Hypertensive disorders in pregnancy
Reading File
Finding Sources
Searching PubMed
"hypertensive disorders" AND "pregnancy"
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Searching Images
preeclampsia pathophysiology spiral artery remodeling trophoblast
Reading File
Finding Sources
I now have comprehensive data from multiple authoritative textbooks. Let me compose a thorough, well-structured response.
Hypertensive Disorders of Pregnancy (HDP)
Classification (ACOG)
HDP encompasses four distinct entities:
| Category | Definition |
|---|---|
| Gestational hypertension | New-onset BP ≥140/90 mmHg after 20 weeks' gestation, without proteinuria or end-organ damage |
| Preeclampsia | Gestational hypertension plus proteinuria (≥300 mg/24 h, protein:creatinine ≥0.3, or dipstick 2+) or new end-organ damage |
| Eclampsia | Preeclampsia + new-onset tonic-clonic/focal seizures not explained by other causes |
| Chronic hypertension | BP ≥140/90 diagnosed before pregnancy or before 20 weeks, or persisting >12 weeks postpartum |
| Superimposed preeclampsia | New proteinuria or end-organ damage in a woman with pre-existing chronic hypertension |
| White coat hypertension | Elevated office BP, usually before 20 weeks; may progress; ambulatory monitoring may be needed |
(Braunwald's Heart Disease, Table 92.1; ACOG Practice Bulletin 222)
Epidemiology
- HDP affects ~8.5% of deliveries in the United States; globally responsible for significant maternal mortality
- Gestational hypertension: 6–17% of nulliparous patients; 2–4% of parous patients
- Preeclampsia: 5–8% of all pregnancies; up to 15% with long-term implications
- Eclampsia: 1 in 2,000–3,000 deliveries in high-resource settings
- Nulliparity accounts for the greatest population-attributable fraction for preeclampsia (~32%)
Key risk factors:
- Prior preeclampsia (8-fold increased risk)
- Chronic hypertension (25% develop superimposed preeclampsia)
- Pregestational diabetes (up to 70% risk in class F/R)
- Antiphospholipid syndrome, SLE
- Obesity, multifetal gestation, IVF
- Non-Hispanic Black race (related more to severity than incidence)
- Age extremes; family history
(Creasy & Resnik's MFM, Ch. 45; Goldman-Cecil Medicine, Ch. 221)
Pathophysiology
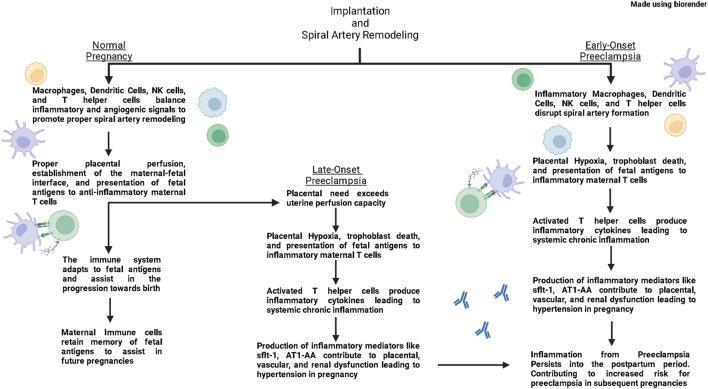
HDP — particularly preeclampsia — involves a two-stage process:
Stage 1 — Impaired spiral artery remodeling
In a normal pregnancy, extravillous trophoblasts invade the spiral arteries, replacing the musculoelastic wall with wide vascular sinusoids, lowering resistance and increasing uteroplacental blood flow. In preeclampsia, this remodeling is deficient: channels remain narrow, producing placental hypoxia and ischemia.
Stage 2 — Systemic maternal endothelial dysfunction
Placental hypoxia triggers release of anti-angiogenic factors into the maternal circulation:
- sFlt-1 (soluble fms-like tyrosine kinase-1) — antagonizes VEGF and PlGF
- Soluble endoglin (sEng) — antagonizes TGF-β
These factors cause widespread endothelial dysfunction, leading to:
- Hypertension: reduced prostacyclin (PGI₂) and PGE₂ (vasodilators) + increased thromboxane A₂ (vasoconstrictor)
- Proteinuria: glomerular endotheliosis — the renal lesion of preeclampsia
- Hypercoagulability: decreased antithrombotic factors; platelet consumption
- Hepatic dysfunction / HELLP syndrome
- Pulmonary edema: increased afterload + capillary leak; aggressive fluid administration worsens it
- Neurological effects: cerebral vasospasm, PRES (reversible posterior encephalopathy syndrome)
Hemoconcentration is a hallmark. Cardiac output is compromised by increased afterload.
(Robbins & Kumar Basic Pathology, Ch. 22; Goldman-Cecil Medicine, Ch. 221)
Clinical Features and Diagnosis
Preeclampsia without severe features
- BP ≥140/90 mmHg on two occasions ≥4 hours apart after 20 weeks
- Plus proteinuria or any end-organ finding below
Preeclampsia with severe features (any one of):
| Feature | Threshold |
|---|---|
| Severe hypertension | SBP ≥160 or DBP ≥110 mmHg × 2, ≥4 h apart |
| Thrombocytopenia | Platelets <100,000/μL |
| Hepatic dysfunction | LFTs >2× upper limit of normal |
| RUQ/epigastric pain | Severe, unresponsive to medication |
| Renal insufficiency | Creatinine >1.1 mg/dL or doubling of baseline |
| Pulmonary edema | — |
| Neurological symptoms | New-onset headache unresponsive to analgesics, visual disturbances |
HELLP syndrome — ~10% of severe preeclampsia:
- Hemolysis (microangiopathic)
- ELevated liver enzymes
- LP Low platelets
Eclampsia: Tonic-clonic seizures, often preceded by headache or visual disturbances. Post-ictal state with hypercarbia, transient hypoxia, lactic acidemia. MRI may show PRES (occipital/parietal cortical changes). CT head if intracranial hemorrhage is suspected.
