Approach to sphenoid sinus according to standard ent textbook
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from Cummings, KJ Lee, and Scott-Brown. Here is the complete, well-structured answer:
Approach to the Sphenoid Sinus
(Sources: Cummings Otolaryngology, KJ Lee's Essential Otolaryngology, Scott-Brown's Otorhinolaryngology)
Anatomy and Ostium Landmarks
The sphenoid sinus is the most posterior paranasal sinus. Its natural ostium drains into the sphenoethmoidal recess (SER) - the space medial and posterior to the superior turbinate, anterior to the anterior sphenoid wall, and lateral to the nasal septum.
Key landmarks (Cummings):
- The ostium is consistently medial to the superior turbinate
- Located approximately halfway to two-thirds up the anterior sphenoid wall
- Situated at 6.2-8.0 cm (average 7.1 cm) from the nasal spine at an angle of 30-34 degrees to the nasal floor
- Always lower than the level of the maxillary sinus roof - following this landmark prevents inadvertent skull base penetration
- Approximately 1.5 cm above the choana
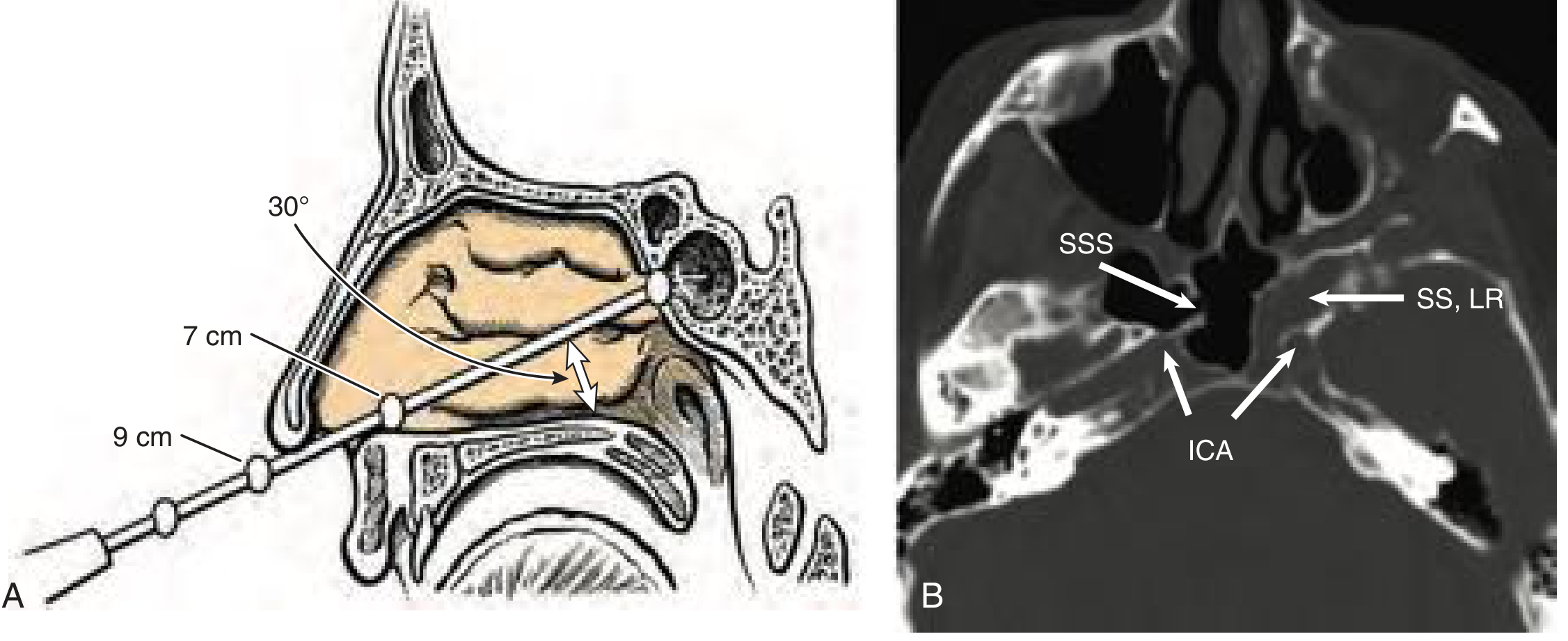
Critical danger: Intersinus septae frequently attach to the bony canal of the ICA. These must be removed without any torsion if resection is needed. The ICA and optic nerve are dehiscent in 20% and 5% of cases respectively.
Surgical Approaches
1. Transnasal (Direct) Approach
Indications: Isolated sphenoid sinus disease, or approaching tumours within the sphenoid skull base. Performed through one nostril.
