exaplain me cardiac cycle in detail
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full detailed answer.
The Cardiac Cycle - A Complete Explanation
The cardiac cycle refers to the sequence of electrical and mechanical events that repeat with every heartbeat, from the beginning of one beat to the beginning of the next. At a resting heart rate of 72 beats/min, one complete cycle lasts approximately 0.833 seconds. At 75 beats/min it is ~800 ms, of which systole occupies ~300 ms and diastole ~500 ms.
Here is the classic Wiggers diagram showing all events together:

The Trigger: Electrical Initiation
Every cardiac cycle begins with a spontaneous action potential fired by the sinoatrial (SA) node, located in the superior lateral wall of the right atrium near the superior vena cava opening. This impulse spreads across both atria and then travels through the AV node, where it is delayed by >0.1 second. This delay is critical - it lets the atria finish contracting and push blood into the ventricles before the powerful ventricular contraction begins.
The atria act as primer pumps for the ventricles. The ventricles are the main power source for circulation.
The Seven Phases of the Cardiac Cycle
The cycle is classically divided into 7 phases (Costanzo's framework):
Phase A - Atrial Systole (Atrial Contraction)
- ECG event: P wave (atrial depolarization)
- What happens: The atria contract, actively ejecting blood through the open mitral and tricuspid (AV) valves into the relaxed ventricles
- About 70% of ventricular filling has already occurred passively before atrial contraction. Atrial systole adds the final ~30% ("atrial kick")
- Left atrial pressure rises, which is reflected as the "a wave" on the jugular venous pulse (JVP)
- The fourth heart sound (S4) can occur here - not audible normally, but heard when ventricular compliance is reduced (e.g. ventricular hypertrophy)
- The SA node narrows the venae cavae and pulmonary vein orifices during contraction, limiting backflow into the veins (though some regurgitation does occur)
- Semilunar valves (aortic and pulmonary): CLOSED
- AV valves (mitral and tricuspid): OPEN
Phase B - Isovolumetric Ventricular Contraction (IVC)
- ECG event: QRS complex (ventricular depolarization)
- What happens: The ventricles begin contracting. Ventricular pressure rises sharply and rapidly
- As soon as ventricular pressure exceeds atrial pressure, the mitral and tricuspid valves snap shut - this produces S1 (first heart sound - "lubb")
- The aortic and pulmonary valves are still closed because ventricular pressure hasn't yet exceeded aortic pressure (~80 mmHg) or pulmonary artery pressure (~10 mmHg)
- Therefore, all four valves are closed - no blood enters or leaves, so ventricular volume stays constant (isovolumetric)
- This phase lasts ~0.05 seconds
- The tension in the ventricular wall increases enormously with no change in fiber length - analogous to an isometric contraction
