Anatomy of knee along with the ligaments with meniscus and the retinaculum
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive information from Gray's Anatomy for Students and the THIEME Atlas of Anatomy. Let me compile the full, detailed answer.
Anatomy of the Knee Joint
The knee is one of the most complex synovial joints in the human body. It is classified as a modified hinge (ginglymus) joint that allows predominantly sagittal plane motion (flexion-extension 5° hyperextension to 135° flexion) with a limited degree of rotation that increases with flexion.
Articulating Bones
The knee consists of three articulations within a single joint capsule:
- Medial tibiofemoral joint - between the medial femoral condyle and medial tibial plateau
- Lateral tibiofemoral joint - between the lateral femoral condyle and lateral tibial plateau
- Patellofemoral joint - between the posterior patellar surface and the patellar (trochlear) surface of the femur
The shape of the femoral condyles is curved and rounded posteriorly (in flexion) and broad and flat inferiorly (in extension), making the joint inherently unstable - hence the reliance on ligaments, menisci, and muscles for stability.
Joint Capsule
The fibrous capsule of the knee envelops all three articulations. Key features:
- Anteriorly reinforced by the quadriceps tendon, patella, patellar ligament, and retinacula
- Posteriorly reinforced by the oblique and arcuate popliteal ligaments and muscle tendons
- The synovial membrane lines the inner surface of the capsule and projects into the joint as alar folds flanking the infrapatellar fat pad
