Abdominal posture
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Here is a thorough explanation of abdominal posture drawing from authoritative anatomy and surgical textbooks:
Abdominal Posture
"Abdominal posture" describes the interplay between abdominal wall muscle tone, pelvic tilt, and lumbar curvature that collectively determines how the trunk is held upright. There are three classical variants:
Three Postural Types
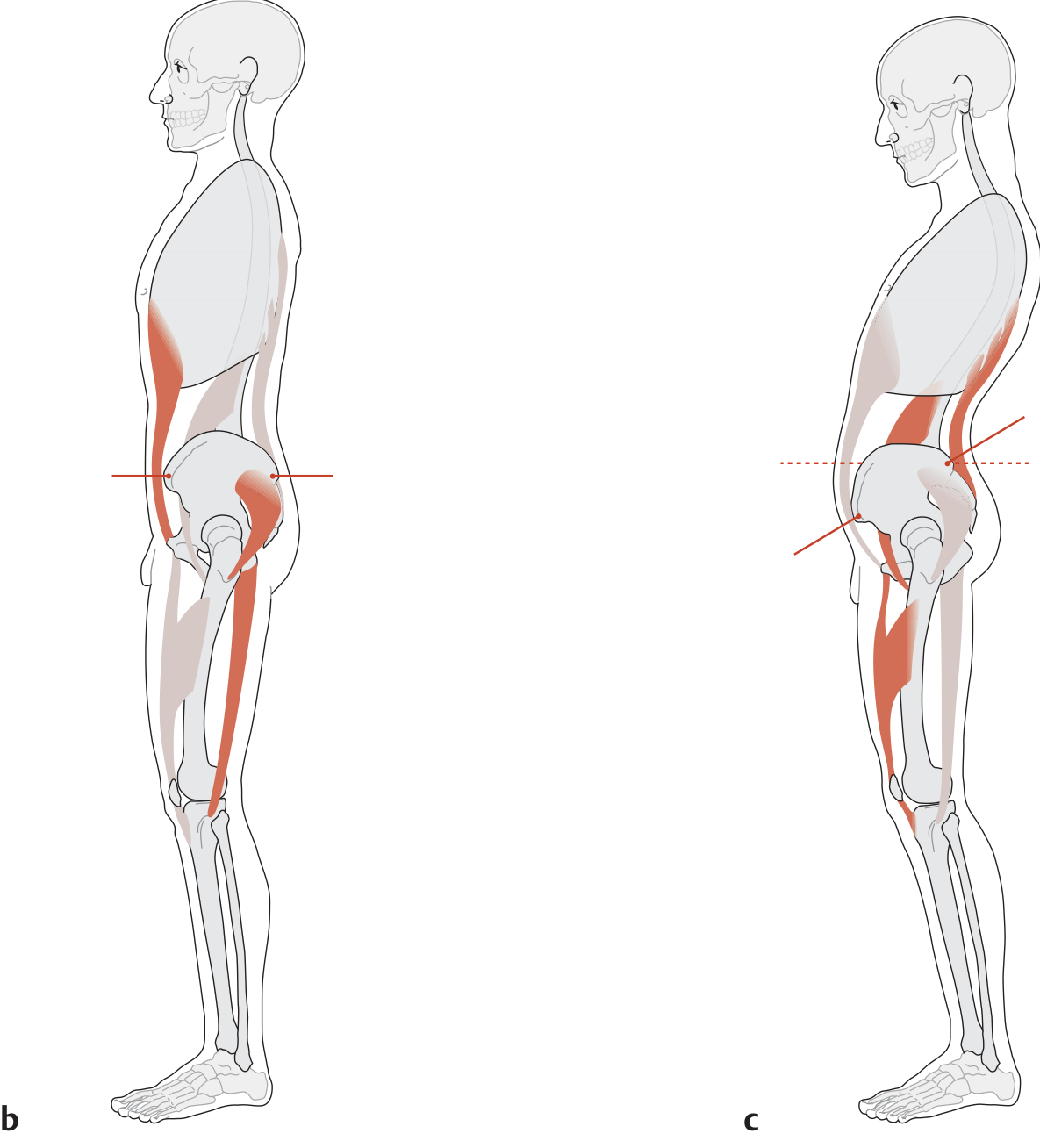
The image below illustrates the active rigid posture (b) vs. the passive slumped (abdominal) posture (c), showing the difference in pelvic tilt and muscle activity:
| Type | Pelvis | Lumbar Spine | Key Muscles |
|---|---|---|---|
| a. Normal active posture | ~12° anterior tilt | Normal lordosis | Balanced ab + back muscles |
| b. Rigid posture ("stomach in, chest out") | ASIS and PSIS at same level (neutral/upright) | Flattened | Abdominal wall, gluteals, hamstrings actively engaged |
| c. Passive slumped posture | Excessive anterior tilt | Accentuated lumbar lordosis | Abdominals lax; intrinsic back muscles shortened |
- THIEME Atlas of General Anatomy and Musculoskeletal System, p. 178
Muscles Responsible for Trunk Flexion (Active Abdominal Posture)
Bilateral contraction of three key muscle groups produces trunk flexion:
- Rectus abdominis - primary trunk flexor; also stabilizes the pelvis during limb movement
- Lateral abdominal muscles (external oblique, internal oblique, transversus abdominis) - provide rotation and transfer transverse forces across the midline via the linea alba
- Psoas major - contributes to trunk/hip flexion
- THIEME Atlas of General Anatomy and Musculoskeletal System, p. 178
Abdominal Core Function in Posture
The abdominal core maintains upright posture through a balance of muscular and connective tissue components:
-
Back muscles + anterolateral abdominal muscles cooperate to uphold the upraised posture and balance gravitational stress
-
Rectus abdominis provides stability to allow limb motion, as well as flexion of the trunk on a fixed pelvis (or vice versa)
-
Linea alba transfers rotation and transverse forces from one side to the other
-
Diaphragm + upper abdominal core support respiration
-
Lower abdominal core + pelvic floor support GI and urinary function
-
Fischer's Mastery of Surgery 8th ed., p. 5985-5986
Passive Slumped (Abdominal) Posture - Clinical Significance
When abdominal muscles are lax or poorly conditioned, the result is the passive slumped posture characterized by:
- Excessive anterior pelvic tilt (pelvis tips forward beyond normal ~12°)
- Accentuated lumbar lordosis due to progressive shortening of intrinsic back muscles
- Shortened iliopsoas (psoas major + iliacus) - this actively reinforces and perpetuates the posture
This postural pattern is clinically important because it is associated with:
- Chronic low back pain
- Pelvic floor dysfunction
- Increased risk of hernias and rectus diastasis (especially after pregnancy, with higher BMI, or older age)
- Abdominal wall laxity from weak or neurologically impaired muscles
Risk Factors for Abdominal Postural Dysfunction
Structural abdominal wall changes that worsen posture include:
-
Pregnancy - mechanical stretching + relaxin/progesterone softening connective tissue
-
Higher age and increased BMI
-
Multiparity, cesarean section, diabetes
-
History of abdominal surgery (incisional hernias, muscle disruption)
-
Fischer's Mastery of Surgery 8th ed., p. 5986
In summary, good abdominal posture depends on a well-conditioned abdominal wall working in balance with the back muscles. When abdominal tone fails, the pelvis tips forward, lumbar lordosis increases, and the passive slumped posture results - with downstream consequences for the spine, pelvic floor, and abdominal wall integrity.
This is a shared conversation. Sign in to Orris to start your own chat.