Phase C - Rapid Ventricular Ejection
- ECG event: ST segment
- What happens: Ventricular pressure finally exceeds aortic pressure (~80 mmHg in left, ~10 mmHg in right). The aortic and pulmonary semilunar valves open
- Blood is ejected rapidly into the aorta and pulmonary artery - this is the fast ejection phase
- Left ventricular pressure peaks at ~120 mmHg; right ventricular pressure peaks at ~25 mmHg
- Aortic pressure also rises rapidly, reaching ~120 mmHg (systolic blood pressure)
- Ventricular volume falls steeply from the End-Diastolic Volume (EDV, ~130 mL) toward its minimum
- AV valves remain closed; semilunar valves are open
Phase D - Reduced Ventricular Ejection
- ECG event: T wave (ventricular repolarization begins)
- What happens: Ejection continues but at a slower rate as the ventricle begins to relax
- Aortic pressure starts to fall as blood runs off into the peripheral arteries
- Ventricular volume reaches its minimum - the End-Systolic Volume (ESV, ~50 mL)
- The ejection fraction (EF) = (EDV - ESV) / EDV = (130 - 50) / 130 ≈ 65% - a key index of ventricular function
- Late in systole, aortic pressure actually slightly exceeds left ventricular pressure, but forward momentum briefly keeps blood flowing forward
Phase E - Isovolumetric Ventricular Relaxation (IVR)
- ECG event: After T wave (electrical silence)
- What happens: Ventricular muscle fully relaxes. Ventricular pressure drops rapidly
- The momentum of ejected blood is overcome; aortic and pulmonary valves snap shut - this produces S2 (second heart sound - "dubb"), the dicrotic notch appears on the aortic pressure tracing
- All four valves are again closed - volume remains constant (isovolumetric)
- This period of protodiastole (~0.04 s) followed by IVR ends when ventricular pressure falls below atrial pressure, allowing the AV valves to open
- Duration: ~0.08 seconds
Phase F - Rapid Ventricular Filling
- ECG event: Isoelectric period (before next P wave)
- What happens: Ventricular pressure drops below atrial pressure; mitral and tricuspid valves open
- Blood that had been accumulating in the atria during systole rushes passively into the ventricles - most of ventricular filling (about 70-80%) happens here
- Ventricular volume increases rapidly; pressure remains low
- The third heart sound (S3) may occur at the peak of rapid filling - physiologically normal in young people, but a sign of heart failure or volume overload in older adults
- The "v wave" on the JVP tracing corresponds to venous filling of the atrium during ventricular systole, followed by rapid descent when the AV valves open
Phase G - Reduced Ventricular Filling (Diastasis)
- ECG event: Late diastole
- What happens: Ventricular filling slows as the ventricle becomes progressively distended
- AV valve cusps drift toward the closed position (but do not close)
