GI SYSTEM ANATOMY AND PHYSIOLOGY FROM BD CHAURASIA AND GUYTON AND GANONG
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
I now have extensive content from both Guyton and Ganong with key diagrams. Let me compile the comprehensive response.
GI System - Anatomy and Physiology
Sources: Guyton & Hall Textbook of Medical Physiology (14e) | Ganong's Review of Medical Physiology (26e)
Note: BD Chaurasia's Human Anatomy is not in the library database. The anatomy content below is drawn from Guyton & Hall (which includes GI anatomy detail) and supplemented with Ganong's structural coverage. The physiology sections are extensively covered from both Guyton and Ganong.
OVERVIEW OF THE GI SYSTEM
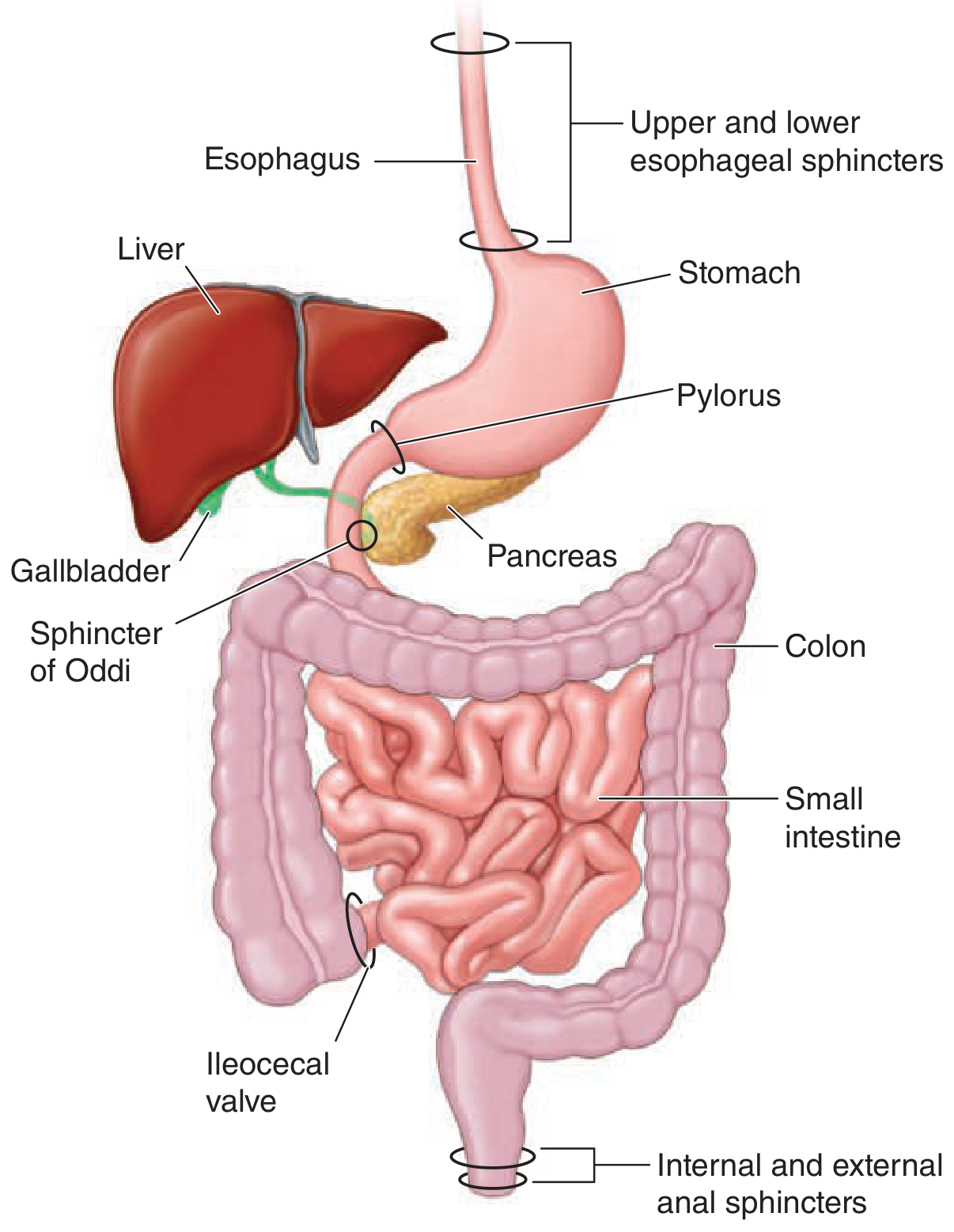
The gastrointestinal system serves as the portal through which nutrients and water are absorbed into the body. The intestine is a continuous tube from mouth to anus, formally contiguous with the external environment. Food encounters:
- Mouth → Esophagus → Stomach → Duodenum → Jejunum → Ileum → Cecum → Colon → Rectum → Anus
The GI tract divides into functional segments separated by sphincters: upper and lower esophageal sphincters, pylorus, ileocecal valve, and inner/outer anal sphincters.