- The suprapatellar bursa communicates superiorly with the joint cavity
The static stabilizers are the capsule, menisci, cruciate and collateral ligaments. The dynamic stabilizers are the quadriceps and hamstrings.
Overview of Ligaments
Knee ligaments are divided into extrinsic (outside the synovial cavity) and intrinsic (inside the joint, intracapsular but extrasynovial):
Extrinsic Ligaments
Anterior:
- Patellar ligament
- Medial and lateral longitudinal patellar retinacula
- Medial and lateral transverse patellar retinacula
Medial and lateral sides:
- Medial collateral ligament (tibial collateral ligament)
- Lateral collateral ligament (fibular collateral ligament)
Posterior:
- Oblique popliteal ligament
- Arcuate popliteal ligament
Intrinsic Ligaments
- Anterior cruciate ligament (ACL)
- Posterior cruciate ligament (PCL)
- Transverse ligament of the knee
- Posterior meniscofemoral ligament (ligament of Wrisberg)
Ligaments in Detail
1. Patellar Ligament
The patellar ligament is the direct continuation of the quadriceps femoris tendon inferior to the patella. It attaches above to the margins and apex of the patella, and below to the tibial tuberosity. It forms the central, strongest component of the anterior knee structure.
2. Collateral Ligaments
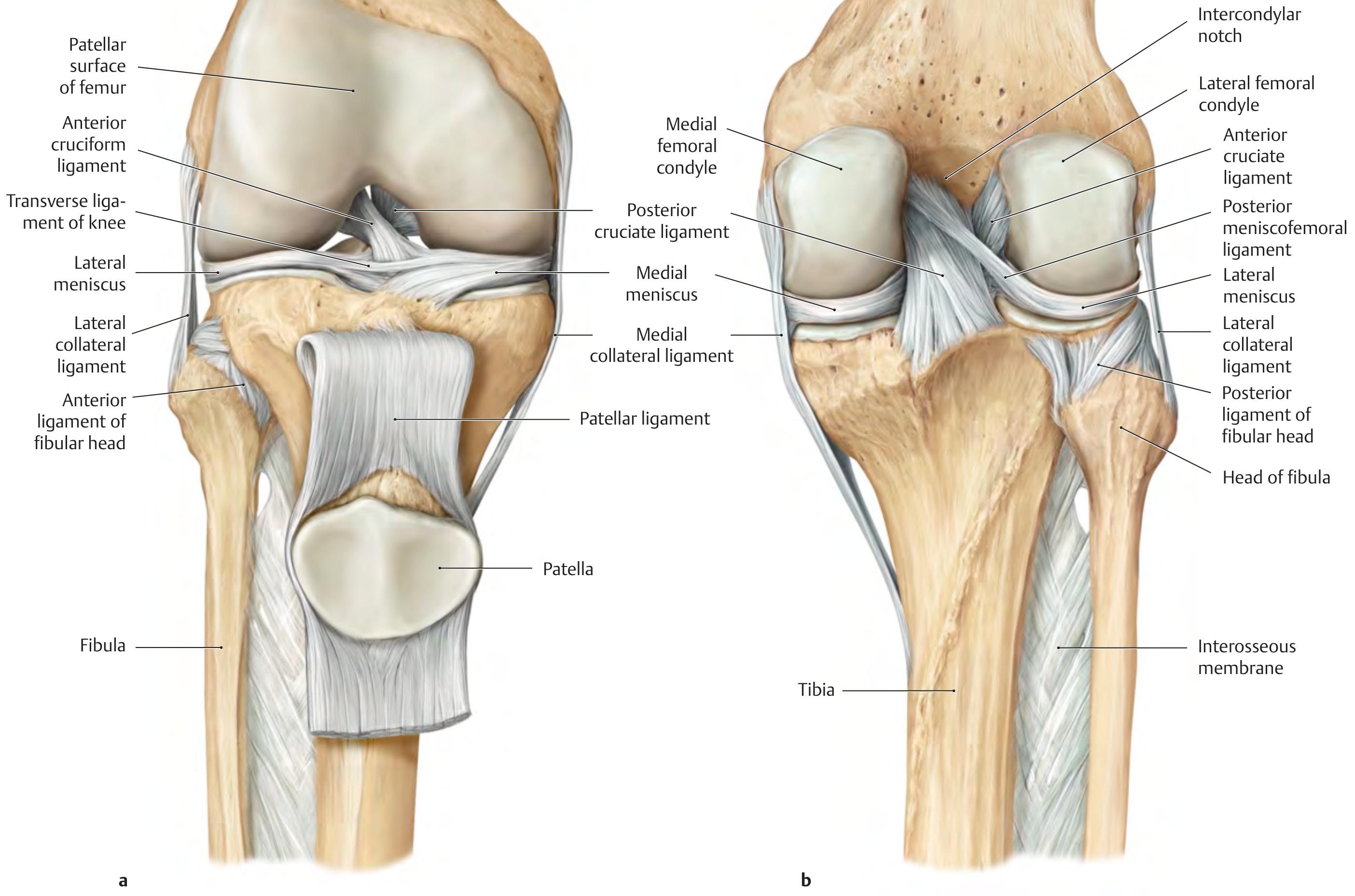
Cruciate ligaments, collateral ligaments, menisci and patellar ligament of the right knee (THIEME Atlas of Anatomy)