- Pressures in the ventricle and atrium equilibrate; flow slows to a trickle
- This phase is shortened disproportionately when heart rate increases (tachycardia mainly steals from diastole, not systole)
- The next P wave fires, triggering atrial systole again, and the cycle repeats
Pressure-Volume Loop of the Left Ventricle
The entire cycle can be visualized as a pressure-volume (PV) loop:
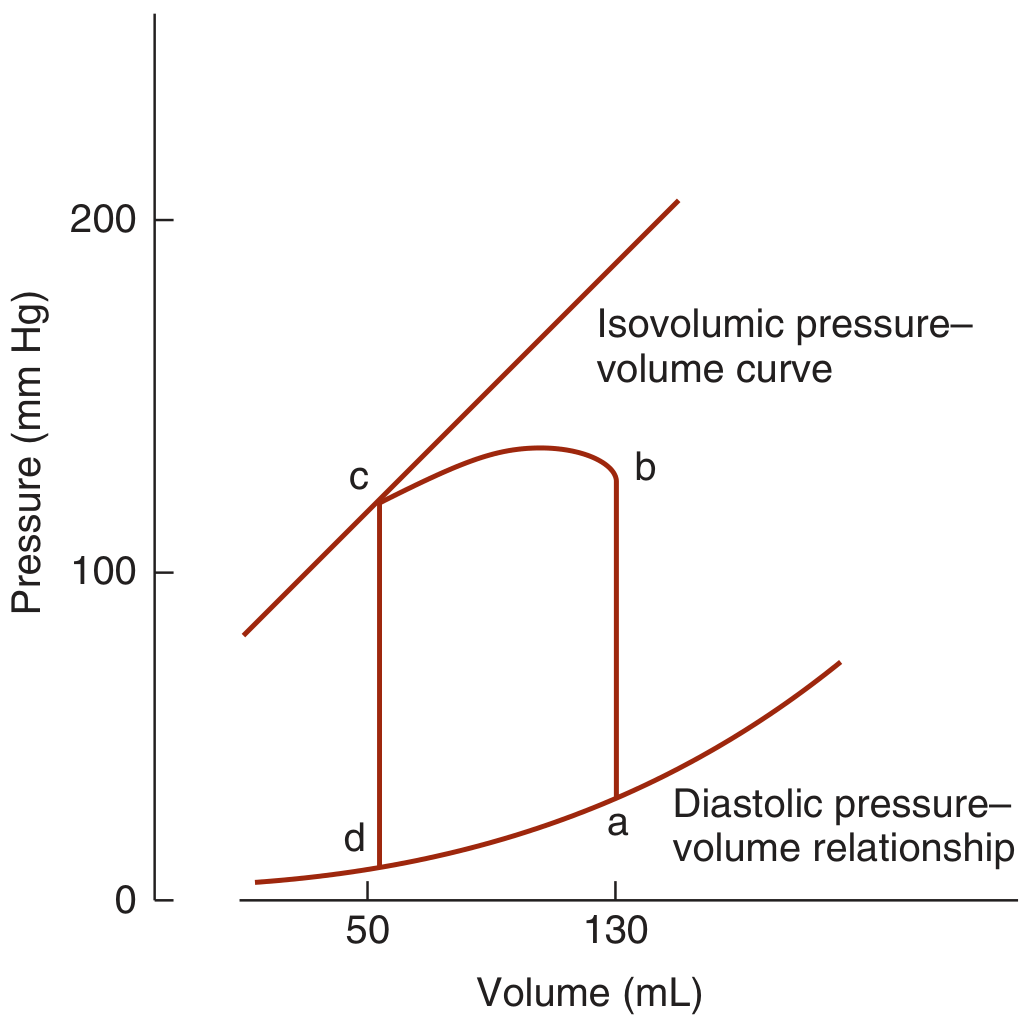
- d → a: Diastolic filling (volume increases, pressure rises slowly)
- a → b: Isovolumetric contraction (pressure rises sharply, volume constant)
- b → c: Ejection (volume falls, pressure rises to peak then falls)
- c → d: Isovolumetric relaxation (pressure falls, volume constant)
The area enclosed by the loop represents the stroke work done by the ventricle.
Summary Table
| Phase | Valves | ECG | Heart Sound | Volume |
|---|---|---|---|---|
| Atrial Systole | AV open, SL closed | P wave | S4 (if abnormal) | ↑ slightly |
| Isovolumetric Contraction | ALL closed | QRS | S1 (lubb) | Constant |
| Rapid Ejection | SL open, AV closed | ST segment | - | ↓↓ |
| Reduced Ejection | SL open, AV closed | T wave | - | ↓ to ESV |
| Isovolumetric Relaxation | ALL closed | After T | S2 (dubb) | Constant |
| Rapid Filling | AV open, SL closed | Isoelectric | S3 (if abnormal) | ↑↑ |
| Diastasis | AV open, SL closed | Isoelectric | - | ↑ slowly |
Key Numerical Values (at rest, HR ~72 bpm)
| Parameter | Value |
|---|---|
| Cycle duration | ~0.833 s |
| Systole | ~0.3 s |
| Diastole | ~0.5 s |
| End-diastolic volume (EDV) | ~130 mL |
| End-systolic volume (ESV) | ~50 mL |
| Stroke volume (SV = EDV - ESV) | ~70-90 mL |
| Ejection fraction (EF) | ~65% |
| Peak LV pressure | ~120 mmHg |
| Peak RV pressure | ~25 mmHg |
| IVC duration | ~0.05 s |
| IVR duration | ~0.08 s |
Effect of Increasing Heart Rate
When heart rate rises (e.g., during exercise), diastole shortens disproportionately more than systole. At triple the normal heart rate, systole occupies ~65% of the cycle vs ~40% at rest. This means the ventricles have less time to fill completely, which can reduce stroke volume at very high heart rates.
Right vs Left Heart
Both sides of the heart go through the same phases, but they are slightly asynchronous:
- Right atrial systole occurs before left atrial systole
- Left ventricular contraction starts before right ventricular contraction
- However, because pulmonary artery pressure (~10-25 mmHg) is much lower than aortic pressure (~80-120 mmHg), the right ventricle ejects before the left
- During inspiration, the aortic valve closes slightly before the pulmonary valve - this produces physiological splitting of S2
Sources: Guyton and Hall Textbook of Medical Physiology; Costanzo Physiology 7th Edition; Medical Physiology (Boron & Boulpaep); Ganong's Review of Medical Physiology 26th Edition; Miller's Anesthesia 10th Edition
This is a shared conversation. Sign in to Orris to start your own chat.