Postpartum presentation: Preeclampsia/eclampsia can present up to 6 weeks postpartum — early recognition is critical.
(Goldman-Cecil Medicine, Ch. 221; Braunwald's Heart Disease, Ch. 92)
Management
1. Antihypertensive Therapy
Non-severe hypertension (140–159/90–109 mmHg):
- Oral agents: labetalol, nifedipine, methyldopa
- Goal: avoid sustained severe-range BP while not over-treating (fetal perfusion depends on adequate MAP)
Severe-range hypertension (≥160/110 mmHg) — treat urgently:
| Drug | Regimen |
|---|---|
| Nifedipine IR (oral) | 10–20 mg; repeat in 20 min; then 10–20 mg q2–6h; max 180 mg/day |
| Labetalol (IV, preferred) | 10–20 mg initial; then 1–2 mg/min infusion (or 20–80 mg q10–30 min); max 300 mg |
| Hydralazine (IV) | 5 mg initial; then 0.5–10 mg/hr (or 5–10 mg q20–40 min); max 20 mg |
(Goldman-Cecil Medicine, Table 221-6)
Recent 2025 network meta-analysis (PMID 40216176) assessed oral antihypertensive options in pregnancy — should be consulted for updated comparative effectiveness data.
2. Seizure Prophylaxis (Magnesium Sulfate)
- Loading dose: 4–6 g IV over 15–20 minutes
- Maintenance: 2 g/hour IV infusion
- Continue for 24–48 hours postpartum
- Toxicity: diminished DTRs → respiratory depression → cardiac arrest
- Monitor: urine output, reflexes, respiratory rate
- Antidote: calcium gluconate 1 g IV over 2–5 minutes
- Cleared renally — reduce/monitor closely with renal impairment
- For recurrent seizures despite MgSO₄: give additional 2 g bolus; avoid respiratory depressants
3. Delivery — The Only Cure
- Definitive management: delivery of fetus and placenta
- Timing balances gestational age vs. severity
- Preeclampsia with severe features at ≥34 weeks → deliver
- <34 weeks: individualized; corticosteroids for fetal lung maturity if expectant management
- Emergent cesarean is not required for an eclamptic seizure alone (absent placental abruption); fetal compromise often resolves with maternal stabilization within minutes
4. Fluid Management
- Most women develop pulmonary edema after delivery
- Restrict IV fluids; avoid volume expansion (albumin not routinely recommended)
- Treat pulmonary edema with furosemide 20 mg IV + afterload reduction
Prevention
Low-dose aspirin (81–162 mg/day, started at 12–16 weeks' gestation):
- Recommended for high-risk women (prior preeclampsia, multifetal gestation, chronic hypertension, diabetes, renal disease, autoimmune conditions)
- Multiple meta-analyses confirm benefit in reducing preeclampsia incidence and preterm birth
- A Cochrane review supports its use; the ASPRE trial showed greatest benefit when initiated early (<16 weeks) in screen-positive women
Calcium supplementation: reduces risk in populations with low dietary calcium intake.
(Creasy & Resnik's MFM; National Kidney Foundation Primer, 8e; Brenner & Rector's The Kidney)
Long-Term Cardiovascular Implications
Preeclampsia is not merely an obstetric complication — it is a window into future cardiovascular health:
- Chronic hypertension 2–7 years postpartum: 36.5% of affected women (vs. 17% controls)
- After early-onset preeclampsia: up to 50%
- After gestational hypertension: 39%
- 2-fold increased risk for CVD overall; up to 8-fold for early-onset (<34 weeks) preeclampsia
- Increased risk for coronary artery disease, cerebrovascular disease, heart failure, and peripheral vascular disease within 5 years of delivery
- Left ventricular diastolic dysfunction detectable up to a decade postpartum
- The AHA recognizes a history of HDP as an established cardiovascular risk factor
Pregnancy functions as a "stress test" — women who develop HDP have subclinical vascular risk made clinically manifest. This creates an opportunity for targeted post-pregnancy cardiovascular risk reduction.
(Creasy & Resnik's MFM, Ch. 72)
Summary Table
| Feature | Gestational HTN | Preeclampsia | Eclampsia | HELLP |
|---|---|---|---|---|
| BP ≥140/90 | ✓ | ✓ | ✓ | ✓ |
| Proteinuria | ✗ | ✓ (or end-organ) | ✓ | Variable |
| Seizures | ✗ | ✗ | ✓ | ✗ |
| Hemolysis/↑LFTs/↓Plt | ✗ | ✗ | ✗ | ✓ |
| Onset | >20 wks | >20 wks | >20 wks/postpartum | 3rd trimester |
| MgSO₄ | Only if severe | Yes (severe features) | Yes | Yes |
| Delivery | At term | By 37 wks (mild); earlier if severe | Urgent | Urgent |
Key references:
- Creasy & Resnik's Maternal-Fetal Medicine, 8e — Chs. 45, 72
- Goldman-Cecil Medicine — Ch. 221
- Braunwald's Heart Disease, 12e — Ch. 92 (ACOG Classification Table)
- Robbins & Kumar Basic Pathology — Ch. 22
- ACOG Practice Bulletin No. 222 (2020)
- Hup et al. (2025) — Oral antihypertensives in pregnancy: network meta-analysis [PMID 40216176]
This is a shared conversation. Sign in to Orris to start your own chat.