Insulin
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile a thorough, well-organized response.
Insulin
1. History
The discovery of insulin stands among the most significant events in the history of medicine. Before 1922, all children with type 1 diabetes died within 1-2 years of diagnosis from wasting, infections, and overwhelming acidosis. In 1889, Minkowski and von Mering showed that pancreatectomy in dogs produced a diabetes-like syndrome. In the winter of 1921, Frederick Banting (a surgeon) and Charles Best (a medical student) at the University of Toronto demonstrated that a pancreatic aqueous extract lowered blood glucose in pancreatectomized dogs. Within two months, a more purified extract lowered blood glucose in a young man with diabetes. The 1923 Nobel Prize in Physiology or Medicine was awarded to Banting and John Macleod (Banting controversially split his prize money with Best). - Medical Physiology (Boron & Boulpaep), p. 1520
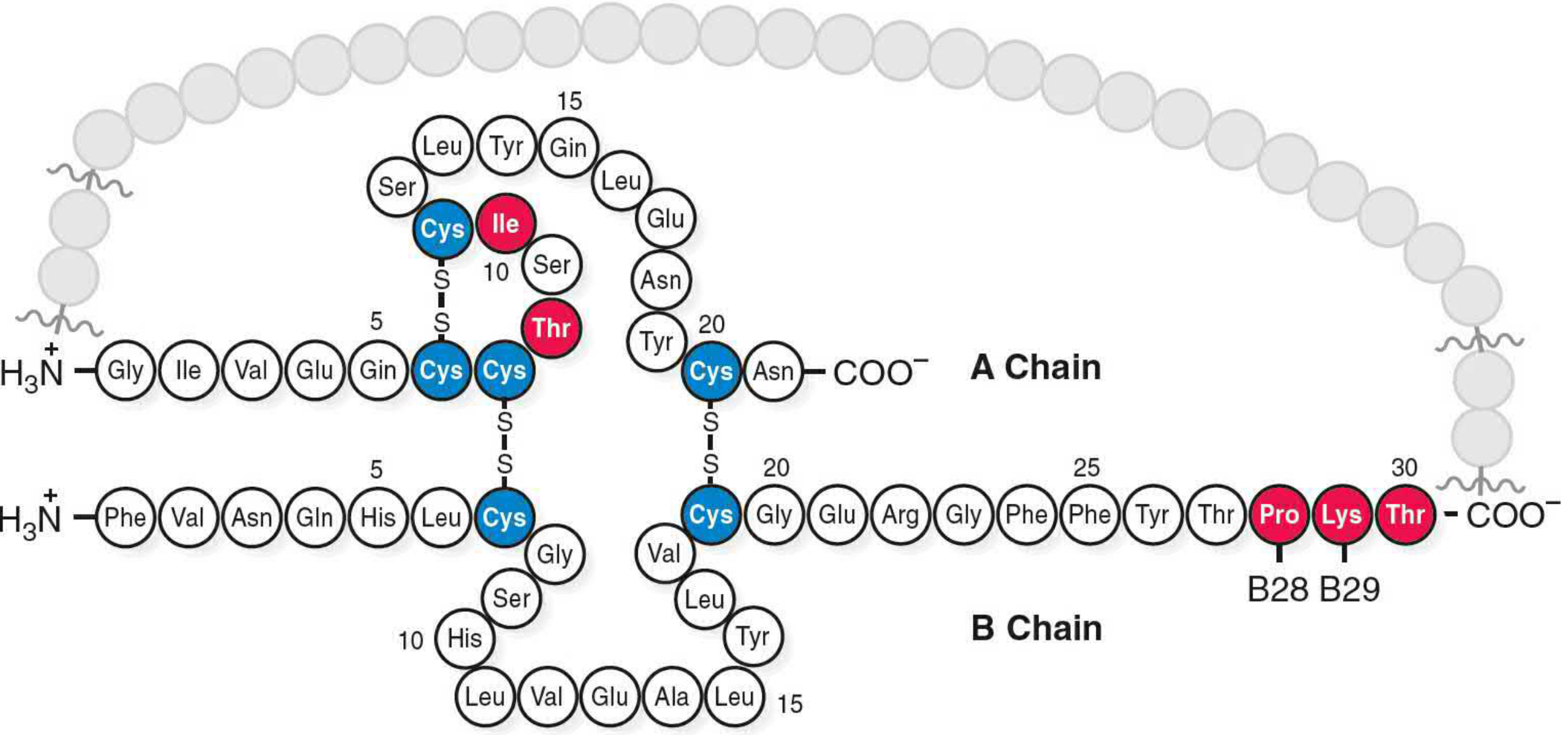
2. Structure and Synthesis
Insulin is synthesized as preproinsulin in the beta cells of the islets of Langerhans. The signal peptide is cleaved to yield proinsulin - a single 51-amino-acid chain. Within proinsulin:
- The B chain occupies the amino-terminal end (30 amino acids)
- The C peptide is the connecting middle segment