Both collateral ligaments stabilize the knee in the coronal plane and are taut in extension, becoming lax in flexion.
Medial (Tibial) Collateral Ligament (MCL)
- A broad, flat ligament - the broader of the two
- Runs obliquely downward and forward from the medial femoral epicondyle (just inferior to the adductor tubercle) to the medial surface of the upper tibia, approximately 7-8 cm below the tibial plateau
- Has superficial and deep portions separated by loose connective tissue
- The deep portion is firmly attached to the joint capsule and the medial meniscus - this anatomical relationship is why MCL injuries often co-occur with medial meniscal tears
- Resists valgus force (inward force on the lateral knee)
Lateral (Fibular) Collateral Ligament (LCL)
- A cord-like, round structure
- Runs from the lateral femoral epicondyle (just above the groove for the popliteus tendon) to a depression on the lateral surface of the fibular head, running obliquely downward and backward
- Separated from the joint capsule by a bursa - has no direct contact with the capsule or lateral meniscus (unlike the MCL)
- Resists varus force (outward force on the medial knee)
- Injured less commonly than the MCL
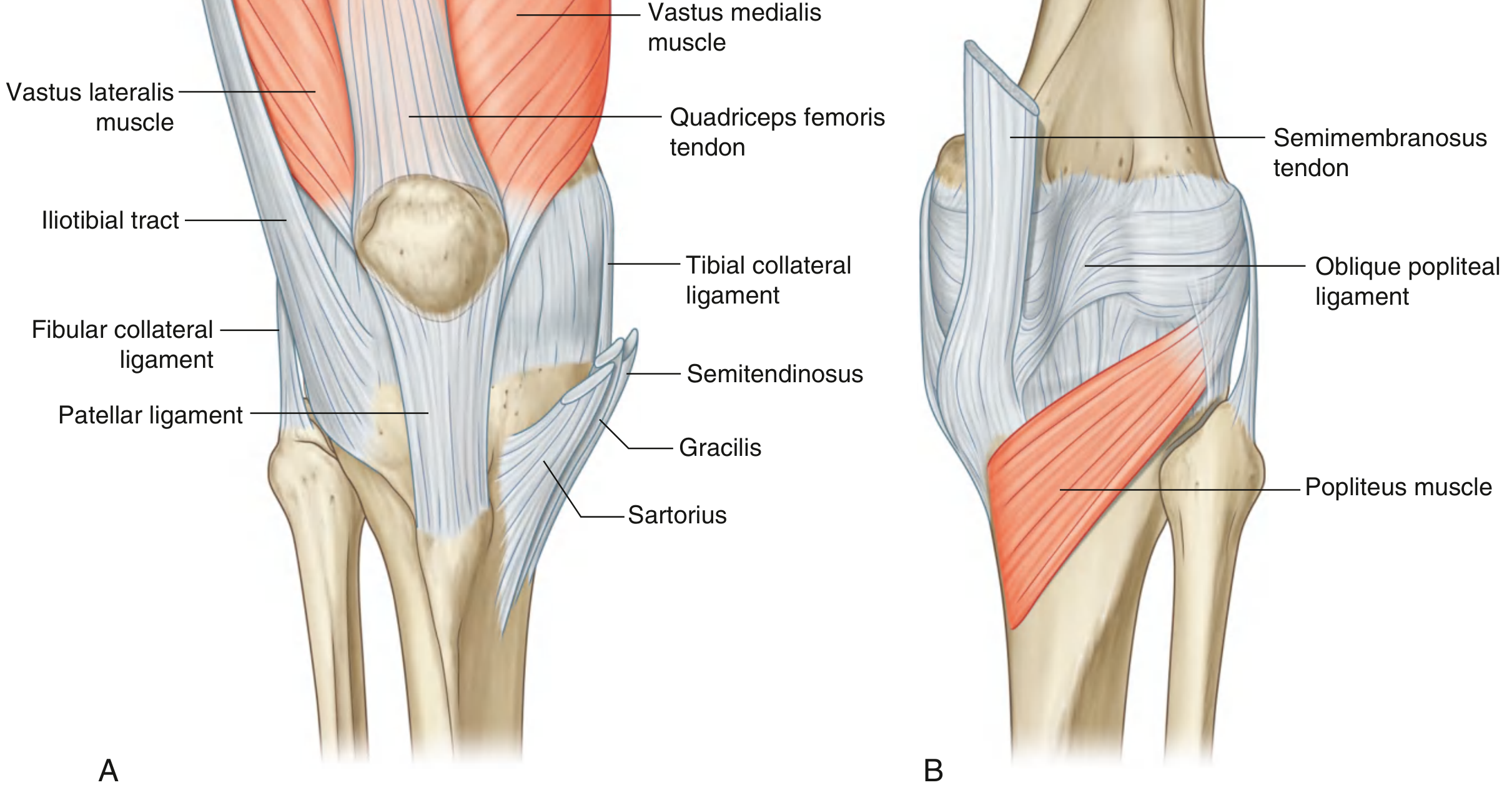
Fibrous membrane of the knee joint capsule - anterior (A) and posterior (B) views (Gray's Anatomy for Students)
3. Cruciate Ligaments
The cruciate ligaments occupy the intercondylar region and cross each other in the sagittal plane - hence the name (Latin crux = cross). They are intracapsular but extrasynovial (covered by a fold of synovial membrane).
