft palate alone (without cleft lip): ~1 in 2,500 births; more common in females
-
~7,000 neonates affected per year in the United States
-
Frequency varies widely among ethnic groups
-
The Developing Human, Clinically Oriented Embryology, p. 537-543
Embryology
The palate forms in two parts:
- Primary palate (anterior, pre-incisive fossa): derived from merging of the medial nasal prominences to form the median palatal process
- Secondary palate (posterior, post-incisive fossa): formed by the lateral palatine processes (palatal shelves), which initially project vertically beside the developing tongue, then elevate to a horizontal position and fuse with each other, the nasal septum, and the primary palate
Cleft palate occurs when the lateral palatine processes fail to meet or fuse. Contributing factors include:
- Width of the stomodeum
- Reduced mobility of the lateral palatine processes
- Altered focal degeneration of the palatal epithelium at fusion sites
- Multifactorial inheritance (genetic + environmental)
The incisive fossa is the anatomical landmark separating anterior from posterior cleft defects.
- The Developing Human, p. 540-544
Classification
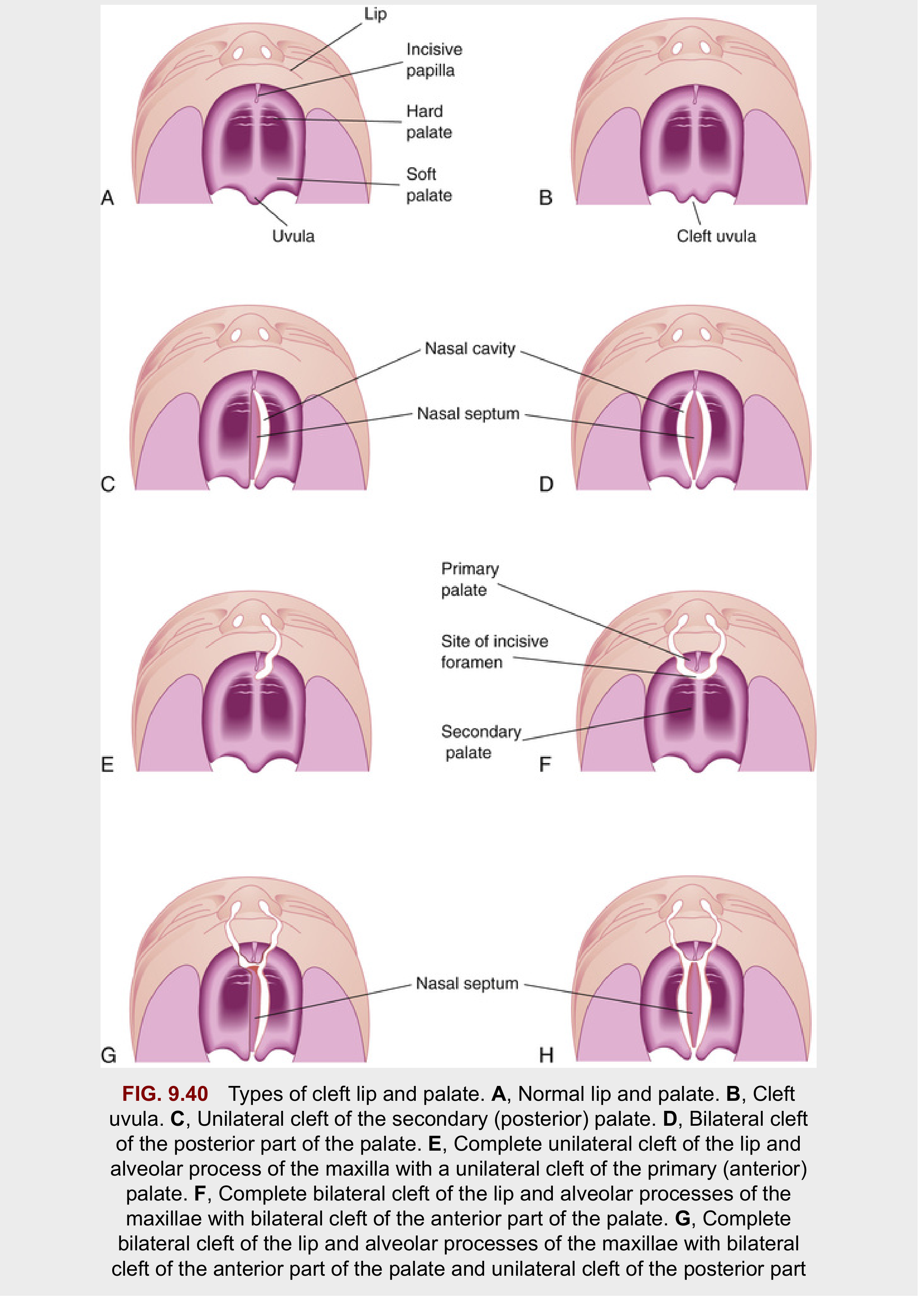
Types of cleft palate (from The Developing Human). A = normal; B = cleft uvula; C = unilateral secondary palate cleft; D = bilateral posterior palate cleft; E-H = progressively severe combined clefts.
