Drugs that control PA pressure
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pulmonary arterial hypertension"[MeSH Terms] AND "drug therapy"[MeSH Terms]
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, well-organized answer. Here it is:
Drugs That Control Pulmonary Arterial (PA) Pressure
Drugs for PAH target three core pathways in the pulmonary vasculature, all of which are deficient or overactive in PAH. A fourth, newer class (activin signal inhibitor) has recently been approved. There are currently 14 FDA-approved PAH therapies in total.
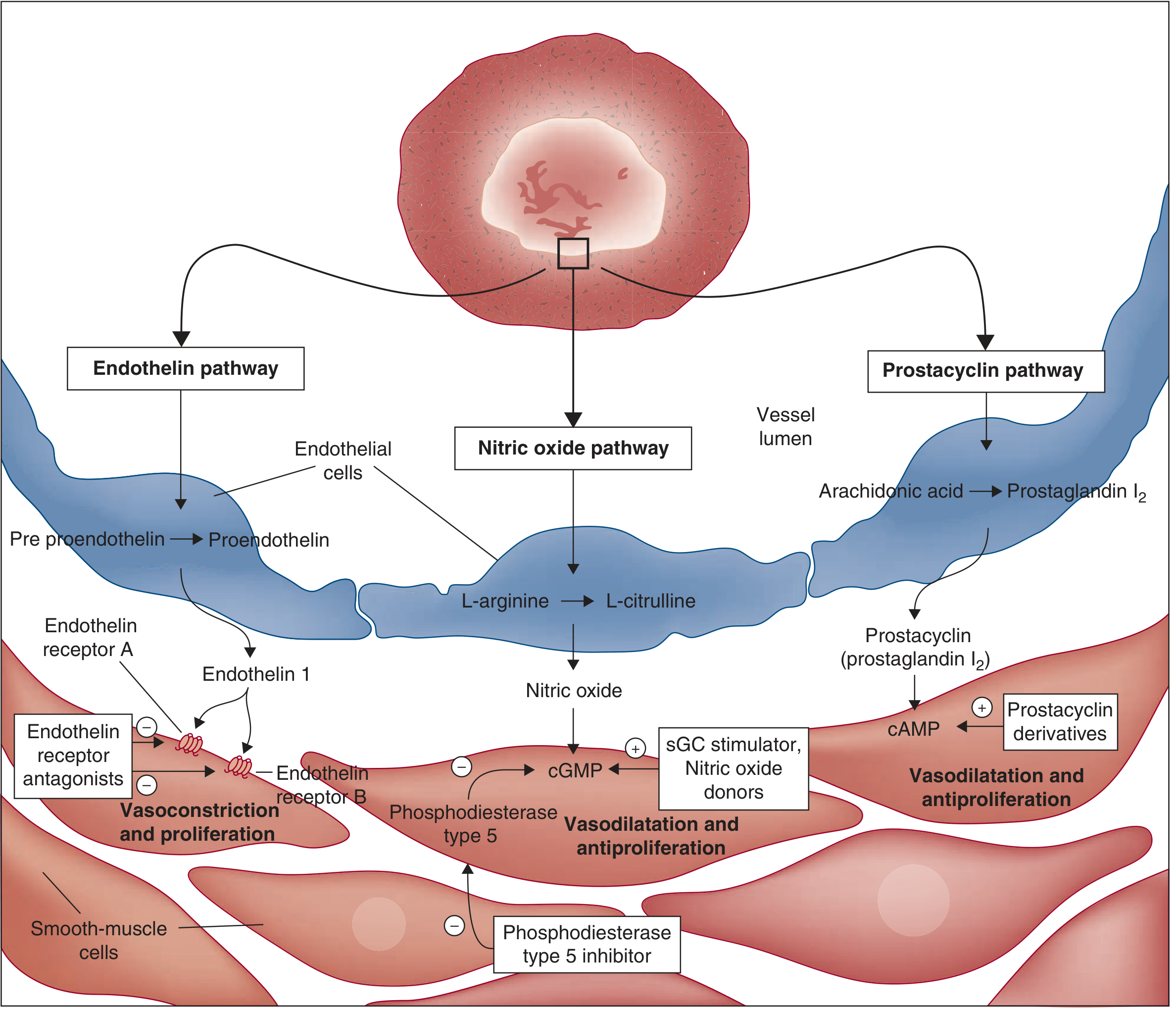
1. Prostacyclin (PGI₂) Pathway
Prostacyclin is deficient in PAH. Replacing or mimicking it raises intracellular cAMP in smooth muscle cells, causing vasodilation and antiproliferation. This is the only class with proven mortality benefit (IV route).
Parenteral Prostacyclin Analogues
| Drug | Route | Notes |
|---|---|---|
| Epoprostenol (PGI₂) | IV continuous infusion | Half-life ~6 min; requires central line; clear mortality benefit in RCTs |
| Treprostinil | IV or SC continuous; inhaled; oral | Half-life ~4 h; more stable; SC causes injection-site pain |
| Iloprost | Inhaled (6–9x/day) | Avoids IV access; pharmacological troughs between doses |
Oral Prostacyclin-Class Agents
| Drug | Mechanism | Notes |
|---|---|---|
| Selexipag | Non-prostanoid IP receptor agonist (prodrug → ACT-333679) | GRIPHON trial: reduced clinical worsening but no mortality benefit; side effects: headache, diarrhea, jaw pain |
| Oral treprostinil | Direct prostacyclin analogue | FREEDOM-EV trial: modest improvement when added to background therapy |
Key side effects of all prostacyclin agents: flushing, headache, jaw pain, diarrhea, nausea, hypotension. Parenteral epoprostenol also reduces systemic vascular resistance by ~50%, limiting dose escalation.
