Distraction osteogenesis
Reading File
Finding Sources
Searching PubMed
"distraction osteogenesis"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content. Let me compile the full answer.
Distraction Osteogenesis
Definition
Distraction osteogenesis (DO) is the mechanical induction of new bone formation by gradually separating two bony surfaces that are pulled apart under controlled tension. Ilizarov described the underlying principle as the "tension-stress effect" - when living tissues are placed under slow, steady tension with adequate stability, they respond with active regeneration and growth.
- Rockwood and Green's Fractures in Adults, 10th ed. (2025)
Historical Background
Gavriil Ilizarov pioneered and refined the technique in the Soviet Union in the 1950s-70s. In the craniofacial skeleton, DO was first applied over 80 years ago but came into widespread clinical use only in the past 25 years. The Ilizarov circular external fixator remains a cornerstone device for limb reconstruction using DO principles.
Biology and Histology
Mechanism of New Bone Formation
New bone in the distraction gap forms through intramembranous ossification (not endochondral), provided the fixation is stable:
- A physis-like structure develops in the gap
- Bone grows in parallel columns extending both proximally and distally from a central growth region called the interzone
- Fibroblast-like cells in the interzone align along the tension-stress vector, elongating parallel to the distraction force
- Surrounding collagen fibers also align parallel to the tension vector
- These fibroblastic cells transform into osteoblasts, depositing osteoid on collagen bundles
- Osteoblasts further differentiate into osteocytes incorporated within the hydroxyapatite (HA) matrix
Cell recruitment for the interzone originates in the periosteum.
Neovascularization
DO produces a dramatic neovascularization effect:
- Fibroblast precursors concentrate around sinusoidal capillaries
- Newly formed capillaries grow very rapidly under tension stress, sometimes outpacing bone formation
- A dense longitudinal vascular network connects to surrounding soft tissue vessels via perforating arteries
- Large vascular channels surround each longitudinal collagen column
- This rich vascularity is essential for intramembranous remodeling
Histology Image (X-ray + Microscopy)
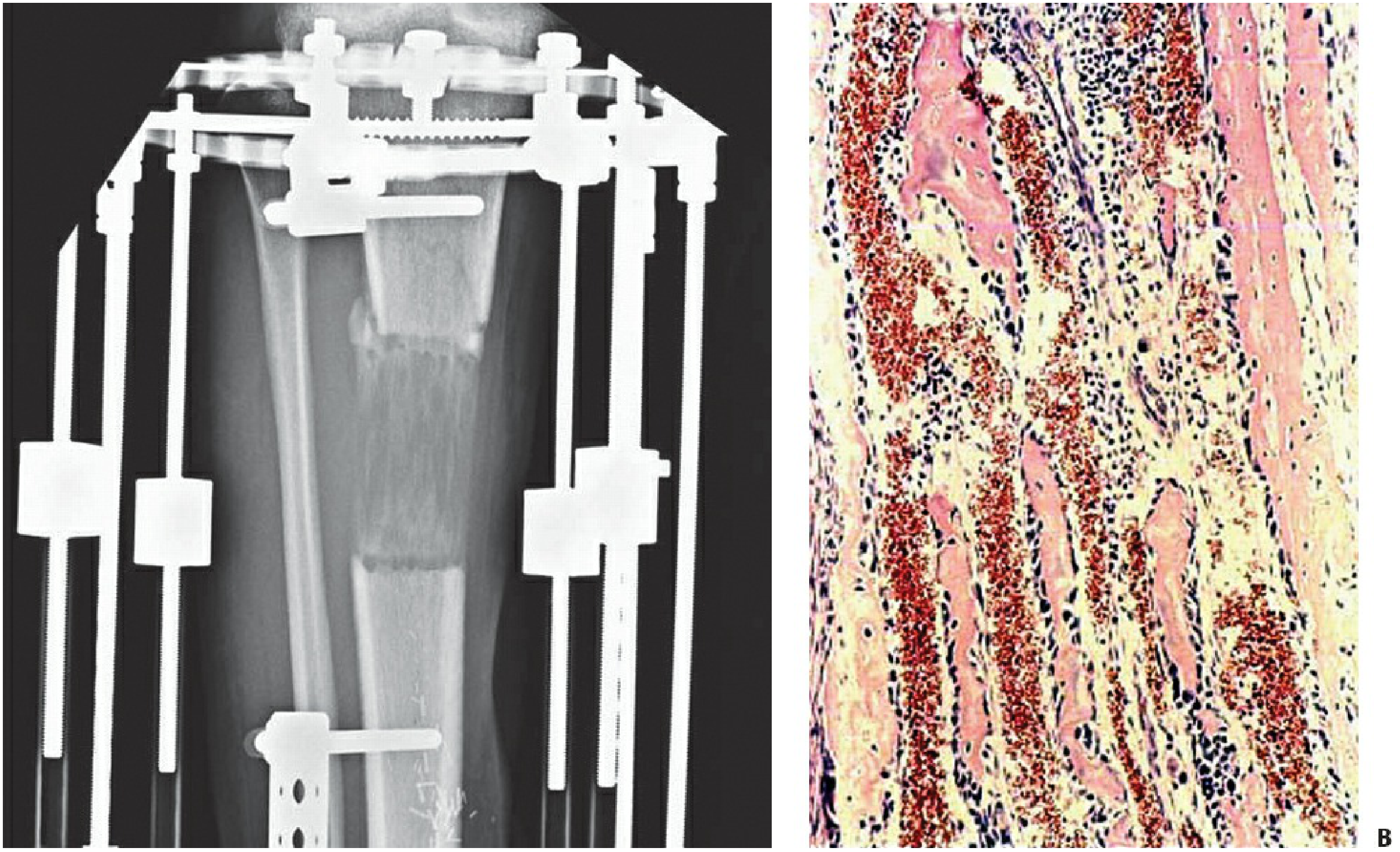
Figure: (Left) Tibia undergoing distraction in a circular frame. (Right) Histology of the regenerate zone - large vascular channels filled with red blood cells are seen longitudinally alongside osteogenic collagen bundles. Rockwood & Green's Fractures in Adults, 10th ed. (2025)
Phases of Distraction Osteogenesis
| Phase | Description |
|---|---|
| Latency phase | 5-7 days after osteotomy before distraction begins; allows early callus formation and periosteal reaction |
| Distraction (activation) phase | Active gradual separation of bone segments at the prescribed rate and rhythm |
| Consolidation (neutralization) phase | Frame maintained after distraction ends; mineralization and remodeling of regenerate bone occurs until cortex forms |
Rate and Rhythm of Distraction
These are critical parameters for successful osteogenesis:
- Optimal rate: 1 mm/day total, as described by Ilizarov
- Rhythm: Divided into at least 4 sessions per day (0.25 mm x 4), not one large distraction
- Constant distraction over 24 hours produces the best regenerate quality
- Too slow (≤0.5 mm/day): premature consolidation - the gap closes before desired length is achieved
- Too fast (≥2 mm/day): disrupts small vascular channels, leads to cyst formation and impaired mineralization
For postoperative metatarsal lengthening (brachymetatarsia), the protocol from Campbell's Operative Orthopaedics (2026) uses 0.25 mm three times daily beginning after a 7-day latency period.