- The A chain occupies the carboxy-terminal end (21 amino acids)
Disulfide bonds form between the A and B chains. The C peptide is then proteolytically cleaved, producing equimolar amounts of insulin and C peptide. Because insulin is degraded more rapidly, the C peptide:insulin ratio in circulation is approximately 5-15:1 - making C peptide a useful clinical marker for endogenous insulin production.
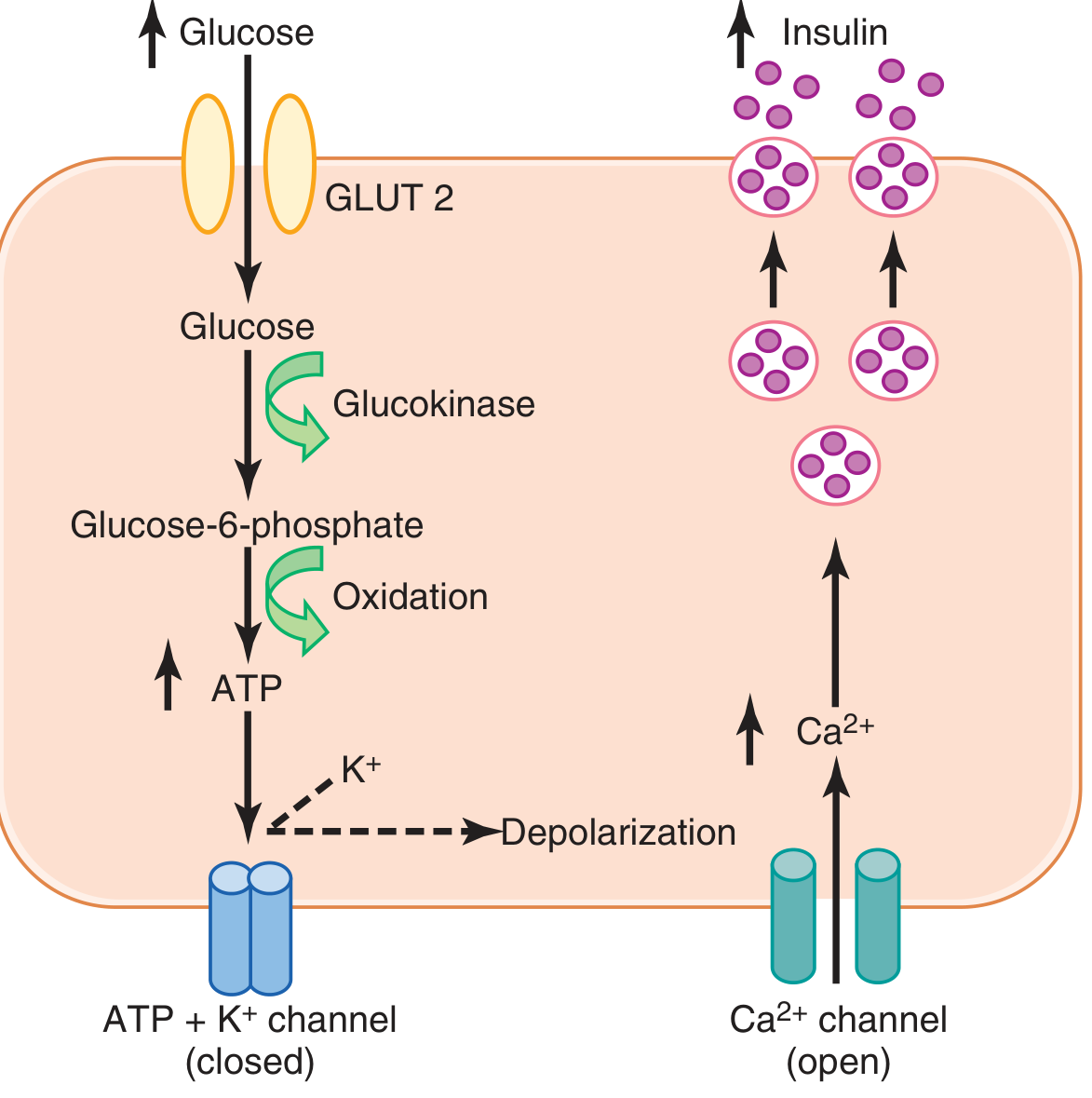
3. Mechanism of Secretion
The primary stimulus for insulin secretion is elevated blood glucose. The beta cell uses GLUT2 (high Km ~15-20 mmol/L) to sense ambient glucose, making uptake proportional to blood concentration. The rate-limiting step is phosphorylation by glucokinase (the "glucose sensor").
Pathway (Guyton & Hall, p. 968):
- Glucose enters beta cell via GLUT2
- Glucokinase phosphorylates glucose → glucose-6-phosphate
- Oxidation generates ATP
- Elevated ATP closes ATP-sensitive K+ channels
- K+ channel closure → depolarization of cell membrane
- Voltage-gated Ca2+ channels open → Ca2+ influx
- Ca2+ triggers exocytosis of insulin-containing vesicles
Stimulators of insulin secretion:
- Glucose (primary), mannose, amino acids (leucine, arginine)
- GLP-1, GIP (incretins), glucagon, cholecystokinin
- Acetylcholine, beta-adrenergic activity, high fatty acids
