Opoid poisoning
Reading File
Finding Sources
Searching PubMed
"opioid overdose"[MeSH Terms] AND "naloxone"[MeSH Terms]
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I have comprehensive information from multiple authoritative sources. Let me now compose a thorough clinical answer.
Opioid Poisoning (Overdose)
Pathophysiology
Opioids act primarily on μ (mu), κ (kappa), and δ (delta) receptors throughout the CNS and periphery. Overdose leads to respiratory depression as the dominant lethal mechanism — via μ-receptor activation in brainstem respiratory centres — combined with CNS depression and cardiovascular instability. Fentanyl is 50–100× more potent than morphine and 10× more potent than heroin, making it the leading driver of overdose deaths in recent years. — Goodman & Gilman's The Pharmacological Basis of Therapeutics
Clinical Features — The Classic Triad
| Feature | Detail |
|---|---|
| Miosis | Pin-point pupils (mydriasis only if severe anoxia supervenes) |
| CNS depression | Stupor → coma |
| Respiratory depression | Shallow, slow respirations; respiratory rate <12/min |
Additional signs: bradycardia, hypotension, hypothermia, cyanosis, cold/clammy skin, pulmonary oedema (especially with heroin).
Opioids generally do not cause seizures — exceptions are meperidine (normeperidine accumulation), high-dose tramadol, or neonatal opioid withdrawal. — Harrison's Principles of Internal Medicine, 22nd ed. (2025)
Diagnosis
- Clinical — recognition of the triad is the basis for immediate treatment; do not wait for labs.
- Toxicology screen (blood or urine) confirms the diagnosis but must not delay management.
- Consider co-ingestion: benzodiazepines are a frequent fatal combination (especially with buprenorphine).
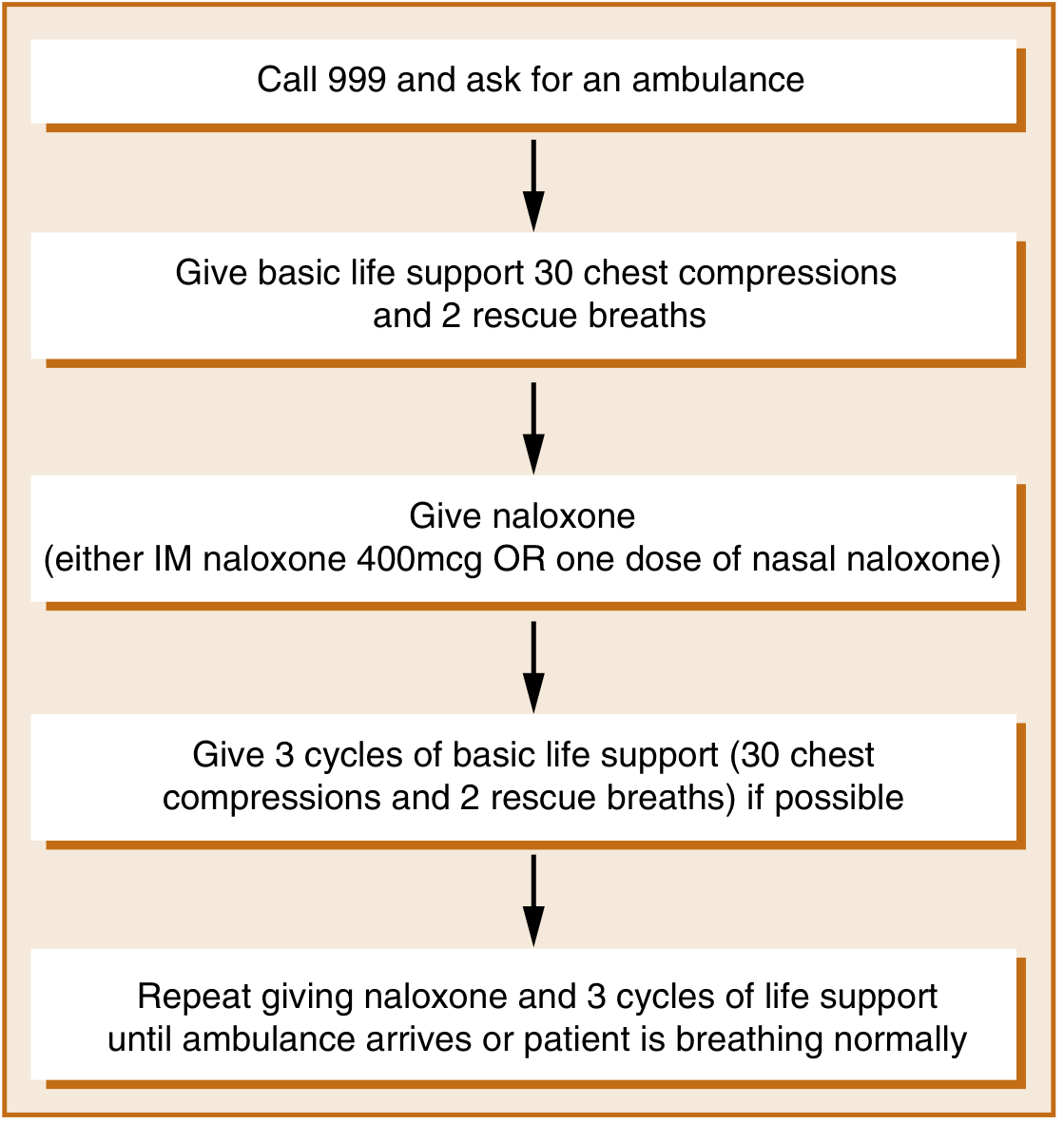
Emergency Management
Step 1 — Airway & Breathing
- Establish airway immediately; intubation and mechanical ventilation may be required.