- Ganong's Review of Medical Physiology, 26e, p. 457
PART I: ANATOMY
1. Layers of the GI Wall (Physiologic Anatomy)
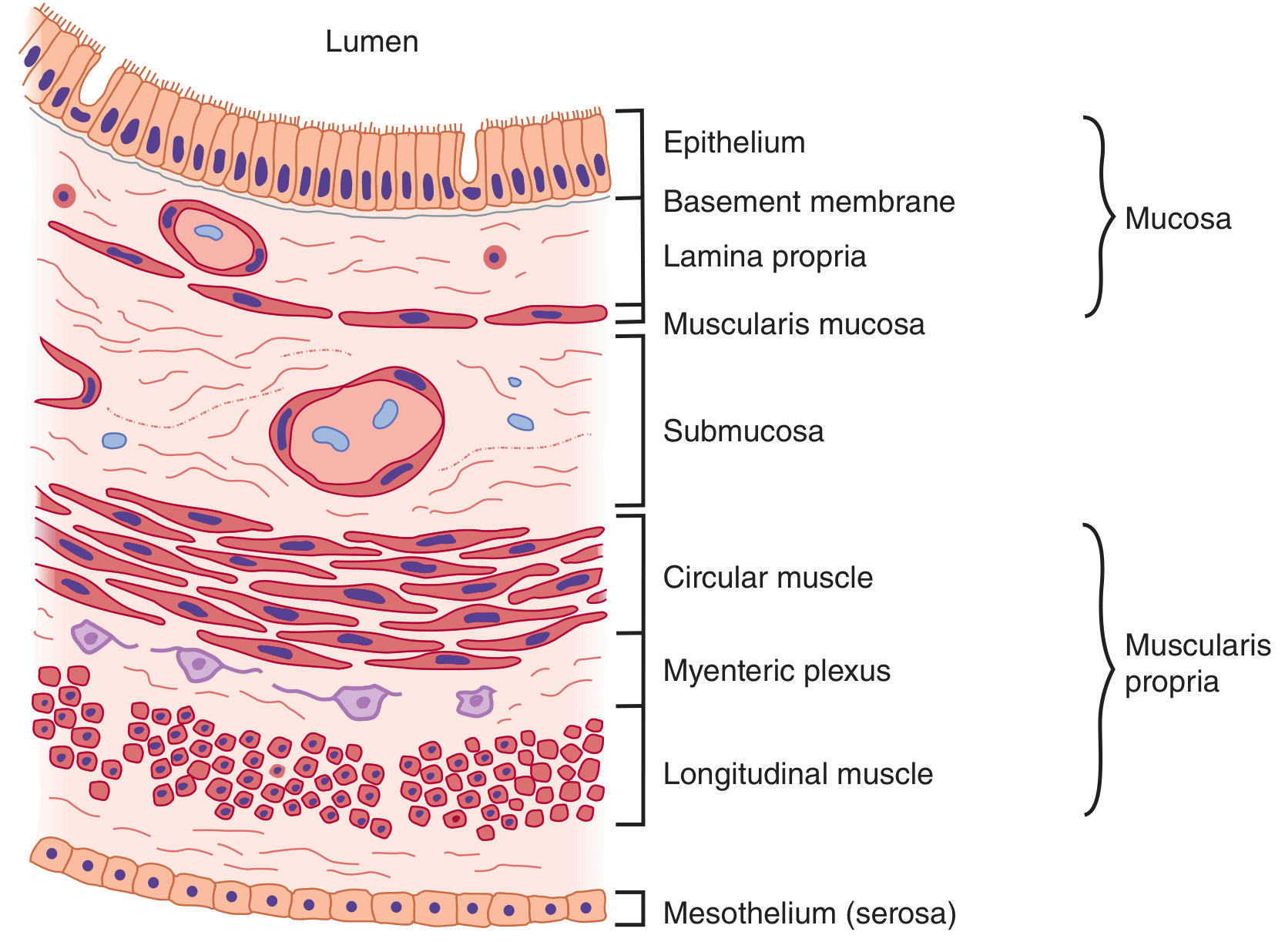
From outer to inner, the gut wall has 5 layers:
| Layer | Details |
|---|---|
| Serosa | Outermost; peritoneal covering |
| Longitudinal smooth muscle | Outer muscle layer; bundles run along length of gut |
| Circular smooth muscle | Inner muscle layer; bundles encircle the gut |
| Submucosa | Loose connective tissue; contains Meissner's (submucosal) plexus, blood vessels, lymphatics |
| Mucosa | Innermost; contains epithelium, lamina propria, muscularis mucosae |
Between the circular and longitudinal muscle layers lies the myenteric (Auerbach's) plexus, the major neural network controlling gut motility.
- Guyton & Hall, p. 776
2. GI Smooth Muscle - Syncytial Organisation
- Individual smooth muscle fibers: 200-500 µm long, 2-10 µm diameter