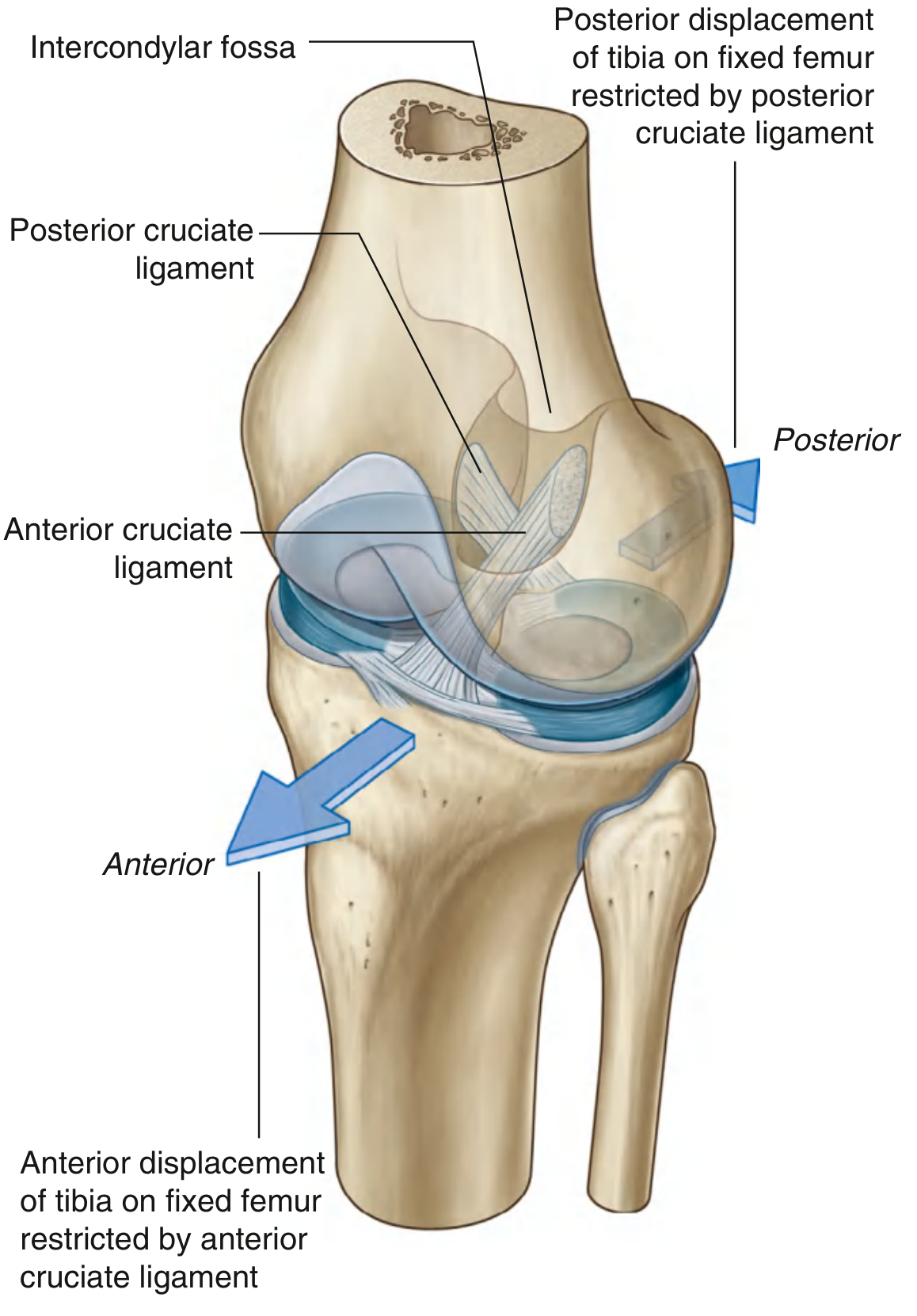
Cruciate ligaments of the knee joint - superolateral view showing directions of restriction (Gray's Anatomy for Students)
Anterior Cruciate Ligament (ACL)
- Attaches to the anterior part of the intercondylar area of the tibia (anterior intercondylar fossa)
- Ascends posteriorly, medially, and superiorly to attach to the medial surface of the lateral femoral condyle (back of the intercondylar fossa)
- Crosses lateral to the PCL as they pass through the intercondylar region
- Function: prevents anterior displacement of the tibia relative to the femur; also limits internal rotation of the tibia and hyperextension
- Two functional bundles exist: anteromedial (taut in flexion) and posterolateral (taut in extension)
- Most commonly injured knee ligament, typically during non-contact cutting/pivoting, sudden changes in direction, or hyperextension with valgus force
Posterior Cruciate Ligament (PCL)
- Attaches to the posterior aspect of the intercondylar area of the tibia
