Can you make notes on obstructive jaundice
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
I now have all the information needed to compile comprehensive notes on obstructive jaundice. Here they are:
Obstructive Jaundice — Clinical Notes
1. Definition
Obstructive jaundice (also called cholestatic or surgical jaundice) is the clinical manifestation of impaired flow of conjugated bilirubin through the biliary tree into the duodenum, resulting in accumulation of conjugated (direct) bilirubin in the blood. Jaundice becomes clinically visible when plasma bilirubin rises above ~1.5 mg/dL (three times normal).
— Current Surgical Therapy 14e; Guyton and Hall Textbook of Medical Physiology
2. Pathophysiology
Normal Bilirubin Metabolism
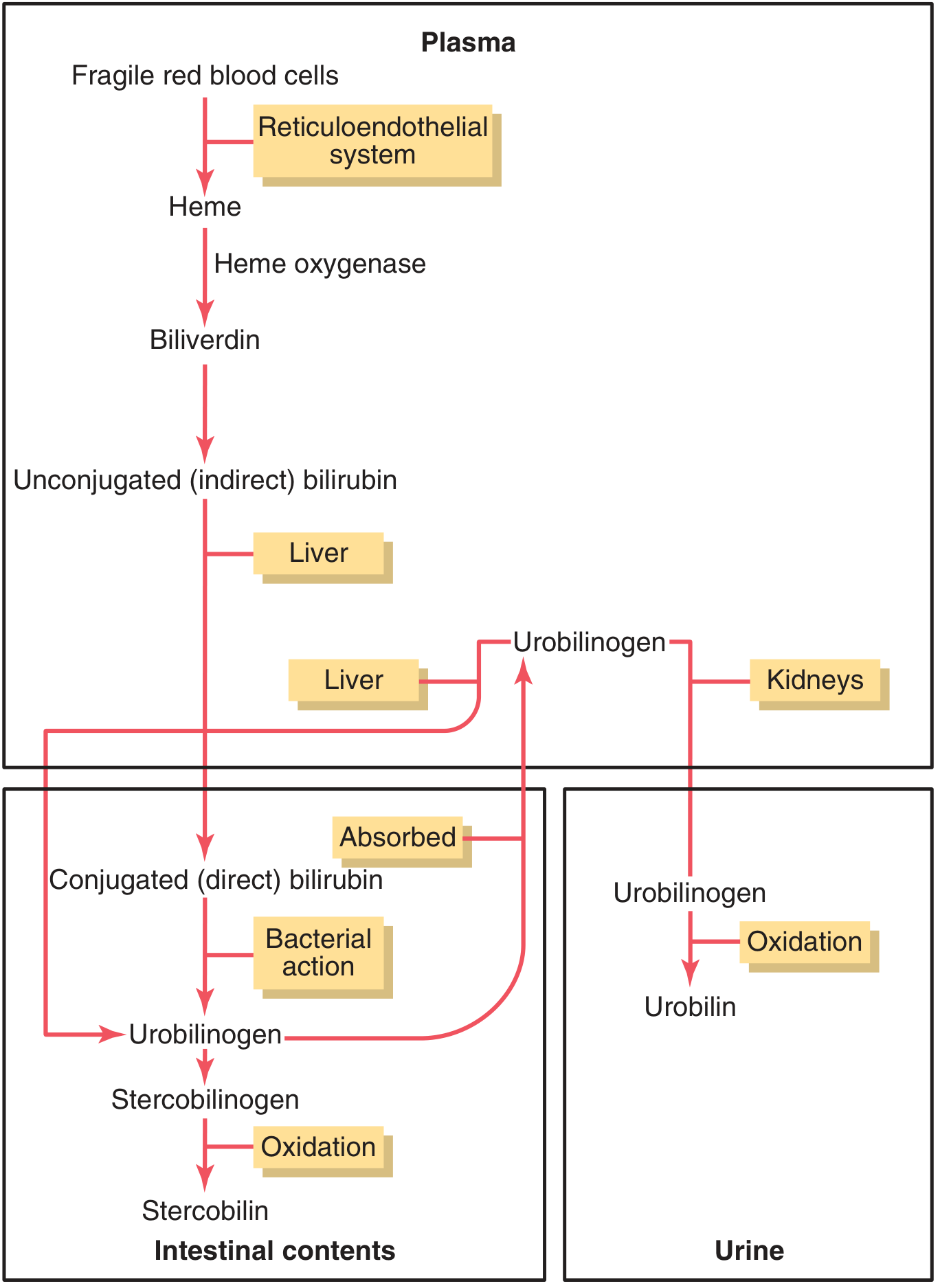
- Aged RBCs are phagocytised by the reticuloendothelial system → heme is cleaved → biliverdin → reduced to unconjugated (indirect) bilirubin
- Unconjugated bilirubin binds albumin in plasma → transported to liver
- In hepatocytes, conjugated (~80% with glucuronic acid) → conjugated (direct) bilirubin → secreted into bile canaliculi
- In the gut, bacteria convert conjugated bilirubin → urobilinogen → stercobilinogen → stercobilin (gives stool its brown colour)
- Some urobilinogen is reabsorbed → liver (enterohepatic recirculation) → ~5% excreted in urine as urobilin
What Happens in Obstruction
When the bile duct is blocked, conjugated bilirubin cannot reach the intestine. It is returned to blood (via rupture of congested bile canaliculi into lymphatics). Therefore:
- Plasma bilirubin is predominantly conjugated (direct)
- No bilirubin reaches the gut → no urobilinogen formed → urinary urobilinogen is absent
- Stools become clay-coloured (acholic) — no stercobilin
- Conjugated bilirubin is water-soluble → excreted in urine → dark urine (bilirubinuria); yellow foam on shaking
