Epidural analgesia
Reading File
Finding Sources
Searching PubMed
"epidural analgesia"[MeSH Terms]
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here is a comprehensive overview of epidural analgesia drawn from Miller's Anesthesia (10e), Barash's Clinical Anesthesia (9e), Morgan & Mikhail's Clinical Anesthesiology (7e), Sabiston's Surgery, and Creasy & Resnik's Maternal-Fetal Medicine.
Epidural Analgesia
Definition and Concept
Epidural analgesia involves the injection of drugs (local anesthetics, opioids, or both) into the epidural space to produce segmental pain relief. A catheter is typically threaded through the needle to allow continuous infusion or bolus dosing. Unlike spinal (intrathecal) anesthesia, the drug acts on nerve roots as they traverse the epidural space, producing dose-dependent sensory and motor blockade.
Anatomical Basis
The epidural space lies between the ligamentum flavum posteriorly and the dura mater anteriorly. It contains epidural fat, venous plexuses, and spinal nerve roots. The depth from skin to the epidural space averages 6 cm in adult obstetric patients; in children, a practical approximation is 1 mm/kg (ages 6 months to 10 years).
Key insertion levels:
- Lumbar (L3-L4 or L4-L5): standard for obstetrics, achieving T10-S5 block
- Thoracic (midthoracic): used for thoracic and major abdominal surgery; "gold standard" for post-thoracotomy analgesia
- Caudal: used especially in pediatrics
Technique
Identification of the Epidural Space