- Drugs: sulfonylureas, meglitinides (close ATP-K+ channels)
Inhibitors of insulin secretion:
- Somatostatin, insulin itself, islet amyloid polypeptide (IAPP), leptin
- Alpha-adrenergic activity (norepinephrine), chronically elevated glucose
- Drugs: diazoxide, phenytoin, verapamil, clonidine
- Katzung's Basic & Clinical Pharmacology, 16e
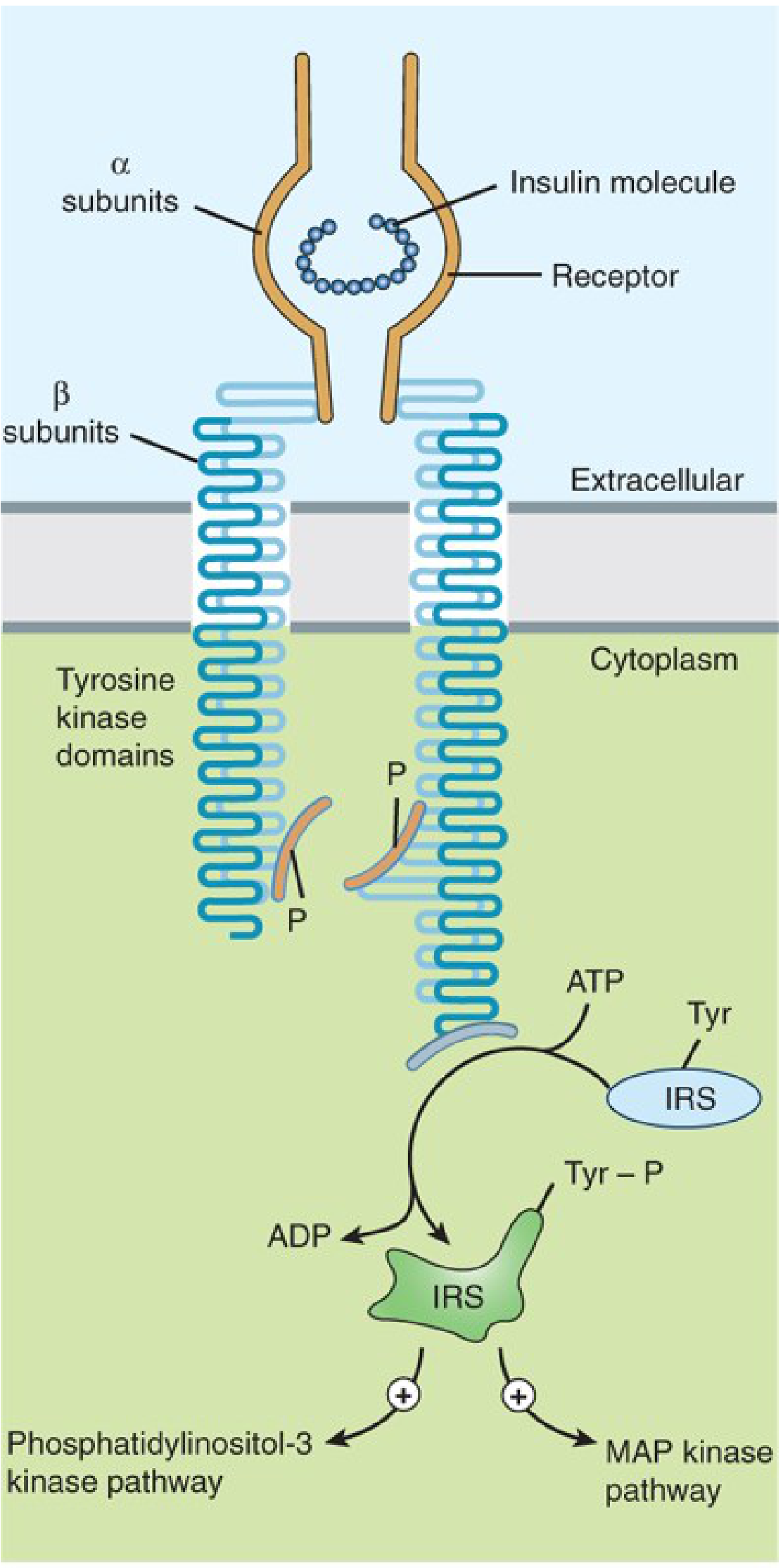
4. The Insulin Receptor
The insulin receptor is a heterotetrameric glycoprotein consisting of two alpha subunits (extracellular, ligand-binding) and two beta subunits (transmembrane + intracellular). The beta subunits contain tyrosine kinase domains.
Signal transduction cascade:
- Insulin binds alpha subunits → conformational change
- Beta subunit tyrosine kinase domains autophosphorylate
- IRS proteins (insulin receptor substrates) are phosphorylated
- PI3-kinase pathway → GLUT4 translocation, glycogen synthesis, protein synthesis, anti-lipolysis
- MAP kinase pathway → cell growth and gene expression
Circulating insulin: Basal levels 5-15 µU/mL (30-90 pmol/L); peak during meals 60-90 µU/mL (360-540 pmol/L).
Half-life: 3-5 minutes. Cleared ~60% by liver (portal route), ~35-40% by kidney. With subcutaneous injection, this ratio reverses (kidney clears ~60%).
5. Metabolic Effects
5a. Carbohydrate Metabolism