- Supplemental oxygen; bag-mask ventilation if needed.
Step 2 — Naloxone (Opioid Antagonist)
Naloxone is the cornerstone of reversal — a highly specific opioid antagonist with rapid onset (~1–2 min IV).
| Route | Initial Dose |
|---|---|
| IV / IM / Endotracheal | 0.4–2.0 mg |
| Intranasal (concentrated) | 2 mg (equivalent to 400 mcg IM but longer-lasting peak) |
Repeat dosing / infusion:
- Repeat doses as needed to restore adequate respiration.
- Continuous IV infusion: give ½ to ⅔ of the initial reversal dose per hour; titrate to respiratory rate — not to consciousness (avoid precipitating withdrawal).
- Duration: naloxone infusion typically continued 24–72 hours depending on the opioid (morphine vs. long-acting methadone).
Special situations:
- Fentanyl / high-potency synthetic opioids: may require total doses ≥10 mg naloxone; rescue kits designed for fentanyl contain double the traditional dose.
- Buprenorphine overdose: primary buprenorphine overdose alone is nearly impossible due to its partial agonist ceiling effect; suspect co-ingestion (especially benzodiazepines).
- Nalmefene — higher potency, longer duration than naloxone; now available as an alternative reversal agent.
⚠️ Key principle: the goal is to reverse respiratory depression, not to fully awaken the patient. Over-reversal precipitates acute opioid withdrawal (agitation, vomiting, pulmonary oedema) and is dangerous.
Co-ingestion / Mixed Overdose
| Co-ingestant | Antidote / Action |
|---|---|
| Benzodiazepines | Flumazenil 0.2 mg/min IV (caution: may precipitate seizures; raises ICP) |
| Cocaine / stimulants | Supportive; benzodiazepines for agitation |
| Suspect polydrug if naloxone response is limited |
Summary Table: Management of Opioid Overdose
(Harrison's, Table 467-2)
- Establish airway; intubation + mechanical ventilation if necessary
- Naloxone 0.4–2.0 mg IV/IM/ET — onset ~1–2 min
- Repeat doses as needed, then continuous infusion (½–⅔ of reversal dose/hour)
- Continuous monitoring for 24–72 h; infusion not needed if patient is intubated
- Consider co-ingestants if response is partial
Post-Acute: Withdrawal & Longer-Term Treatment
Opioid Withdrawal Management
Taper using methadone (oral, 10 mg q2–4h PRN for objective signs, total ≤40 mg stabilisation dose on day 1; reduce by 5 mg/day) or buprenorphine (initiated once objective withdrawal signs present, guided by COWS score). — Goldman-Cecil Medicine
FDA-Approved Treatments for Opioid Use Disorder
| Drug | Mechanism | Notes |
|---|---|---|
| Methadone | Full μ-agonist | Long-acting; dispensed via licensed clinics only |
| Buprenorphine | Partial μ-agonist | Office-prescribable; ceiling effect limits overdose risk |
| Naltrexone | Pure antagonist | Requires full detoxification first; prevents relapse |
Methadone and buprenorphine maintenance are both associated with reduced overdose mortality and all-cause mortality. — Goldman-Cecil Medicine
Take-Home Naloxone (Prevention)
- Patients on >50 morphine milligram equivalents/day should receive a naloxone prescription at discharge.
- IM or intranasal naloxone kits are effective for lay first-responders.
- Patient and family training in take-home naloxone significantly reduces overdose deaths. — Washington Manual; Maudsley Guidelines
Sources: Harrison's Principles of Internal Medicine 22E (2025) · Goldman-Cecil Medicine · Goodman & Gilman's Pharmacological Basis of Therapeutics · The Maudsley Prescribing Guidelines in Psychiatry, 15th ed. · Washington Manual of Medical Therapeutics
Pontine hemorrhage vs opoid poisoning
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Now I have everything needed for a thorough, image-supported comparison.