- Arranged in bundles of up to 1000 parallel fibers
- Longitudinal layer: bundles run lengthwise; circular layer: bundles encircle the gut
- Fibers connected by gap junctions - low-resistance pathways for ionic current spread
- Each muscle layer acts as a functional syncytium: an action potential spreads throughout the mass
- Guyton & Hall, p. 776
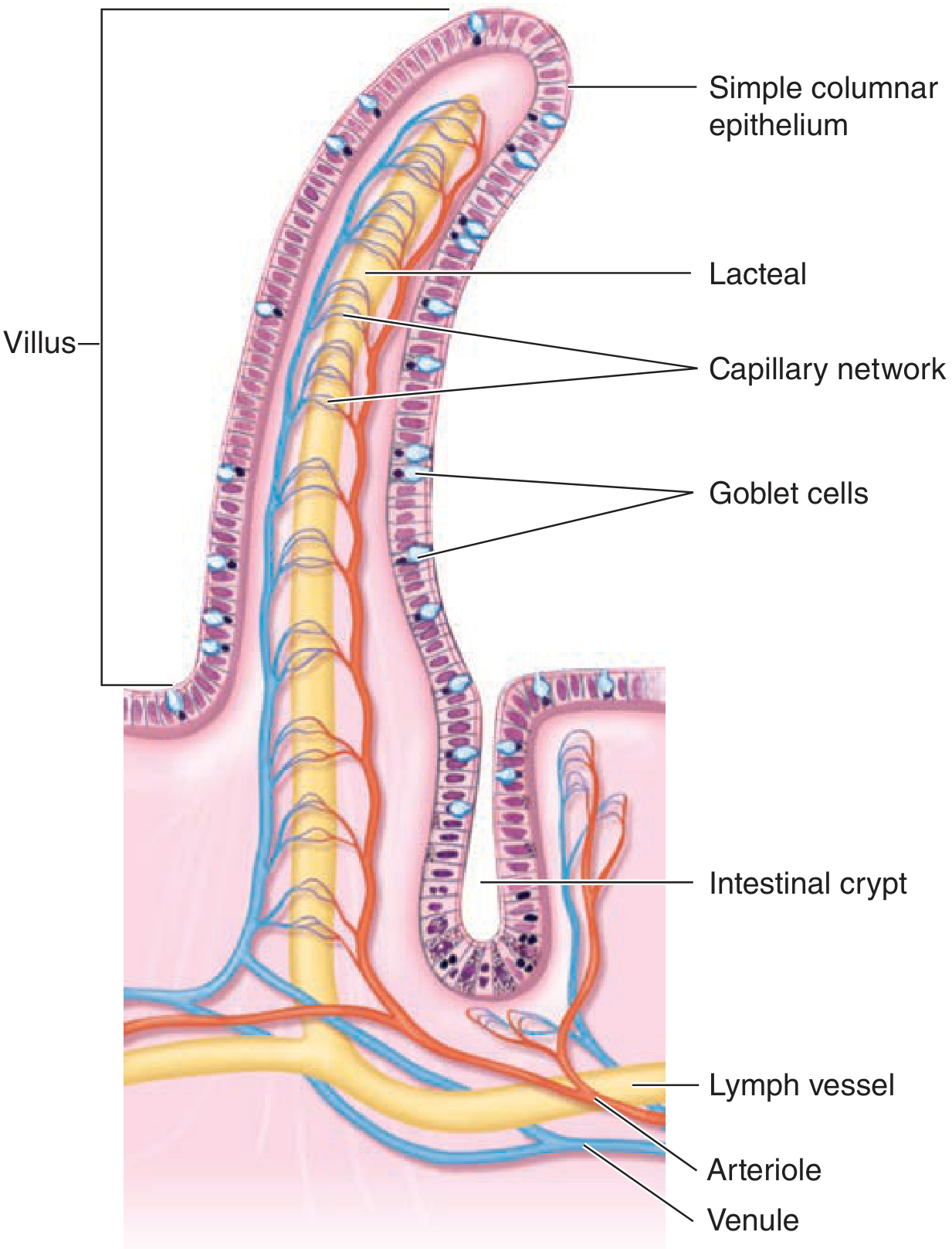
3. Villi and Crypts (Small Intestine)
The small intestinal mucosa is folded into finger-like villi to maximize absorptive surface area. Between villi are crypts of Lieberkühn.
-
Stem cells at the crypt base give rise to all epithelial cells
-
Epithelium turns over every 3-5 days
-
Villus cells have extensive microvilli (brush border) with a glycocalyx
-
Brush border hydrolases perform final digestion
-
Crypt base contains Paneth cells (antimicrobial peptides) and stem cells
-
Epithelial layer contains scattered endocrine cells and intraepithelial lymphocytes
-
Ganong's Review, p. 458
4. Blood Supply (Splanchnic Circulation)
- Celiac artery - stomach
- Superior mesenteric artery (SMA) - small intestine + proximal large intestine
- Inferior mesenteric artery (IMA) - distal colon and rectum
The arteries enter the gut wall and branch, sending smaller arteries in both directions around the gut, meeting on the anti-mesenteric border. From these, small arteries penetrate into:
- Muscle bundles
- Intestinal villi
- Submucosal vessels (for secretion and absorption)
Portal circulation: Water-soluble nutrients (carbohydrates, proteins) → portal vein → liver sinusoids. The liver temporarily stores 50-75% of absorbed nutrients.
Lymphatic drainage: Fats are absorbed into intestinal lacteals → intestinal lymphatics → thoracic duct → systemic circulation, bypassing the liver.