The loss-of-resistance (LOR) technique is standard - the needle advances until resistance (from ligamentum flavum) disappears, indicating entry into the epidural space. Either saline or air may be used for LOR, though saline is preferred (air in large volumes >2-3 mL can cause patchy or unilateral block and headache).
Needle Approaches
The image below shows the two main approaches at the thoracic level:
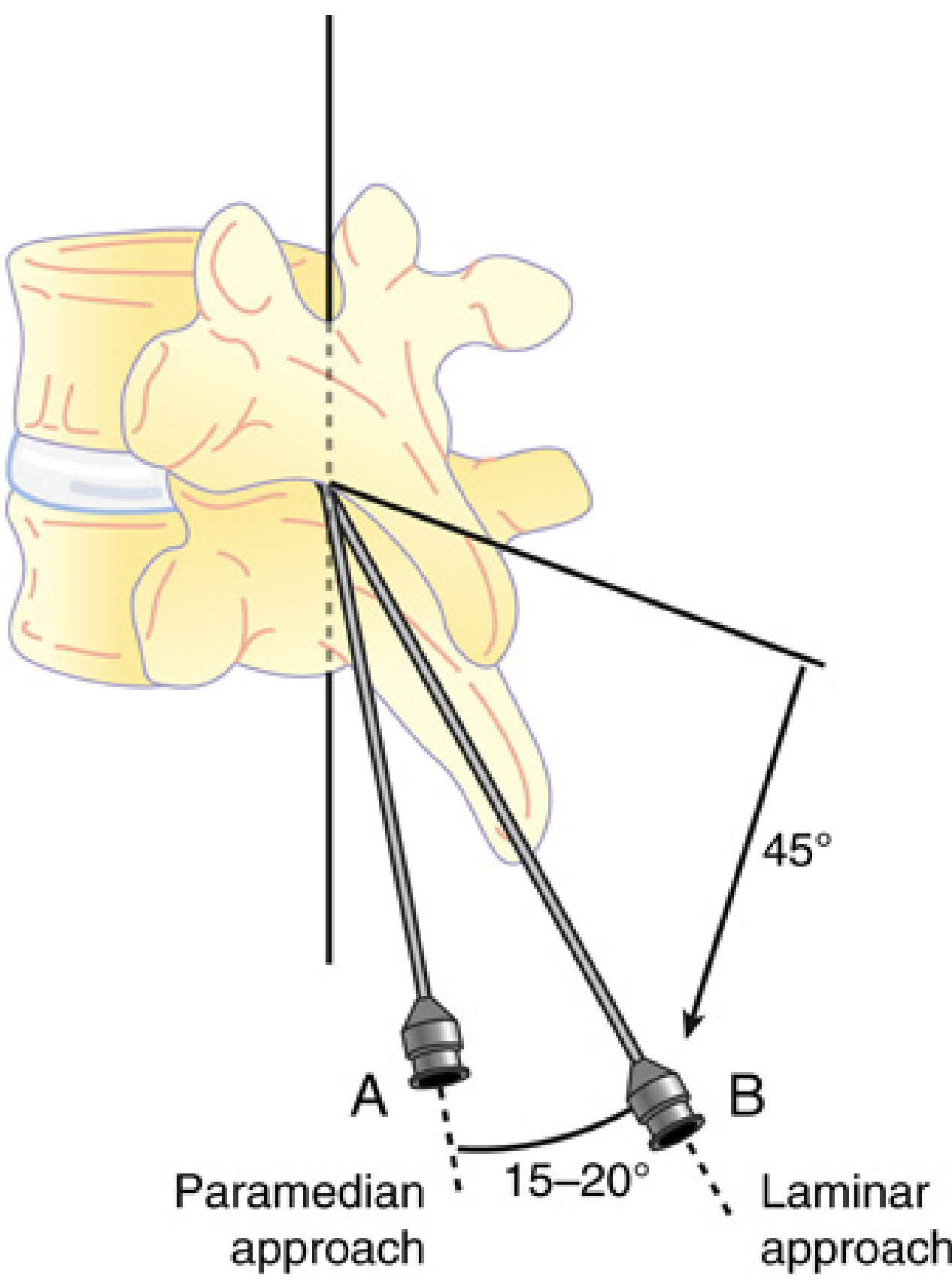
Paramedian approach (A): needle inserted 1 cm lateral to tip of spinous process, advanced rostrally at 45° and medially at 15-20°. Laminar approach (B): inserted next to rostral edge of spinous process at ~45° angle. - Miller's Anesthesia, 10e
- Midline approach: most common at the lumbar level
- Paramedian approach: favored at midthoracic levels; improves success rate; the needle contacts the lamina, then is "walked" rostrally over its edge
- Ultrasound guidance: useful in obese patients or those with poor landmarks; can estimate epidural depth and needle angle, but has not proven as reliable as for peripheral blocks
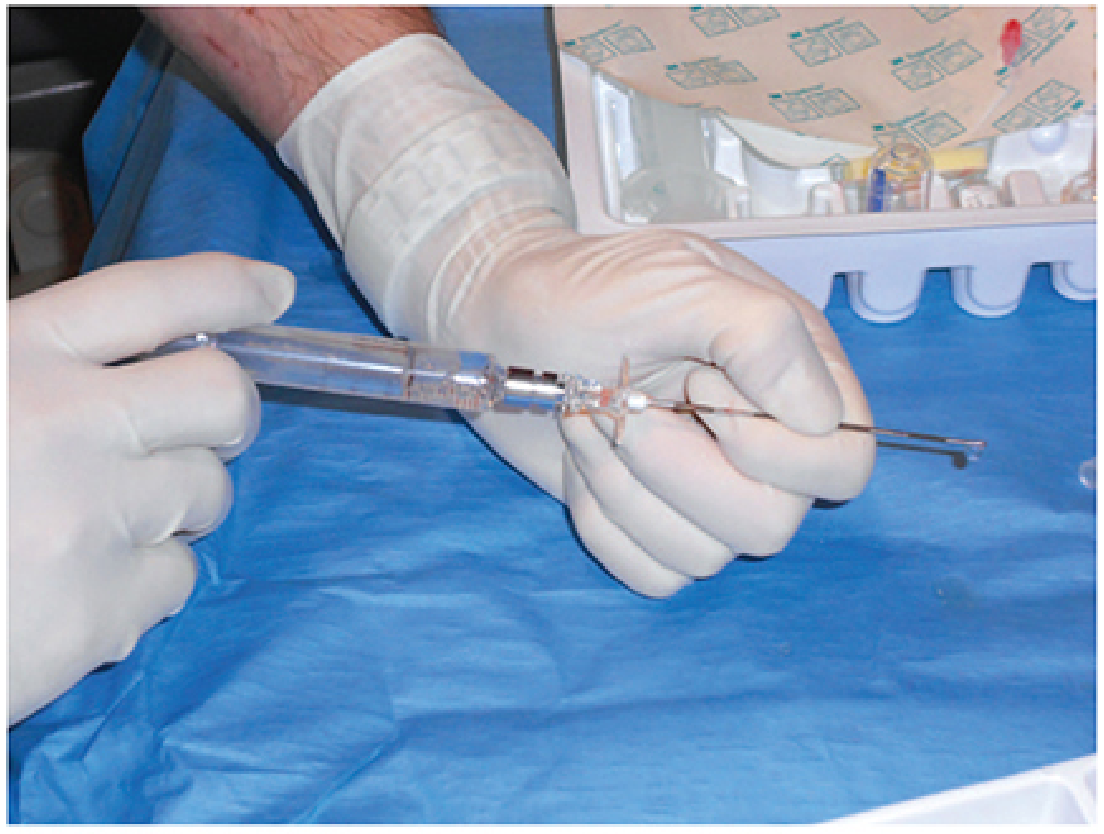
Loss-of-resistance syringe technique. - Morgan & Mikhail's Clinical Anesthesiology, 7e
Catheter Placement
After needle placement, an epidural catheter is threaded 3-5 cm into the space for continuous drug administration. A test dose (e.g., lidocaine + epinephrine) is given to detect intravascular or intrathecal placement before the full dose.