| Type | Location | Cause |
|---|---|---|
| Cleft uvula | Uvula only | Mildest form; "fishtail" appearance |
| Cleft of posterior palate | Posterior to incisive fossa | Failure of lateral palatine processes to fuse with each other and nasal septum |
| Cleft of anterior palate | Anterior to incisive fossa | Failure to fuse with primary palate |
| Complete cleft | Entire palate to incisive fossa | Combined failure |
| Submucous cleft palate (SMCP) | Intact mucosa but underlying muscle/bone dehiscence | Abnormal muscle orientation with intact overlying mucosa |
SMCP classic triad: bifid uvula + zona pellucida (hyperlucent midline line on soft palate) + notch at posterior hard palate midline.
Clinical photograph

Infant with unilateral cleft lip and palate (The Developing Human, p. 539)
Anatomy and Pathophysiology
Five muscle pairs contribute to the soft palate. The key abnormalities in cleft palate are:
Levator veli palatini (LVP):
- Normal: transverse orientation, creates a muscular sling for the velum - the principal structure for nasopharyngeal closure during speech and swallowing
- In cleft: runs in an abnormal anterior-posterior direction, attaching to the posterior aspect of the hard palate instead of forming a midline sling
Tensor veli palatini (TVP):
- Normally dilates the Eustachian tube and supports the soft palate
- In cleft: thinner, abnormal insertion into the anterior portion of the levator - unable to open the Eustachian tube, leading to chronic middle ear disease
Musculus uvulae:
-
Increases midline bulk of posterior soft palate during speech
-
Deficiency (as in SMCP) causes velopharyngeal insufficiency (VPI)
-
K.J. Lee's Essential Otolaryngology, p. 979-980; Cummings Otolaryngology, p. 3605
Associated Conditions and Complications
| Problem | Mechanism |
|---|---|
| Feeding difficulties | Communication between oral and nasal cavities; inability to generate suction |
| Otitis media with effusion | TVP dysfunction → Eustachian tube cannot open → chronic middle ear fluid |
| Velopharyngeal insufficiency (VPI) | Disrupted LVP sling → hypernasal speech, nasal regurgitation |
| Speech and language delay | VPI + abnormal resonance |
| Dental/orthodontic problems | Maxillary arch abnormalities, missing/malformed teeth |
| Midface growth retardation | Inherent growth deficiency + potentially surgery-related |
| Pierre Robin sequence | Cleft palate + micrognathia + glossoptosis; airway risk |
Associated syndromes include velocardiofacial syndrome (22q11 deletion), Stickler syndrome, van der Woude syndrome, and many others - cleft palate may be part of >400 syndromes.
Management - Multidisciplinary Team
Optimal management requires a cleft team including: pediatrician, plastic/craniofacial surgeon, otolaryngologist, speech-language pathologist, orthodontist, dentist, audiologist, geneticist, social worker, and psychologist.