- Guyton & Hall, p. 783
PART II: PHYSIOLOGY
1. Electrical Activity of GI Smooth Muscle
Two types of electrical waves are seen in GI smooth muscle:
a) Slow Waves (Basic Electrical Rhythm)
- Not action potentials; undulating changes in resting membrane potential
- Amplitude: 5-15 mV
- Frequency varies by region:
- Stomach body: ~3/min
- Duodenum: ~13/min
- Terminal ileum: ~8-9/min
- Generated by Interstitial Cells of Cajal (ICC) - the pacemakers of the gut
- ICCs form a network interposed between muscle layers with synaptic-like contacts to smooth muscle
- Slow waves alone do not cause contraction (except in the stomach)
b) Spike Potentials (True Action Potentials)
-
Occur when resting membrane potential rises above -40 mV
-
Normal resting membrane potential: -50 to -60 mV
-
Frequency: 1-10 spikes/sec
-
Duration: 10-20 milliseconds (much longer than nerve action potentials)
-
Carried mainly by calcium-sodium channels (slow channels) - NOT fast sodium channels
-
Calcium entry during action potential triggers muscle contraction
-
Guyton & Hall, p. 776-777
2. Neural Control - Enteric Nervous System (ENS)
The ENS ("second brain") consists of two plexuses:
| Plexus | Location | Function |
|---|---|---|
| Myenteric (Auerbach's) | Between circular and longitudinal muscle | Controls motility - peristalsis and mixing |
| Submucosal (Meissner's) | In submucosa | Controls secretion and blood flow |
The ENS can function independently of the CNS, making the gut capable of local reflex control. It contains roughly 100 million neurons - as many as the spinal cord.
3. Motility
Mastication (Chewing)
- Anterior teeth (incisors): cutting; posterior teeth (molars): grinding
- Force: 55 lbs on incisors, 200 lbs on molars
- Controlled by nuclei in the brain stem (motor branch of CN V - trigeminal)
- Chewing reflex: food in mouth → inhibition of jaw muscles → jaw drops → stretch reflex → jaw closure
Swallowing (Deglutition)
Three stages:
Voluntary (oral) stage: Tongue pushes bolus toward pharynx.
Pharyngeal stage (reflex):
- Soft palate rises → closes posterior nares
- Palatopharyngeal folds pull medially → passage only for small food
- Vocal cords appose; larynx rises, epiglottis covers opening
- Upper esophageal sphincter (UES/pharyngoesophageal sphincter) relaxes
- Pharyngeal peristalsis propels bolus into esophagus
- Entire stage: <2 seconds
- Swallowing center: medulla and lower pons
- Afferent: CN V, IX; Efferent: CN V, IX, X, XII
Esophageal stage:
-
Primary peristalsis: continuation of pharyngeal peristaltic wave; moves bolus in ~8-10 seconds
-
Secondary peristalsis: initiated by distension of esophagus if primary fails to clear bolus
-
Lower esophageal sphincter (LES) relaxes as the peristaltic wave approaches
-
Guyton & Hall, p. 789-791
Gastric Motility
- Receptive relaxation: fundus relaxes as food enters (mediated by vagus - VIP/NO)
- Mixing movements: antral contractions mix food with gastric juice → chyme
- Gastric emptying: regulated by duodenal receptors; fats and acid slow emptying via enterogastric reflex and hormones (secretin, CCK, GIP)
Small Intestine Motility
- Segmentation contractions: primary mixing movement; divide and re-divide the chyme
- Peristalsis: propulsive; moves chyme aborally at 0.5-2 cm/sec
- Migrating Motor Complex (MMC): housekeeping wave during fasting, every ~90 min; sweeps residue distally (controlled by motilin)
Large Intestine Motility
- Haustral contractions: mixing, slow movement