Pharmacology: Drug Combinations
Combining a local anesthetic with a lipophilic opioid produces better analgesia at lower doses than either drug alone - the local anesthetic facilitates entry of the opioid from the epidural space into the CSF.
Local Anesthetics Used
- Bupivacaine: most widely used; long-acting amide; excellent sensory-motor dissociation at low concentrations (<0.1%)
- Ropivacaine: similar to bupivacaine; marginally less motor block at equivalent doses
- Levobupivacaine: comparable to the above two in obstetric trials
- 2-Chloroprocaine: faster onset, shorter duration; useful when rapid conversion to surgical anesthesia is needed
- Lidocaine: intermediate duration
Opioids Used
- Fentanyl (1-2 µg/mL, or 50-100 µg bolus): lipophilic, fast onset
- Sufentanil (0.3-0.5 µg/mL, or 5-10 µg bolus): more potent, longer duration
- Morphine: hydrophilic; longer duration but more side effects (pruritus, nausea, delayed respiratory depression)
Clinical Applications
1. Labor Analgesia (Obstetrics)
Epidural analgesia is the most effective method of labor pain relief. Key points:
- Initiation: ~10 mL of bupivacaine 0.125% + fentanyl 50-100 µg (or sufentanil 5-10 µg) into the lumbar epidural space
- Maintenance options:
- Continuous epidural infusion (CEI): 10-12 mL/h
- Patient-controlled epidural analgesia (PCEA): bolus 5-10 mL, lockout 10-20 min, background 0-10 mL/h; provides greater patient satisfaction, lower bupivacaine dose, less motor block
- Programmed intermittent epidural bolus (PIEB): timed boluses every 30-60 min; superior drug distribution compared to CEI; associated with lower anesthetic dose, greater satisfaction, less motor block
- Operative delivery: sacral blockade achieved with 10 mL bupivacaine 0.25-0.5%, lidocaine 1%, or 2-chloroprocaine 2-3%
Labor epidural analgesia does not increase the risk of cesarean delivery. The only consistent effect is prolongation of the second stage by ~25 minutes. Concerns about dystocia, operative delivery, and autism spectrum disorders in offspring are not supported by controlled evidence. - Morgan & Mikhail's, 7e
2. Post-Thoracotomy Analgesia
Thoracic epidural analgesia (TEA) with local anesthetic-opioid infusions is the "gold standard" for post-thoracotomy pain. A meta-analysis demonstrated that epidural techniques reduce respiratory complications compared with other approaches. The combination of thoracic sufentanil + bupivacaine provides better analgesia with movement and less sedation than either drug alone. - Miller's Anesthesia, 10e
3. Major Abdominal and Other Surgery
Thoracic (but not lumbar) epidural analgesia:
- Facilitates return of GI motility after abdominal surgery by inhibiting sympathetic outflow and reducing spinal reflex gut inhibition
- Decreases pulmonary infections and complications (confirmed by multiple RCTs and meta-analyses)
- May reduce postoperative myocardial infarction risk by attenuating stress response and redistributing coronary blood flow
- Decreases risk of supraventricular arrhythmias after cardiac surgery
- Reduces overall postoperative mortality by ~30% (meta-analysis of 141 trials, 9,559 patients) vs. systemic opioids - Miller's Anesthesia, 10e
Key principle: Benefits are maximized when the catheter is placed at a level congruent with the surgical incision dermatomes ("catheter incision-congruent analgesia"), allowing lower doses and fewer side effects. Local anesthetic-based solutions outperform opioid-based solutions for attenuating perioperative pathophysiology.