- Obstructed bile ducts → progressive dilatation of intrahepatic ducts as intrabiliary pressure rises
— Guyton and Hall Textbook of Medical Physiology; Harrison's Principles of Internal Medicine 22E
3. Causes
Malignant (painless jaundice — most common)
| Tumour | Key Feature |
|---|---|
| Carcinoma of the head of pancreas | Most common malignant cause; Courvoisier sign positive |
| Cholangiocarcinoma | Hilar (Klatskin) or distal |
| Gallbladder carcinoma | Often presents late |
| Ampullary carcinoma | Periampullary; may be resectable |
Benign
| Cause | Notes |
|---|---|
| Choledocholithiasis | Most common overall cause (5–10% of cholecystectomy patients) |
| Primary/secondary sclerosing cholangitis | Beaded appearance on MRCP |
| Benign biliary strictures | Post-surgical, post-inflammatory |
| Choledochal cyst | Congenital; Caroli's disease is a variant |
| Chronic pancreatitis (pseudotumoral) | Compression of CBD |
| Pancreatic pseudocyst | Extrinsic compression |
| Parasites (e.g., Ascaris, Clonorchis) | |
| Hemobilia | Rare; after trauma/intervention |
| Ampullary scars, duodenal diverticulum |
Congenital
- Biliary atresia
- Caroli's disease
— Current Surgical Therapy 14e
4. Clinical Features
Symptoms
- Jaundice (yellowish skin and sclera)
- Pruritus (bile salt deposition in skin)
- Dark urine (bilirubinuria)
- Pale/clay-coloured stools (acholia)
- Fatigue
- Abdominal pain: present or absent is a key clinical discriminator:
- Painful → usually calculous (stones)
- Painless → usually malignancy
Signs
- Jaundice of skin/sclera
- Courvoisier's Law: A palpable, non-tender enlarged gallbladder in a jaundiced patient suggests malignant obstruction rather than stones (because a chronically inflamed/fibrosed gallbladder from calculous disease cannot distend). Exception: empyema of the gallbladder can give a tender mass.