Steps:
- Middle turbinate is carefully medialized with a Freer elevator (avoid destabilizing the basal lamella)
- The superior turbinate is identified and its inferior half cut sharply at the transition of the vertical to horizontal segment
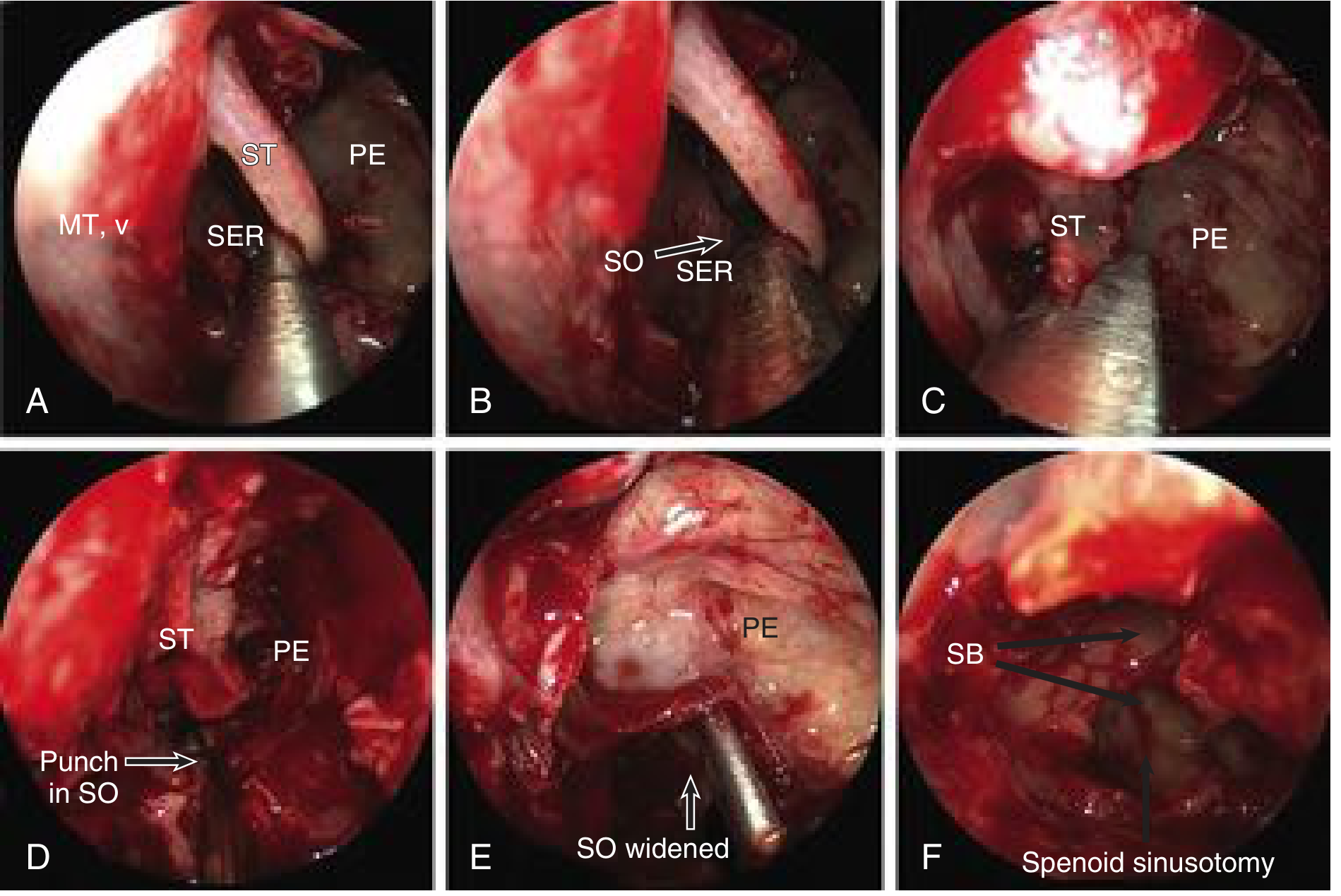
- The sphenoid ostium is visualized in the SER, medial to the superior turbinate attachment
- A stapes curette is used to bluntly palpate and curette the ostium edges
- Ostium enlarged with a 2-mm Kerrison rongeur or sphenoid mushroom punch
- If using a microdebrider - blades directed medially and inferiorly only (never lateral - risks ICA/optic nerve)
- Lowering the anterior sphenoid face: beware the posterior septal branch of the sphenopalatine artery coursing in the mucosa overlying the inferior sphenoid face
If access is narrow: the posterior middle turbinate can be partially removed with microscissors. Initial sphenoidotomy is made with a micro-Kerrison punch at the ostium, enlarged inferiorly avoiding the septal artery.
2. Transethmoidal Approach
Indications: When a sphenoethmoidectomy is to be performed; often done prior to ethmoid skull base dissection.