- Mass movements (mass peristalsis): 1-3 times/day, propel contents rapidly; triggered by gastrocolic reflex
- Defecation reflex: distension of rectum → internal anal sphincter relaxes; external sphincter under voluntary control
4. Secretion
Salivary Secretion
- Produced by parotid, submandibular, and sublingual glands
- Contains: salivary α-amylase (begins starch digestion), mucins (lubrication), IgA, lysozyme
- Saliva is hypotonic
- ~1-1.5 L/day
Gastric Secretion
- Parietal cells: secrete HCl (H⁺/K⁺-ATPase proton pump) and intrinsic factor
- Stimulated by: acetylcholine (via M3), histamine (via H2, cAMP), gastrin (via CCK-B receptor, Ca²⁺)
- Inhibited by: somatostatin, prostaglandins, GIP
- Chief cells: secrete pepsinogen (activated to pepsin by HCl)
- G cells (antrum): secrete gastrin
- Mucous cells: secrete mucus + HCO₃⁻ (protect mucosa)
- Output: ~2.5 L/day
Three phases of gastric secretion:
- Cephalic phase (~30%): sight/smell/taste/thought of food → vagus → HCl + pepsin
- Gastric phase (~60%): food in stomach → distension + amino acids → gastrin → HCl
- Intestinal phase (~10%): chyme in duodenum; initially stimulatory, then inhibitory
Pancreatic Secretion
- Exocrine pancreas: compound alveolar gland
- Secretin (from S cells, triggered by acid in duodenum): acts on duct cells → large volume, high HCO₃⁻, low enzyme juice (via cAMP)
- CCK (from I cells, triggered by fats and proteins): acts on acinar cells → enzyme-rich juice (via phospholipase C/Ca²⁺)
- Acetylcholine (vagus): also stimulates acinar cells → enzyme release
Principal digestive enzymes from Ganong's Table 25-2:
| Source | Enzyme | Substrate | Function |
|---|---|---|---|
| Salivary glands | Salivary α-amylase | Starch | Hydrolyzes 1:4 linkages → maltose, maltotriose |
| Stomach | Pepsins (from pepsinogen) | Proteins | Cleave bonds adjacent to aromatic AAs |
| Pancreas | Trypsin | Proteins | Cleaves bonds at basic AAs (Arg, Lys) |
| Pancreas | Chymotrypsin | Proteins | Cleaves bonds at aromatic AAs |
| Pancreas | Elastase | Elastin, proteins | Cleaves bonds at aliphatic AAs |
| Pancreas | Lipase | Triglycerides | Fatty acids + monoglycerides |
| Pancreas | Pancreatic amylase | Starch | α-limit dextrins + maltose |
| Intestinal mucosa | Enteropeptidase | Trypsinogen | Activates trypsin |
| Intestinal mucosa | Lactase, sucrase | Disaccharides | Monosaccharides |
- Ganong's Review, p. 462-464
Bile
- Secreted by hepatocytes, stored in gallbladder
- CCK causes gallbladder contraction + sphincter of Oddi relaxation
- Bile salts emulsify fats, forming micelles for lipase access
- Bile salts are reabsorbed in terminal ileum (enterohepatic circulation)
5. Absorption
Carbohydrates
- Digested to monosaccharides (glucose, galactose, fructose)
- Glucose and galactose: absorbed via SGLT1 (Na⁺-coupled, active) on apical membrane → GLUT2 on basolateral
- Fructose: absorbed via GLUT5 (facilitated) on apical membrane
Proteins
- Digested to amino acids and di/tripeptides
- Amino acids: Na⁺-coupled transporters (apical)
- Di/tripeptides: PepT1 (H⁺-coupled)
Fats
- Triglycerides → fatty acids + monoglycerides (pancreatic lipase)
- Packaged into micelles with bile salts
- Fatty acids enter enterocytes → reassembled into triglycerides → packaged into chylomicrons
- Chylomicrons exit via lacteals into lymphatics → thoracic duct
Vitamins and Minerals
- Vitamin B12 (cobalamin): requires intrinsic factor; absorbed in terminal ileum