- Hepatomegaly (with malignancy or prolonged obstruction)
- Signs of cirrhosis suggest parenchymal rather than obstructive disease (ascites, spider naevi, gynaecomastia, encephalopathy, Kayser-Fleischer rings)
--- Harrison's Principles of Internal Medicine 22E
If Complicated by Cholangitis
| Syndrome | Components |
|---|---|
| Charcot's Triad | RUQ pain + Fever/rigors + Jaundice |
| Reynolds' Pentad | Charcot's triad + Hypotension + Altered mental status (= severe suppurative cholangitis) |
Reynolds' pentad indicates septic shock and carries near-100% mortality without urgent biliary decompression.
— Harrison's, Washington Manual, Sleisenger & Fordtran's
5. Laboratory Investigations
| Test | Finding in Obstructive Jaundice |
|---|---|
| Bilirubin | Elevated direct (conjugated) >50% of total bilirubin |
| Alkaline phosphatase (ALP) | Markedly elevated (3–4× or more in ~75% of cholestasis); often rises before jaundice clinically apparent |
| GGT / 5'-nucleotidase | Elevated — confirms hepatobiliary origin (not bone) |
| ALT / AST | Mildly elevated (usually well below viral/ischaemic hepatitis levels); can be >3× ULN in choledocholithiasis |
| Prothrombin time | May be prolonged (↓ vitamin K absorption due to no bile) — normalises with vitamin K (distinguishes from parenchymal disease where PT doesn't correct) |
| Urinary urobilinogen | Absent (no bilirubin reaches gut) |
| Urinary bilirubin | Present (dark urine, yellow foam) |
| Serum lipase | May be elevated (associated pancreatitis) |
Key bilirubin thresholds (choledocholithiasis):
- Bilirubin >5 mg/dL → suspect CBD stone
- Bilirubin ≥20 mg/dL → strongly suggests neoplastic obstruction
Van den Bergh reaction differentiates conjugated from unconjugated bilirubin — positive direct reaction in obstructive jaundice.
— Current Surgical Therapy 14e; Harrison's; Guyton & Hall
6. Differentiating Obstructive from Parenchymal Liver Disease
| Feature | Suggests Obstructive Jaundice | Suggests Parenchymal Disease |
|---|---|---|
| History | Abdominal pain, fever/rigors, prior biliary surgery, acholic stools | Viral prodrome, drug/toxin exposure, IVDU, family history of liver disease |
| Examination | High fever, abdominal tenderness, palpable mass | Ascites, spider naevi, gynecomastia, asterixis, encephalopathy, Kayser-Fleischer rings |
| Labs | ↑↑ ALP, direct hyperbilirubinaemia, PT corrects with vitamin K | ↑↑ ALT/AST, PT does NOT correct with vitamin K |
| Urobilinogen | Absent in urine | Present/increased in urine |
— Goldman-Cecil Medicine
7. Imaging Investigations
| Modality | Role |
|---|---|
| Transabdominal Ultrasound (US) | First-line. Identifies biliary dilatation and level of obstruction reliably. Sensitivity for intraluminal stones only ~21–63%. |
| CT Abdomen | Excellent for pancreatic tumours >2 cm. Detects distant metastases, lymphadenopathy. |
| MRCP | Gold standard non-invasive investigation. ~95% sensitivity for biliary obstruction. Test of choice for CBD stones non-invasively. Cannot treat. |
| Endoscopic Ultrasound (EUS) | Excellent for hilar, periampullary, and pancreatic head lesions. Allows FNA (sensitivity 84–91%). Enables staging (vascular invasion, lymph nodes). |
| ERCP | Primarily therapeutic. Defines level/character of strictures. Allows sphincterotomy, stone removal, stenting. >90% cannulation success. |
| PTC (Percutaneous Transhepatic Cholangiography) | Used when ERCP fails or hilar obstruction is proximal. 2% major complication rate. |
— Current Surgical Therapy 14e; Goldman-Cecil Medicine
8. ASGE Risk Stratification for Choledocholithiasis
| Predictor | Clinical Signs | Probability |