Presurgical Management
- Feeding: Specialized nipples (Haberman feeder, Mead Johnson cleft palate nurser); infants are usually fed upright; breastfeeding is difficult but not impossible
- Lip taping: Narrows the cleft gap prior to definitive repair; reduces tension at closure
- Nasoalveolar molding (NAM): Palatal appliance modified over weeks to narrow the cleft and reshape nasal cartilage; most useful for wide unilateral or bilateral clefts; followed by nostril posts to reposition alar cartilages and elongate the columella
- Ear tubes (grommets): Often placed at the time of palatoplasty due to near-universal otitis media with effusion
Surgical Repair - Timing
The timing of palatoplasty is a balance between two competing risks:
| Early repair (< 12 months) | Late repair (> 18 months) |
|---|---|
| Better speech outcomes | Less midface growth inhibition |
| Higher risk of maxillary growth retardation | Higher rate of articulation errors and VPI |
-
Standard in the USA: repair before 18 months; most done between 6-16 months
-
Dorf and Curtin showed 10% vs. 86% articulation error rates for repair before vs. after 1 year
-
Most surgeons target ~12 months of age
-
Some centers use a staged approach: early soft palate repair + later hard palate closure, to minimize midface growth restriction
-
K.J. Lee's Essential Otolaryngology, p. 980; Cummings Otolaryngology, p. 3607
Palatoplasty Techniques
Goals of all techniques:
- Separate nasal from oral cavity
- Restore a functional velopharyngeal valve for speech and swallowing
- Preserve midface growth
- Reconstruct the levator muscle sling (intravelar veloplasty)
| Technique | Description | Best For |
|---|---|---|
| Two-flap (Bardach) palatoplasty with intravelar veloplasty | Two mucoperiosteal flaps raised on greater palatine vessels; soft palatal muscles released from hard palate; nasal layer then muscle sling then oral layer closed | Widely used for all palatal clefts |
| Double-opposing Z-plasty (Furlow palatoplasty) | Opposing Z-plasty incisions on oral and nasal layers transpose myomucosal flaps; reorients levator and lengthens palate | Soft palate clefts, SMCP, also combined with other techniques |
| Von Langenbeck | Bipedicled mucoperiosteal flaps, no pushback | Narrower clefts |
| V-Y pushback (Veau-Wardill-Kilner) | Pushes palatal flaps posteriorly; lengthens palate | When more palatal length needed |
| Schweckendiek (primary veloplasty) | Soft palate only initially; hard palate closed later | Staged approach centers |
Cummings Otolaryngology, p. 3608; K.J. Lee's Essential Otolaryngology, p. 980-981
Postoperative Care
- Arm restraints to prevent finger insertion into the mouth
- Soft/liquid diet for 2-3 weeks
- Pain management
- Monitor for wound dehiscence and airway issues
- Pierre Robin patients: pre-planned airway management with anesthesiology
Secondary Procedures
- Velopharyngeal insufficiency: If VPI persists after palatoplasty, options include pharyngeal flap surgery or sphincter pharyngoplasty
- Alveolar bone grafting: Typically at age 7-9 (mixed dentition), to provide bone for canine tooth eruption
- Orthognathic surgery: Le Fort I osteotomy for significant midface retrusion, typically after skeletal maturity (~17-18 years)
- Revision rhinoplasty and lip revision: For cosmetic refinement
- Orthodontics: Throughout childhood and adolescence
Genetics and Etiology
- Multifactorial inheritance (genetic + environmental) accounts for most non-syndromic cases
- IRF6 gene (interferon regulatory factor 6) is involved in isolated cleft formation
- Environmental risk factors: maternal smoking, alcohol, folate deficiency, anticonvulsants (phenytoin, valproate), corticosteroids, retinoids
- Recurrence risk in a family with one affected child: ~4% for subsequent children
Submucous Cleft Palate
A special variant where the overlying mucosa is intact but:
- The levator and other palatal muscles are oriented anterior-posteriorly (not transversely)
- There is a bony defect in the hard palate
- Classic triad: bifid uvula + zona pellucida + posterior hard palate notch
Management: monitor closely; surgery only if evidence of feeding problems, otologic disease, or VPI.
- K.J. Lee's Essential Otolaryngology, p. 980; Cummings Otolaryngology, p. 3609
Recent Evidence (2024-2026)
- A 2025 systematic review and meta-analysis (PMID 40394284) examined enhanced recovery after surgery (ERAS) protocols for pediatric cleft lip/palate surgery, supporting their use to optimize perioperative management.
- A 2026 umbrella review (PMID 42251739) examined the emerging role of artificial intelligence in cleft diagnosis and detection.
- A 2026 systematic review (PMID 42107941) analyzed the effectiveness of different surgical methods for cleft palate repair - these do not contradict established guidelines but continue to refine technique selection.
Sources: The Developing Human: Clinically Oriented Embryology; K.J. Lee's Essential Otolaryngology; Cummings Otolaryngology - Head and Neck Surgery; Bailey and Love's Short Practice of Surgery.
This is a shared conversation. Sign in to Orris to start your own chat.