4. Rib Fractures / Trauma
Current guidelines strongly recommend epidural catheter placement for patients >65 years with ≥4 rib fractures. Epidural analgesia is associated with decreased ventilator days, fewer pulmonary complications, and shorter ICU stay. - Current Surgical Therapy, 14e
5. Patient-Controlled Epidural Analgesia (PCEA)
Postoperatively, PCEA allows individualized dosing and outperforms CEI in patient satisfaction and drug use. Observational data show >90% of patients achieve adequate analgesia. Side effect rates:
- Pruritus: 1.8-16.7%
- Nausea: 3.8-14.8%
- Sedation: 13.2%
- Hypotension: 4.3-6.8%
- Motor block: 0.1-2%
- Respiratory depression: 0.2-0.3%
Contraindications
| Type | Examples |
|---|---|
| Absolute | Patient refusal, raised intracranial pressure, infection at insertion site, active hemorrhage/coagulopathy, severe spinal malformations, intraspinal tumors or tethered cord |
| Relative | History of spinal surgery, spinal fracture/instability near insertion site, maternal septicemia (untreated), hydrocephalus/unstable epilepsy in children |
Complications
Common
- Maternal/systemic hypotension: most common; prevention by prehydration and avoiding supine position
- Post-dural puncture headache (PDPH): from inadvertent "wet tap" (dural puncture); incidence 0.25-9% depending on operator experience; treated with bedrest, caffeine, or blood patch
Serious (Rare but Catastrophic)
- Epidural hematoma: risk is magnified with anticoagulant use; presents with back pain, lower extremity sensory/motor deficits, bladder/bowel dysfunction; requires urgent MRI and decompressive surgery
- ASRA Pain Medicine guidelines govern catheter timing around anticoagulation (LMWH, DOACs, etc.)
- Almost all anticoagulants except unfractionated heparin are contraindicated with an indwelling catheter
- Epidural abscess: presents with back pain after epidural injection; diagnosed by MRI
- Total spinal: massive cephalad spread from inadvertent intrathecal injection of epidural dose
- Local anesthetic systemic toxicity (LAST): from intravascular catheter migration
Combined Spinal-Epidural (CSE) Analgesia
The CSE technique ("needle-through-needle") provides the rapid onset of spinal analgesia with the flexibility of an epidural catheter for prolonged or adjustable block. Commonly used in obstetrics for faster labor analgesia onset and in major surgeries requiring long operating times.
Summary Table
| Parameter | Lumbar Epidural (Obstetric) | Thoracic Epidural (Surgical) |
|---|---|---|
| Level | L3-L4 or L4-L5 | Midthoracic (T4-T9) |
| Block target | T10-S5 | Dermatomes matching incision |
| Typical LA | Bupivacaine 0.0625-0.125% | Bupivacaine/ropivacaine + LA |
| Typical opioid | Fentanyl 1-2 µg/mL | Fentanyl or sufentanil |
| Key benefit | Superior labor analgesia | GI, pulmonary, cardiac protection |
| Major risk | Hypotension, PDPH | Epidural hematoma with anticoagulation |
Sources:
- Miller's Anesthesia, 10e - Chapters 49 & 77
- Barash's Clinical Anesthesia, 9e - Chapter 14-15
- Morgan & Mikhail's Clinical Anesthesiology, 7e - Chapter 41
- Sabiston's Textbook of Surgery - Chapter on Regional Anesthesia
- Creasy & Resnik's Maternal-Fetal Medicine - Chapter on Obstetric Anesthesia
- Current Surgical Therapy, 14e - Rib fractures/trauma section
This is a shared conversation. Sign in to Orris to start your own chat.