|---|---|---|
| Very strong | CBD stone on US; clinical ascending cholangitis; bilirubin >4 mg/dL | High (>50%) → proceed to ERCP |
| Strong | Dilated CBD >6 mm (gallbladder in situ); bilirubin 1.8–4 mg/dL | High if both present |
| Moderate | Abnormal LFTs (other than bilirubin); age >55; dilated CBD on imaging | Intermediate–low (10–50%) → EUS or MRCP first |
9. Management
General Principles
- Treat the underlying cause — relief of obstruction is the primary goal
- Correct coagulopathy with vitamin K (or FFP pre-procedure)
- Antibiotics if cholangitis suspected (broad-spectrum covering gram-negatives and anaerobes)
Endoscopic (ERCP-Based)
- Sphincterotomy: incision of the sphincter of Oddi to facilitate stone passage or stent placement
- Stone extraction: balloon or basket retrieval
- Biliary stenting: plastic (temporary) or self-expanding metal stent (SEMS) for malignant strictures
- Balloon dilation: for focal benign strictures
Indications for ERCP:
- Choledocholithiasis with cholangitis
- Malignant biliary obstruction (palliation or tissue sampling)
- Benign biliary strictures post-surgery
- Biliary ductal injuries
Surgical
- Indicated for resectable malignancy (Whipple's procedure for pancreatic head cancer, hepaticojejunostomy, etc.)
- CBD exploration for stones when ERCP fails
- Surgical biliary bypass (hepaticojejunostomy) for unresectable malignancy when endoscopic palliation fails
Radiological (Percutaneous)
- PTBD (percutaneous transhepatic biliary drainage): when ERCP not feasible (altered anatomy, failed cannulation)
- EUS-guided biliary drainage (EUS-BD): alternative to PTBD with comparable efficacy and lower cost/reinterventions
Management of Cholestasis Complications
- Pruritus: ursodeoxycholic acid (UDCA), cholestyramine
- Fat-soluble vitamin malabsorption (A, D, E, K): supplementation
- Cholangitis: urgent ERCP/biliary decompression + antibiotics
— Sleisenger & Fordtran's; Current Surgical Therapy 14e
10. Complications
| Complication | Mechanism |
|---|---|
| Ascending cholangitis | Stasis of bile → bacterial colonisation → retrograde infection |
| Septicaemia / septic shock | Bacteraemia from biliary tree |
| Acute kidney injury | Sepsis, hepatorenal syndrome |
| Coagulopathy | Vitamin K malabsorption → ↓ clotting factors II, VII, IX, X |
| Malabsorption | Fat and fat-soluble vitamin malabsorption |
| Secondary biliary cirrhosis | Prolonged untreated obstruction → hepatic fibrosis |
| Hepatic abscess | Complication of suppurative cholangitis |
| Pancreatitis | From CBD stones passing through ampulla |
--- Harrison's; Schwartz's Principles of Surgery
Summary: Key Distinguishing Points
| Obstructive Jaundice | Haemolytic Jaundice | |
|---|---|---|
| Bilirubin type | Conjugated (direct) | Unconjugated (indirect) |
| Urine bilirubin | Present (dark urine) | Absent |
| Urine urobilinogen | Absent | Increased |
| Stool colour | Pale/acholic | Normal or dark |
| ALP | Markedly elevated | Normal |
| Pruritus | Present | Absent |
| Gallbladder | May be palpable (Courvoisier sign) | Normal |
Key clinical pearls:
- Painless jaundice + palpable gallbladder = malignancy until proven otherwise
- Painful jaundice + fever = stones ± cholangitis
- ALP rises before visible jaundice in biliary obstruction
- Bilirubin ≥20 mg/dL suggests neoplastic, not calculous, obstruction
- PT correction with vitamin K = obstructive (hepatocyte function intact); non-correction = parenchymal disease
Can you give notes of above topic in terms of surgery
Finding Sources
Finding Sources
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.