2. Endothelin Receptor Antagonists (ERAs)
ET-1 is a potent vasoconstrictor and smooth muscle mitogen; it is elevated in PAH. ERAs block ET_A and/or ET_B receptors on smooth muscle to reduce vasoconstriction and vascular remodeling.
| Drug | Selectivity | Key Trial | Notes |
|---|---|---|---|
| Bosentan | Non-selective (ET_A + ET_B) | BREATHE-1 | First approved ERA; monthly LFT monitoring required (up to 17% get aminotransferase elevation) |
| Ambrisentan | Selective ET_A | ARIES-1 | Less hepatotoxicity; associated with fluid retention and anemia |
| Macitentan | Non-selective (ET_A + ET_B), optimized binding | SERAPHIN | 45% reduction in composite clinical worsening endpoint over ~85 weeks |
ERAs are teratogenic (Category X). Common side effects: nasopharyngitis, fluid retention, peripheral edema, anemia. Sitaxsentan was withdrawn in 2010 due to fatal hepatotoxicity.
3. Nitric Oxide (NO) / cGMP Pathway
NO from endothelium activates soluble guanylate cyclase (sGC) → cGMP → vasodilation in smooth muscle. Two drug approaches target this:
PDE-5 Inhibitors (prevent cGMP breakdown)
| Drug | Notes |
|---|---|
| Sildenafil | Oral; improves hemodynamics and 6-MWD; also used in erectile dysfunction |
| Tadalafil | Oral, once daily; longer half-life than sildenafil |
Side effects: headache, flushing, visual disturbances, hypotension. Do NOT combine with riociguat (serious hypotension risk).
sGC Stimulator (directly stimulates sGC, NO-independent)
| Drug | Notes |
|---|---|
| Riociguat | Dual mechanism: sensitizes sGC to NO AND directly stimulates sGC independent of NO. Only approved PAH drug also indicated for inoperable CTEPH (Group 4 PH). Approved 2013. |
4. Activin Signal Inhibitors (Newest Class)
| Drug | Mechanism | Notes |
|---|---|---|
| Sotatercept | Fusion protein (Fc-IgG + activin receptor II extracellular domain); traps activin ligands → rebalances TGF-β/BMPR2 pathway, reducing vascular cell proliferation | Phase 3 STELLAR trial: +40 m improvement in 6-MWD vs. placebo in patients already on background triple therapy; reduces PVR. Telangiectasia in ~10% |
5. Calcium Channel Blockers (CCBs)
Used only in the minority (~10%) of patients with a positive acute vasoreactivity test (mPAP drops ≥10 mmHg to <40 mmHg with inhaled NO or adenosine during right heart catheterization).
| Drug | Route |
|---|---|
| Nifedipine | Oral |
| Amlodipine | Oral |
| Diltiazem | Oral (if resting heart rate elevated) |
CCBs are not used in non-responders and are contraindicated in right heart failure. They have no proven benefit in Group 2-5 PH.
6. Supportive / Adjunct Therapy
| Drug | Role |
|---|---|
| Diuretics | Reduce RV preload; manage fluid retention |
| Anticoagulants (warfarin) | Idiopathic PAH (microvascular thrombi); use controversial |
| Digoxin | Adjunct in RV failure |
| Supplemental oxygen | Prevents hypoxic vasoconstriction (target SpO₂ >90%) |
Treatment Strategy Summary
- NYHA FC IV / cardiogenic shock: Start continuous IV epoprostenol (only drug with clear mortality benefit in severe PAH)
- NYHA FC II-III (vasoreactivity-negative): Initial combination oral therapy is preferred - AMBITION trial showed ambrisentan + tadalafil was superior to monotherapy (18% vs. 34% vs. 28% event rate)
- Escalation: Triple therapy (ERA + PDE5i + prostacyclin) is now used in high-risk patients; sotatercept can be added on top of maximal therapy
- Group 2 PH (left heart disease): PAH-specific drugs are not recommended and may be harmful
- CTEPH (Group 4): Riociguat is the pharmacological option; surgery (pulmonary endarterectomy) is preferred
Recent evidence note (2025-2026):
- A network meta-analysis (PMID 38820258, Ann Am Thorac Soc 2024) evaluated sotatercept vs. other add-on PAH therapies, supporting its efficacy as an add-on agent
- A 2026 systematic review (PMID 41678138) addressed transitioning between prostacyclin pathway agents, particularly to oral selexipag
Sources: Fuster and Hurst's The Heart 15th Ed.; Katzung's Basic and Clinical Pharmacology 16th Ed.; Harrison's Principles of Internal Medicine 22E (2025); Braunwald's Heart Disease; Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.