- Ascends anteriorly to attach to the medial wall of the intercondylar fossa of the femur (lateral surface of medial femoral condyle)
- Stronger and thicker than the ACL
- Function: prevents posterior displacement of the tibia relative to the femur ("dashboard injury" mechanism)
4. Posterior Ligaments
- Oblique popliteal ligament: a broad expansion of the semimembranosus tendon that reinforces the posterior capsule
- Arcuate popliteal ligament: a Y-shaped ligament on the posterolateral capsule
- Posterior meniscofemoral ligament (ligament of Wrisberg): connects the posterior horn of the lateral meniscus to the medial femoral condyle, passing behind the PCL
Menisci
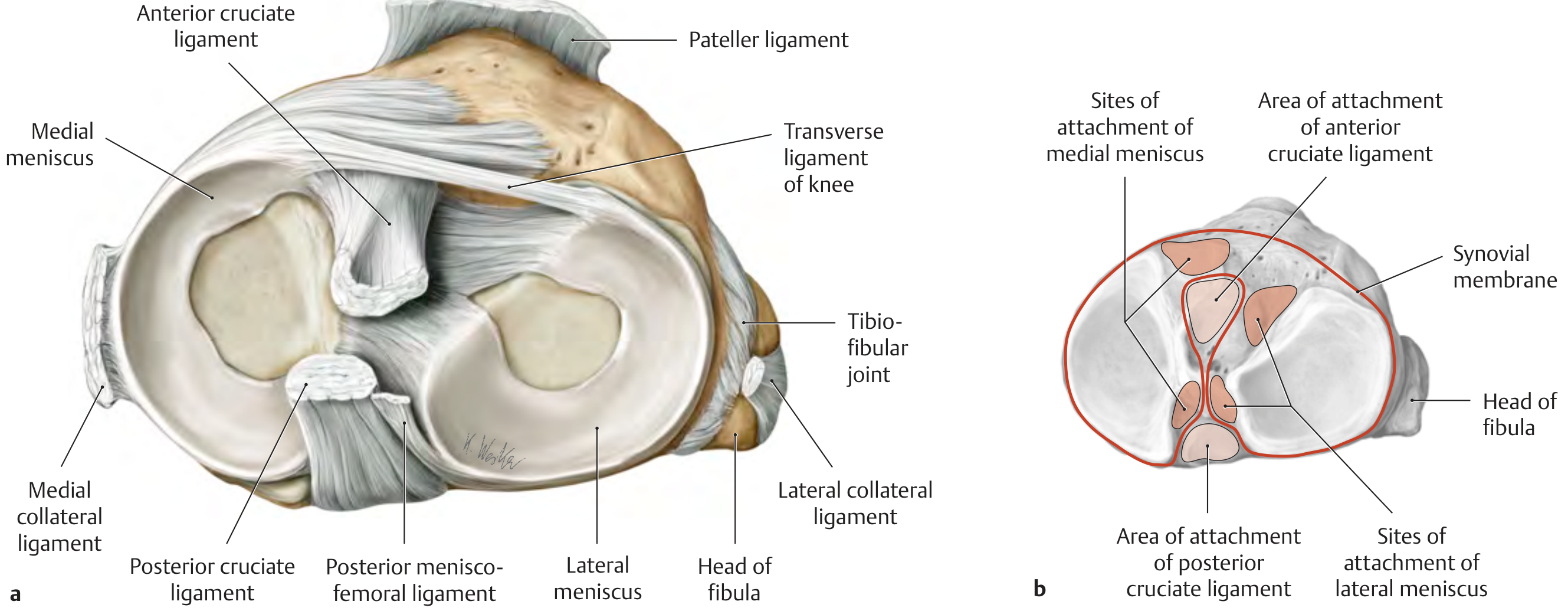
Right tibial plateau from above showing both menisci, cruciate attachment areas, and the transverse ligament (THIEME Atlas of Anatomy)
The menisci are C-shaped (crescent-shaped) fibrocartilaginous discs that sit on the tibial plateau between the femoral condyles and tibial surfaces. They are wedge-shaped in cross-section (thicker peripherally, thinner centrally).