| Target | Effect |
|---|---|
| Muscle | Increases glucose transport (via GLUT4 translocation); promotes glycogen synthesis; inhibits phosphorylase |
| Liver | Inactivates liver phosphorylase; activates glucokinase; promotes glycogen synthesis; inhibits gluconeogenesis |
| Fat | Increases glucose transport into adipocytes |
Insulin can increase the rate of glucose transport into resting muscle cells by at least 15-fold. When liver glycogen reaches 5-6% concentration, further glycogen synthesis is inhibited and excess glucose is converted to fat (lipogenesis). - Guyton & Hall, p. 964-966
5b. Fat Metabolism
Insulin is a fat-storing, fat-sparing hormone:
- Promotes fatty acid synthesis in the liver (from excess glucose via pyruvate → acetyl-CoA → fatty acids)
- Activates lipoprotein lipase in adipose capillaries (breaks down circulating triglycerides for uptake)
- Inhibits hormone-sensitive lipase (prevents triglyceride breakdown in adipose tissue)
- Promotes glucose transport into fat cells, generating α-glycerol phosphate for triglyceride re-esterification
In insulin deficiency: Hormone-sensitive lipase becomes uninhibited → massive lipolysis → elevated fatty acids → hepatic ketogenesis → diabetic ketoacidosis. Excess acetyl-CoA cannot enter the TCA cycle and is diverted to ketone bodies.
