Signs and symptoms of insulin resistance
Reading File
Finding Sources
Searching the Web
signs and symptoms of insulin resistance clinical features
Searching PubMed
"insulin resistance" AND "signs symptoms" AND "clinical features"
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have excellent, comprehensive information from Harrison's, Robbins, Goldman-Cecil, Fitzpatrick's, and web sources. Let me compile the full answer.
Signs and Symptoms of Insulin Resistance
Insulin resistance is defined as the failure of target tissues (liver, skeletal muscle, adipose tissue) to respond normally to insulin. Many people with insulin resistance are initially asymptomatic because the pancreas compensates with increased insulin secretion. Signs and symptoms emerge as the condition progresses or when compensatory hyperinsulinemia itself drives pathological changes.
Pathophysiology at a Glance
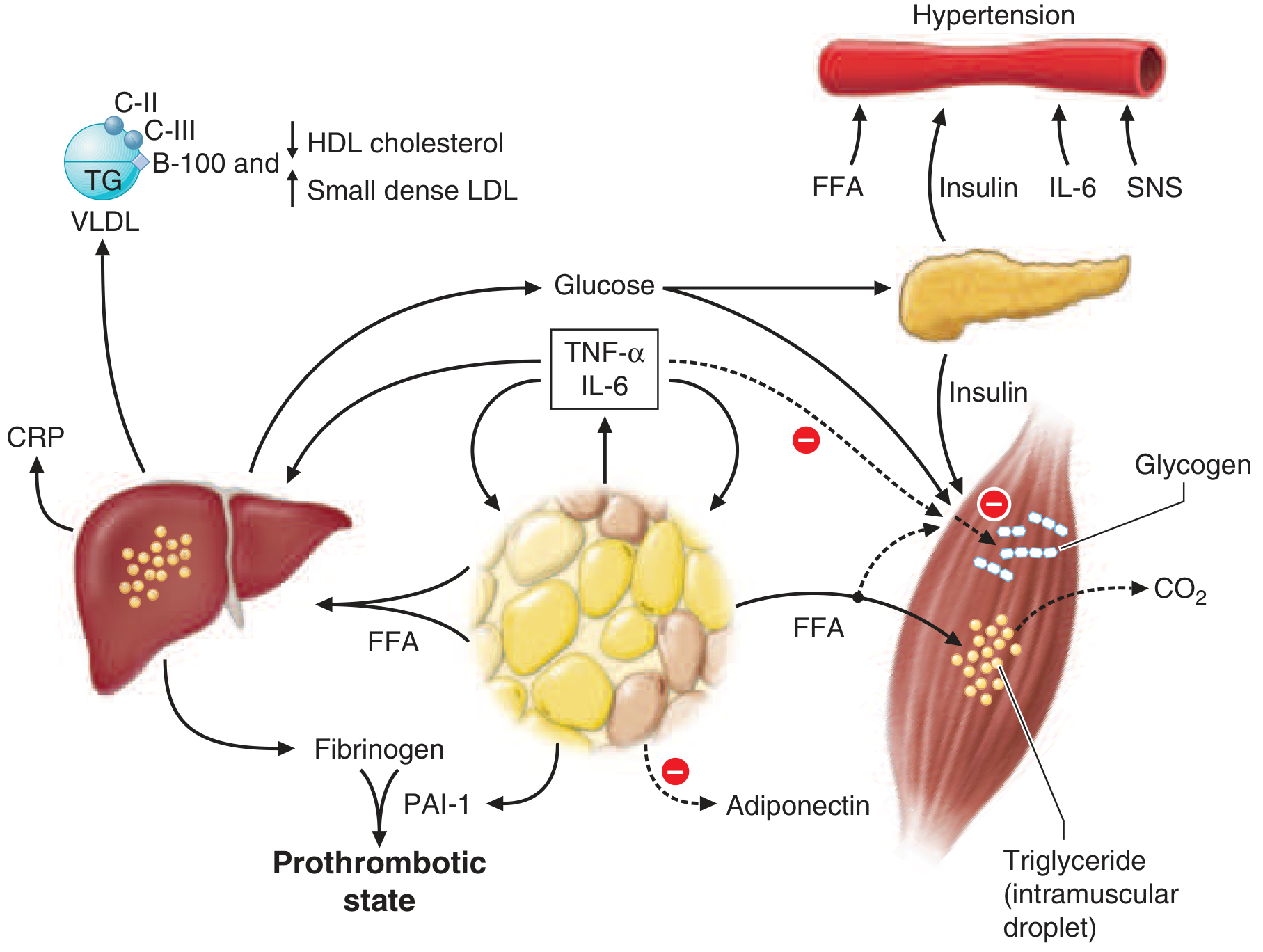
Expanded adipose tissue releases excess free fatty acids (FFAs), leading to hepatic VLDL overproduction, impaired muscle glucose uptake, hyperinsulinemia, and downstream effects on blood pressure, coagulation, and inflammation. - Harrison's Principles of Internal Medicine 22E
1. Skin Signs (Often the Earliest Visible Clues)
Acanthosis nigricans is the hallmark cutaneous marker of insulin resistance and hyperinsulinemia:
- Symmetric, hyperpigmented, hyperkeratotic plaques with a velvety texture on intertriginous skin (neck, axillae, groin, antecubital fossae, knuckles)
- Skin appears dark, dirty, or thickened
- Caused by hyperinsulinemia activating IGF-1 receptors on keratinocytes and fibroblasts, stimulating their proliferation
- More common and more strongly associated with benign (metabolic) forms in individuals with darker skin pigmentation and obesity
Skin tags (acrochordons) - small, soft, pedunculated growths, especially around the neck and axillae, commonly accompany acanthosis nigricans in insulin-resistant states.