Functions:
- Deepen the tibial articular surfaces to improve congruity with the femoral condyles
- Act as shock absorbers and load distributors (transmit up to 70% of load in extension, 85% in flexion)
- Contribute to joint stability, nutrition of articular cartilage, and proprioception
- Facilitate the "screw-home" locking mechanism
Medial Meniscus
- More semicircular (C-shaped) in outline, wider posteriorly
- Less mobile than the lateral meniscus because:
- Its attachment points (anterior and posterior horns) are more widely spaced on the tibial plateau
- Its peripheral border is firmly attached to the MCL and joint capsule
- The medial meniscus is therefore far more frequently injured (torn) than the lateral meniscus
- The posterior horn is the thickest part and most commonly torn
Lateral Meniscus
- More circular (nearly forms a complete ring) than the medial meniscus
- More mobile because:
- Its horn attachments are closer together
- It has no direct attachment to the LCL or joint capsule
- The popliteus tendon passes between it and the capsule (creating the popliteal hiatus)
- Associated with the posterior meniscofemoral ligament (ligament of Wrisberg)
- The lateral meniscus moves about twice as much as the medial meniscus during knee flexion
Meniscal Attachments
Both menisci are attached at their anterior and posterior horns to the intercondylar area of the tibia by short ligaments. The anterior horns of both menisci are connected to each other by the transverse ligament of the knee.
Retinaculum
The retinaculum forms the fibrous tissue extensions of the quadriceps muscle group that envelop the patella and stabilize it within the patellar groove (trochlea). There are four components:
| Component | Description |
|---|---|
| Medial longitudinal patellar retinaculum | Expansion of vastus medialis running longitudinally along the medial patellar border |
| Lateral longitudinal patellar retinaculum | Expansion of vastus lateralis and iliotibial band along the lateral patellar border |
| Medial transverse patellar retinaculum | Horizontal fibers from the medial patella to the tibial condyle |
| Lateral transverse patellar retinaculum | Horizontal fibers from the lateral patella and iliotibial band to the tibial condyle |
A key component is the medial patellofemoral ligament (MPFL), which runs from the superomedial patella to the medial femoral epicondyle (just anterior and distal to the adductor tubercle). It is the primary restraint against lateral patellar dislocation and provides approximately 50-60% of the medial stabilizing force. The MPFL is torn in virtually all lateral patellar dislocations.
The anterior capsule and retinacula serve primarily to stabilize the patella, alongside the tendons of rectus femoris, vastus medialis, and vastus lateralis at a deeper level, together with the meniscopatellar ligaments.
Bursae
Several bursae surround the knee:
| Bursa | Location |
|---|---|
| Suprapatellar | Between quadriceps tendon and femur; communicates with joint cavity |
| Prepatellar | Anterior to patella (housemaid's knee when inflamed) |
| Infrapatellar (deep) | Between patellar ligament and tibia |
| Infrapatellar (superficial) | Subcutaneous, anterior to tibial tuberosity |
| Pes anserine | Between MCL and the pes anserine tendons (sartorius, gracilis, semitendinosus) |
| Semimembranosus | Deep to semimembranosus tendon; may communicate with joint - forms Baker's cyst |
Vascular Supply and Innervation
Arterial supply is via a rich anastomotic network formed by:
- Descending genicular artery (femoral artery)
- Superior and inferior medial and lateral genicular arteries (popliteal artery)
- Anterior and posterior tibial recurrent arteries
Innervation:
- Branches from the femoral nerve (quadriceps)
- Tibial nerve (posterior capsule)
- Common fibular (peroneal) nerve (anterolateral capsule)
- Obturator nerve (medial capsule)
"Unhappy Triad" (O'Donoghue's Triad)
A classic injury pattern from a valgus force to the knee (e.g., a tackle from the lateral side) disrupts three structures simultaneously:
- Anterior cruciate ligament (ACL)
- Medial collateral ligament (MCL)
- Medial meniscus
This occurs because the MCL is firmly attached to the medial meniscus, and when both are injured by a valgus force, the sudden instability tears the ACL as well.
Locking Mechanism
When standing, the knee "locks" into extension by:
- Rolling and then gliding of the femoral condyles on the tibia as extension progresses
- Medial rotation of the femur on the tibia at full extension - this tightens all ligaments simultaneously
- The center of gravity passing anterior to the knee joint
The popliteus muscle "unlocks" the knee by initiating lateral rotation of the femur on the tibia to break the locked position at the start of flexion.
Sources: Gray's Anatomy for Students (4th Ed.), pp. 713-717; THIEME Atlas of General Anatomy and Musculoskeletal System (pp. 444-468); Bailey and Love's Short Practice of Surgery (28th Ed.), p. 4160
This is a shared conversation. Sign in to Orris to start your own chat.