Steps (KJ Lee):
- Complete posterior ethmoidectomy first
- The superior turbinate is cut sharply at the vertical-horizontal junction to directly visualize the sphenoid ostium (medial to superior turbinate attachment)
- The safest entry is via the natural ostium (not by punching through the posterior wall of the most posterior ethmoid cell)
- A stapes curette bluntly palpates and curettes the ostium edges
- Further enlargement with Kerrison rongeurs and sphenoid mushroom punches
From within the ethmoid, there are two methods (Cummings):
- Enter through the inferomedial part of the most posterior ethmoidal cell (less preferred)
- Formally identify the sphenoid ostium in the SER via the superior turbinate landmark (preferred)
The inferior third of the superior turbinate may be resected for full visualization. Resection of the inferior half does not appear to disrupt olfactory function, but overresection must be avoided as the superior turbinate bears olfactory fibers.
3. Transseptal Approach
Indications: Pituitary adenomas, lesions of the sella/parasellar region, clivus, and parasellar tumours. Provides midline access while protecting lateral structures (ICA, optic nerve).
Steps (Cummings):
- Submucoperiosteal infiltration with ropivacaine 0.75% + epinephrine 1:100,000 (hydraulic dissection)
- Vertical hemitransfixion incision at the caudal edge of the septal cartilage
- Elevation of septal flaps (as in septoplasty)
- Disarticulation of the osseocartilaginous junction - preserve the uppermost part to avoid postoperative dorsal nasal saddling
- Fracture the posterior septal attachment to the perpendicular lamina of the ethmoid
- Resect the posterior septal bone (Jansen-Middleton forceps) to expose the sphenoid rostrum
- Elevate mucoperiosteum of the anterior sphenoid wall until both ostia are visualized
- Open anterior wall with Kerrison micropunch, enlarge with 5-mm diamond bur
- Sphenoidotomy made large enough to introduce a 4-mm endoscope and instrument simultaneously
4. Transseptal-Transnasal (Binostril, Four-Hand) Approach
Described by Stamm et al. (2008). Enables work by two surgeons with four hands without nasal septal perforation.
Key steps:
- Hemitransfixion incision unilaterally with bilateral subperichondrial/periosteal dissection
- Cartilage incised 1 cm posterior to anterior limit, preserving the L-shaped strut of cartilage
- Bony septum removed, inferior portion left as midline landmark
- A pedicled mucoperichondrial flap (based on sphenopalatine artery - the Hadad-Bassagasteguy flap) is elevated on the contralateral side for skull base reconstruction
Ostium Enlargement - Principles
Once the ostium is identified (Cummings):
- Insert a small curette, opening directed first inferiorly and medially - avoid trauma to the nasal septum
- Use a small sphenoid punch or microdebrider to widen
- Avoid circumferential opening - prevents postoperative stenosis; preserve ostium mucosa medially
- Beware of small arterial branches from the sphenopalatine artery inferiorly, medially, or laterally
- A 30-degree angled endoscope helps visualize disease in superior and lateral recesses
- Instrumentation posteriorly, posterolaterally, or superiorly must be done carefully (ICA, optic nerve, skull base)
Classification of Sphenoid Surgery (KJ Lee)
| Type | Description |
|---|---|
| Type I | Identification of ostium without further intervention |
| Type II | Enlargement of ostium to the level of the cranial base and inferiorly to one-half of sinus height |
| Type III | Widening the ostium to its most lateral extent |
Extended Sphenoid Procedures / "Sphenoid Rescue"
Indications: Extensive disease, previous surgical failure, large mucocele, fungus balls, extensive nasal polyposis.
Includes:
- Bilateral extended sphenoidotomies
- Posterior nasal septectomy
- Sphenoid rostrum resection
- Intersinus septectomy
- Goal: create a common sphenoid cavity with broad drainage
Pneumatization Patterns (Scott-Brown)
Relevant for surgical planning - especially for transphenoidal approaches to pituitary tumours:
| Type | Frequency | Description |
|---|---|---|
| Sellar | 90% | Pneumatization posterior to sella turcica |
| Pre-sellar | 9% | Pneumatization up to the anterior sella |
| Conchal | 1% | Shallow, minimal pneumatization with trabecular bone between sinus and sella |
Lateral pneumatization into the pterygoid root creates a lateral sphenoid recess, which runs between the second division of the trigeminal nerve (V2) and the vidian nerve.
Danger Points Summary
- ICA - dehiscent in ~20%; intersinus septae often attach to it
- Optic nerve - dehiscent in ~5%; at risk with lateral microdebrider use
- Sphenopalatine artery (posterior septal branch) - runs over the inferior sphenoid face
- Skull base - stay below the maxillary sinus roof level; use the calibrated probe (7 cm from nasal sill at 30 degrees)
- Olfactory fibers on superior turbinate - avoid overresection
- Cummings Otolaryngology Head and Neck Surgery, Ch. 44 & 177
- KJ Lee's Essential Otolaryngology, Ch. on ESS
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1, Ch. 87
This is a shared conversation. Sign in to Orris to start your own chat.