5c. Protein Metabolism
Insulin is anabolic for protein:
- Increases amino acid transport into cells
- Increases ribosomal protein synthesis
- Inhibits protein catabolism (proteolysis)
- Inhibits gluconeogenesis from amino acids (conserving protein stores)
In insulin deficiency, protein catabolism increases dramatically, amino acids flood the plasma, urea excretion rises, and wasting occurs - one of the most severe consequences of untreated diabetes. Insulin and growth hormone act synergistically to promote growth; neither alone produces significant growth in a depancreatized/hypophysectomized animal. - Guyton & Hall, p. 966-967
5d. Brain Actions
Insulin may act on hypothalamic POMC neurons to reduce food intake and suppress hepatic glucose production and systemic lipolysis - a central regulation of energy balance not requiring direct glucose uptake into neurons (the brain uses GLUT3, not GLUT4, and is largely insulin-independent for glucose uptake).
6. Counter-Regulatory Hormones
The following hormones oppose insulin's effects:
Glucagon (primary), epinephrine, glucocorticoids, growth hormone, thyroxine, somatostatin. In pregnancy: human placental lactogen (HPL).
7. GLUT Transporters
| Transporter | Tissues | Km (mmol/L) | Function |
|---|---|---|---|
| GLUT 1 | All tissues, RBCs, brain | 1-2 | Basal uptake, blood-brain barrier |
| GLUT 2 | Beta cells, liver, kidney, gut | 15-20 | Glucose sensing, insulin release |
| GLUT 3 | Brain, placenta | <1 | Neuronal uptake |
| GLUT 4 | Muscle, adipose | ~5 | Insulin-mediated uptake |
| GLUT 5 | Gut, kidney | 1-2 | Fructose absorption |
- Katzung's Basic & Clinical Pharmacology, 16e
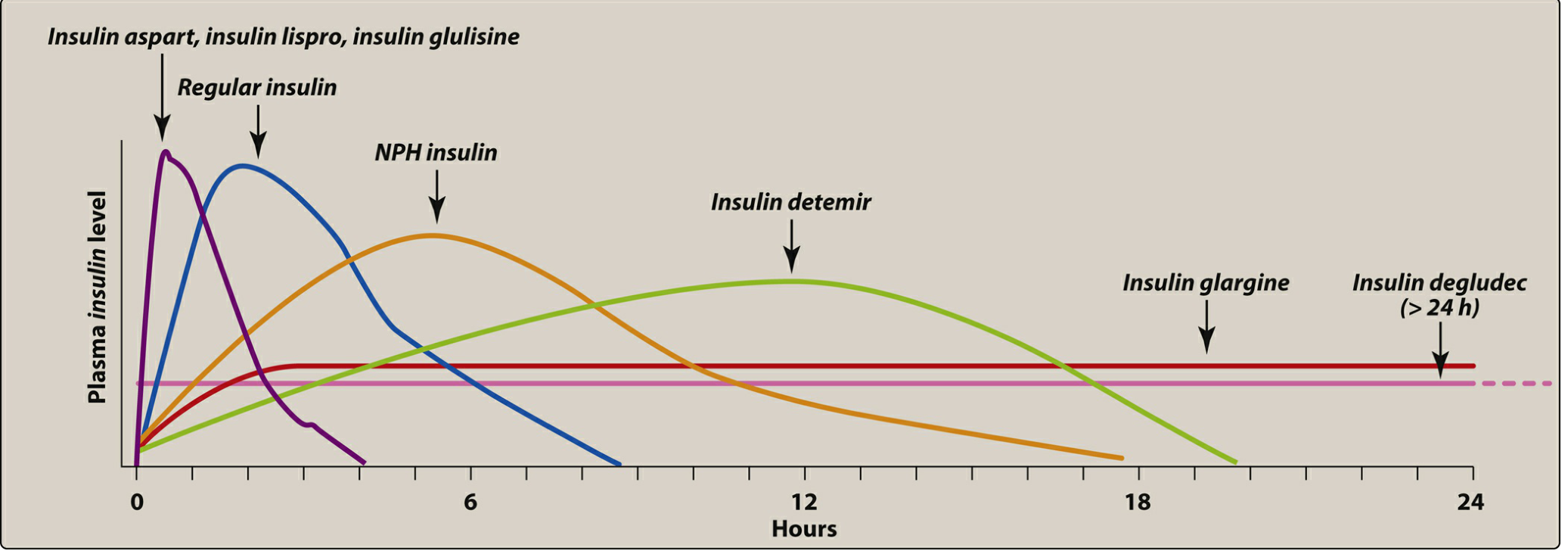
8. Insulin Preparations
| Type | Examples | Onset | Peak | Duration | Use |
|---|---|---|---|---|---|
| Ultra-rapid | Faster aspart, lispro-aabc | 5-10 min | 1-3 hr | 3-5 hr | Prandial |
| Rapid-acting | Lispro, aspart, glulisine | 10-20 min | 1-3 hr | 3-5 hr | Prandial |
| Short-acting | Regular (soluble) | 30-60 min | 2-4 hr | 5-8 hr | Prandial, IV use |
| Intermediate | NPH (isophane) | 2-4 hr | 4-12 hr | 12-24 hr | Basal |