Pontine Hemorrhage vs. Opioid Poisoning
Both conditions share pinpoint pupils + coma + respiratory depression — making this one of the most important and challenging differentials in emergency neurology. The key is that they overlap on one sign (miosis) but diverge on nearly everything else.
Why They Overlap
The pons contains both:
- Descending sympathetic pupillodilator fibres (sympathetic, from hypothalamus)
- Ascending pupillodilator pathways
A pontine lesion destroys both simultaneously → bilateral near-maximal pupillary constriction. Opioids produce the same pupillary finding via μ-receptor–mediated enhancement of Edinger-Westphal parasympathetic tone. Both give reactive, pinpoint pupils — under magnification, light response is preserved in both. — Plum and Posner's Diagnosis and Treatment of Stupor and Coma
Side-by-Side Comparison
| Feature | Pontine Hemorrhage | Opioid Poisoning |
|---|---|---|
| Pupils | Pinpoint, reactive (reactive to light on magnification) | Pinpoint, reactive |
| Onset | Sudden, hyperacute (seconds–minutes) | Gradual (minutes–hours) |
| Consciousness | Deep coma, often immediately | Drowsiness → stupor → coma; gradual |
| Respiratory pattern | Ataxic / periodic / apneustic breathing (pontine respiratory centre damage) | Slow, shallow, regular depression |
| Motor signs | Quadriplegia / flaccid paralysis; decerebrate posturing; bilateral extensor responses | No focal motor deficits; flaccid but symmetric and without focal signs |
| Oculomotor signs | Absent oculovestibular (caloric) responses; horizontal ophthalmoplegia; ocular bobbing; skewed deviation | Oculocephalic reflexes preserved; no gaze palsy; no ocular bobbing |
| Ciliospinal reflex | Absent | Preserved |
| Temperature | Hyperthermia (38.5–40°C) in nearly all within hours | Hypothermia (opioids cause heat loss) |
| Blood pressure | Usually hypertensive (history of poorly treated HTN) | Normal or hypotensive |
| Heart rate | Bradycardia common | Bradycardia can occur, less prominent |
| Response to naloxone | No response | Dramatic reversal of respiratory depression and miosis |
| CT head | Hyperintense (white) lesion in pons on non-contrast CT | Normal |
| Cause | Hypertensive bleed, AVM rupture | Drug ingestion (history, toxicology screen) |
The Decisive Distinguishing Features
1. Ocular Bobbing
Present in pontine hemorrhage; absent in opioid poisoning. Ocular bobbing (rapid downward conjugate eye movement with slow return) is pathognomonic of pontine or lower brainstem structural damage.
2. Absent Oculovestibular Responses
Caloric testing is intact in opioid overdose. In pontine hemorrhage, the horizontal gaze centres are destroyed → absent vestibulo-ocular reflex (doll's eye manoeuvre and cold caloric both fail).
3. Quadriplegia / Decerebrate Posturing
Opioids cause symmetric flaccidity but no focal motor signs and no corticospinal tract signs. Pontine hemorrhage produces bilateral corticospinal tract damage → quadriplegia, extensor posturing, absent/abnormal tendon reflexes.
4. Hyperthermia vs. Hypothermia
Pontine hemorrhage → hyperthermia (near-universal within hours).
Opioid poisoning → hypothermia.
5. Naloxone Test
"The pinpoint pupils may suggest an opiate overdose, but the other eye signs and flaccid quadriplegia are not seen in that condition. If there is any question in an ambiguous case, naloxone can be administered to reverse any opiate intoxication." — Plum and Posner's Diagnosis and Treatment of Stupor and Coma
Naloxone 0.4–2 mg IV should be given to any comatose patient with pinpoint pupils when the diagnosis is uncertain. No response = structural cause. Rapid reversal = opioid toxicity.