- Iron: absorbed in duodenum as Fe²⁺ via DMT1
- Calcium: absorbed in duodenum, stimulated by 1,25-(OH)₂-vitamin D
- Fat-soluble vitamins (A, D, E, K): absorbed with fat in micelles
Water and Electrolytes
- GI tract handles ~9 liters/day of fluid (2L intake + 7L secretions)
- ~8.9 L is absorbed (small intestine: ~7-8L, colon: ~1.3-1.9L)
- Only ~100-200 mL excreted in feces
6. GI Hormones
| Hormone | Source | Stimulus | Actions |
|---|---|---|---|
| Gastrin | G cells (antrum) | Protein/AA, vagal stimulation, distension | ↑ HCl, pepsin; ↑ growth of gastric mucosa |
| Secretin | S cells (duodenum) | Acid (pH <4.5) in duodenum | ↑ HCO₃⁻ from pancreas and bile; ↓ gastric motility |
| CCK | I cells (duodenum/jejunum) | Fats and proteins in duodenum | ↑ pancreatic enzymes; gallbladder contraction; ↓ gastric emptying |
| GIP (glucose-dependent insulinotropic peptide) | K cells (duodenum/jejunum) | Glucose, fat | ↑ insulin release; ↓ gastric acid |
| Motilin | Mo cells (duodenum) | Fasting, fat | Initiates MMC during fasting |
| Somatostatin | D cells (throughout) | Acid, fat, protein | Inhibits all GI secretions and motility |
| VIP | ENS neurons | Nerve stimulation | Vasodilation; ↑ intestinal secretion; ↓ motility |
7. Blood Flow Regulation in the GI Tract
-
Blood flow in each GI region is directly proportional to local metabolic activity
-
During active absorption: blood flow in villi can increase up to 8-fold
-
Vasodilatory mechanisms: release of cholecystokinin, secretin, GIP, VIP from mucosa; liberation of kinins (kallikrein-kinin system); reduced O₂ tension (reactive hyperemia)
-
Portal hypertension: obstruction of portal venous flow → collaterals (esophageal varices, caput medusae, hemorrhoids)
-
Guyton & Hall, p. 783-785
8. Defecation
- Mass movements drive feces into rectum
- Rectal distension → intrinsic defecation reflex (via ENS) → internal anal sphincter relaxation (smooth muscle)
- Voluntary contraction of external anal sphincter (skeletal muscle, pudendal nerve) can delay defecation
- Valsalva maneuver, squatting position facilitate defecation
Summary: Key Numbers to Remember
| Parameter | Value |
|---|---|
| GI smooth muscle fiber length | 200-500 µm |
| Slow wave frequency - stomach | ~3/min |
| Slow wave frequency - duodenum | ~13/min |
| Slow wave frequency - terminal ileum | ~8-9/min |
| Resting membrane potential (GI SM) | -50 to -60 mV |
| Threshold for spike potential | -40 mV |
| Saliva production | ~1-1.5 L/day |
| Gastric secretion | ~2.5 L/day |
| Total fluid entering small intestine | ~9 L/day |
| Fecal water loss | ~100-200 mL/day |
| Epithelial turnover rate | 3-5 days |
Sources: Guyton and Hall Textbook of Medical Physiology (14e) | Ganong's Review of Medical Physiology (26e)
Note on BD Chaurasia: BD Chaurasia's Human Anatomy is not available in the textbook library. For GI anatomy as per BD Chaurasia, the key topics to study are: peritoneum and its reflections, blood supply (celiac trunk, SMA, IMA), portal circulation, lymphatic drainage of each segment, nerve supply (vagus, sympathetic splanchnic nerves, pudendal nerve), relations of each organ (stomach, duodenum, jejunum, ileum, large intestine), and surgical anatomy of the anal canal. The structural anatomy covered above (layers of the wall, villi, splanchnic circulation) is consistent across standard anatomy and physiology textbooks.
This is a shared conversation. Sign in to Orris to start your own chat.