| Long-acting | Glargine | 2-4 hr | 8-12 hr | 22-24 hr | Basal |
| Detemir | 1-2 hr | 4-7 hr | 20-24 hr | Basal | |
| Degludec | 30-90 min | No peak | >42 hr | Basal |
- Harriet Lane Handbook, 23e, Table 10.3
Key mechanisms of long-acting analogs:
- Glargine: Lower isoelectric point → precipitates at injection site → slow release; flat peakless profile
- Detemir: Fatty acid side chain → binds albumin → slow dissociation
- Degludec: Forms multihexamers subcutaneously → depot releases slowly over >42 hours (longest half-life)
Rapid-acting analogs (lispro, aspart, glulisine) differ from regular insulin by amino acid substitutions (e.g., lispro swaps B28-B29 Pro-Lys → Lys-Pro) that prevent self-aggregation into hexamers, allowing faster monomeric absorption.
Regular insulin is the only preparation suitable for IV administration (plus rapid-acting analogs in insulin pumps).
9. Clinical Notes
- Intensive therapy (≥3 injections/day + frequent monitoring) achieves HbA1c ≤7% and significantly reduces microvascular complications (retinopathy, nephropathy, neuropathy), but increases hypoglycemic episodes. Not recommended for elderly, long-standing diabetes, or hypoglycemia unawareness.
- Hypoglycemia is the main adverse effect. Signs: sweating, tremor, tachycardia, confusion, seizure, coma.
- Insulin resistance: Aberrant serine/threonine phosphorylation of IRS or insulin receptor beta subunits causes functional receptor down-regulation. Glucocorticoids lower insulin receptor affinity; excess growth hormone can also cause resistance.
- C peptide is used clinically to distinguish endogenous insulin production (elevated in insulinoma, type 2 DM) from exogenous insulin administration (low C peptide + high insulin = factitious hypoglycemia).
Sources: Guyton & Hall Textbook of Medical Physiology | Katzung's Basic & Clinical Pharmacology, 16e | Lippincott Illustrated Reviews: Pharmacology | Medical Physiology (Boron & Boulpaep) | Harriet Lane Handbook, 23e | Quick Compendium of Clinical Pathology, 5e | Basic Medical Biochemistry, 6e
This is a shared conversation. Sign in to Orris to start your own chat.