- Fitzpatrick's Dermatology, Acanthosis Nigricans section; DermNet NZ
2. Metabolic / Laboratory Signs
These are often detected on routine blood work before overt symptoms develop:
| Feature | Mechanism |
|---|---|
| Fasting hyperinsulinemia | Compensatory pancreatic beta-cell response |
| Impaired fasting glucose / prediabetes | Failure of hepatic glucose suppression + reduced muscle uptake |
| Hypertriglyceridemia | FFA flux drives hepatic VLDL overproduction; excellent marker of IR state |
| Low HDL cholesterol | Altered HDL composition; small, dense HDL cleared more rapidly |
| Small, dense LDL particles | Associated with triglycerides >180 mg/dL; more atherogenic |
| Hyperuricemia | Insulin resistance impairs renal uric acid excretion |
| Elevated CRP / inflammatory markers | Expanded adipose tissue secretes TNF-α, IL-6, resistin |
| Reduced adiponectin | Adiponectin production falls with increasing adiposity and IR |
- Harrison's Principles of Internal Medicine 22E, Chapter 420
3. Cardiovascular / Hemodynamic Features
- Hypertension: Hyperinsulinemia increases renal sodium reabsorption and sympathetic nervous system activity. The normal vasodilatory (nitric oxide-mediated) effect of insulin is lost, but the pro-hypertensive effects are preserved, creating a net pressor state.
- Endothelial dysfunction: Imbalance between nitric oxide production and endothelin-1 secretion leads to reduced vascular flow.
- Prothrombotic state: Elevated fibrinogen and plasminogen activator inhibitor-1 (PAI-1) from hepatocytes and adipocytes.
- Harrison's Principles of Internal Medicine 22E
4. Features of Overt Hyperglycemia (When Beta-Cell Compensation Fails)
When the pancreas can no longer compensate, insulin resistance progresses to prediabetes and then type 2 diabetes mellitus, with symptoms of hyperglycemia:
- Polyuria (frequent urination)
- Polydipsia (increased thirst)
- Polyphagia (increased hunger)
- Unexplained fatigue
- Blurred vision
- Recurrent yeast/fungal infections
- Unexplained weight loss (late, when beta-cell failure is significant)
- Goldman-Cecil Medicine; Cleveland Clinic
5. Reproductive / Endocrine Features (especially in women)
Hyperinsulinemia stimulates ovarian androgen production, leading to:
- Polycystic ovary syndrome (PCOS): Chronic anovulation, oligomenorrhea or amenorrhea, infertility
- Hirsutism: Excess androgen-driven body/facial hair growth
- Elevated free testosterone / hyperandrogenism
- Enlarged, cystic ovaries on ultrasound
- Robbins & Kumar Basic Pathology; Harrison's 22E
6. Features of Obesity / Body Composition
- Central (visceral/abdominal) obesity - increased waist circumference is both a cause and a sign of insulin resistance
- Visceral fat sends FFAs directly to the liver via the portal circulation, worsening hepatic insulin resistance
- Fat accumulation in skeletal muscle and liver (non-alcoholic fatty liver disease / MASLD) is closely associated
- Robbins & Kumar Basic Pathology; Harrison's 22E, Chapter 420
7. Features of the Metabolic Syndrome (Cluster Presentation)
Insulin resistance is the unifying pathophysiologic thread of metabolic syndrome, diagnosed when 3 or more of the following are present:
| Criterion | Threshold (IDF/AHA-NHLBI) |
|---|---|
| Increased waist circumference | Population/ethnicity-specific cut-offs |
| Fasting triglycerides | ≥150 mg/dL (1.7 mmol/L) |
| Low HDL | <40 mg/dL (M) / <50 mg/dL (F) |
| Blood pressure | ≥130/85 mmHg |
| Fasting glucose | ≥100 mg/dL |
- Harrison's Principles of Internal Medicine 22E
Summary Table: Signs vs. Symptoms
| Category | Signs (Objective) | Symptoms (Subjective) |
|---|---|---|
| Skin | Acanthosis nigricans, skin tags | - |
| Metabolic labs | High insulin, high TG, low HDL, high glucose | - |
| Cardiovascular | Hypertension, endothelial dysfunction | - |
| Hyperglycemia | Elevated blood glucose | Thirst, polyuria, fatigue, blurred vision |
| Reproductive | Hirsutism, PCOS, elevated androgens | Irregular periods, infertility |
| Body composition | Abdominal obesity, fatty liver | Weight gain |
| Inflammation | Elevated CRP, IL-6, TNF-α | Fatigue |
Key clinical pearl: Insulin resistance is often clinically silent in early stages. Acanthosis nigricans and central obesity are the most recognizable bedside clues. Progression to overt symptoms (polyuria, polydipsia) signals that beta-cell compensation has begun to fail, heralding type 2 diabetes.
This is a shared conversation. Sign in to Orris to start your own chat.