CT Scan
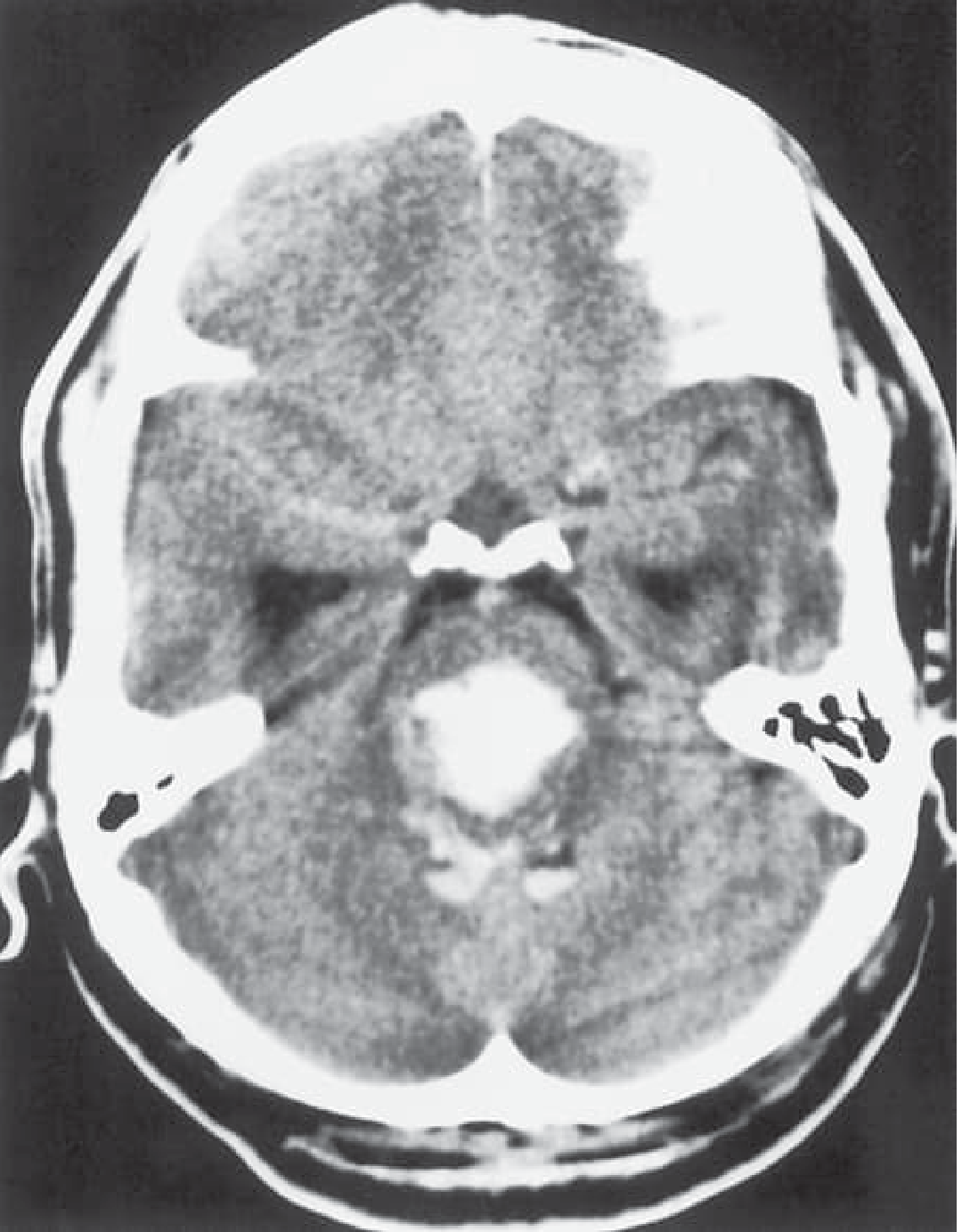
The dense hyperdense (bright white) lesion in the brainstem on non-contrast CT is diagnostic of hemorrhage and is absent in opioid poisoning.
Clinical Findings in Pontine Hemorrhage (n=80)
(Plum and Posner's, from Murata et al.)
| Finding | % of Cases |
|---|---|
| Coma at presentation | 50% |
| Respiratory disturbance | 46% |
| Bradycardia | 43% |
| Hyperthermia | 40% |
| Pinpoint pupils | 29% |
| Hemiplegia | 43% |
| Tetraplegia | 28% |
| Decerebrate posturing | 20% |
Note: pinpoint pupils occur in only ~29% of all pontine hemorrhages — many present with anisocoria or normal pupils — emphasising that miosis alone is not sufficient for either diagnosis.
Quick Decision Algorithm
Coma + Pinpoint Pupils
│
├── Give IV Naloxone 0.4–2 mg
│ │
│ Reversal → Opioid Poisoning ✓
│ No reversal ↓
│
├── CT Head (stat, non-contrast)
│ │
│ Hyperdense pontine lesion → Pontine Hemorrhage ✓
│ Normal CT ↓
│
└── Metabolic / toxic workup (BMP, LFTs, toxicology, EEG)
Sources: Plum and Posner's Diagnosis and Treatment of Stupor and Coma · Bradley and Daroff's Neurology in Clinical Practice · Harrison's Principles of Internal Medicine 22E (2025) · Localization in Clinical Neurology, 8th ed.
This is a shared conversation. Sign in to Orris to start your own chat.