Osteotomy Technique (Corticotomy)
Superior regenerate is achieved with a low-energy corticotomy:
- Osteotomize the anterior, anterolateral, and anteromedial cortices with an osteotome
- Perform closed osteoclasis to the posterior cortex, preserving periosteal tissues
- Preserve periosteum, bone marrow, and surrounding soft-tissue blood supply
- Pre-drill circumferentially to minimize stress risers
The goal is to separate cortical bone while preserving the medullary canal, periosteum, and intramedullary blood supply as much as possible.
Effect of Mechanical Stability
Stability of the fixation device is non-negotiable:
| Stability | Result |
|---|---|
| Stable fixation | Intramembranous ossification proceeds, vigorous regenerate |
| Mechanical instability | Bone resorption, fibrous nonunion, islands of endochondral ossification, vascular cysts |
| Translational shear | Atrophic fibrous nonunion with incomplete vascular channels |
Circular frames (Ilizarov frames) limit abnormal forces when placed in compression, stabilize new blood vessels, and allow intramembranous remodeling to proceed.
Soft Tissue Response (Tension-Stress Effect)
All tissues respond to slow, prolonged tension with metaplasia and differentiation. In order of responsiveness:
- Bone (best responder)
- Muscle
- Ligament and tendons
- Neurovascular structures (slowest, most intolerant of acute distraction)
Muscle response: increase in myofibrils in existing muscle + formation of new muscle via satellite cells → myoblasts → myotubes
Vascular response: smooth muscle proliferation, new elastic structures, neovascularization mirroring prenatal arterial growth
Clinical Applications
Orthopedic
- Limb lengthening (leg length discrepancy, achondroplasia, short stature)
- Bone transport - transport of a bone segment across a defect (e.g., post-tumor resection, osteomyelitis with bone loss)
- Deformity correction - angular and rotational deformities
- Brachymetatarsia - metatarsal lengthening (Campbell's Operative Orthopaedics, 2026)
- Nonunion and delayed union treatment
Craniofacial / Head & Neck
- Posterior cranial vault distraction (PCVD): achieves 20-40 mm advancement vs. 10-15 mm with conventional fronto-orbital advancement (FOA) - almost twice the volumetric gain (Cummings Otolaryngology, 2025)
- Mandibular distraction: for micrognathia, Pierre Robin sequence, hemifacial microsomia
- Midface advancement: Le Fort III level
- Gradual soft tissue adaptation is a major advantage over acute osteotomies - avoids the need for skin/soft tissue grafting
Devices Used
| Device | Features |
|---|---|
| Ilizarov circular frame | Most versatile; multiplanar correction; best stability; preferred for complex deformities |
| Unilateral external fixator | Simpler application; used for straightforward lengthening |
| Intramedullary lengthening nails (PRECICE, STRYDE) | Internal devices; eliminate pin-tract infection; require second surgery for removal |
| Internal distractors (craniofacial) | Buried devices with external activation; used for mandible and cranium |
Complications
Pin/Wire-Related
- Pin-track infection - most common complication
- Pin breakage
- Pin loosening
Bone/Healing-Related
- Premature consolidation (too slow a rate)
- Delayed consolidation / poor regenerate (too fast a rate, instability)
- Fracture through the callus (during or after frame removal)
- Nonunion / fibrous nonunion
- Vascular cysts in regenerate
Deformity
- Axial malalignment (angulation during distraction)
- Joint stiffness (e.g., MTP joint stiffness after metatarsal lengthening)
Soft Tissue / Neurovascular
- Joint subluxation/contracture (soft tissues lag behind bone lengthening)
- Nerve traction injury
- Vascular compromise (rare with appropriate rate)
Device-Related
- Fixator loosening
- Frame-related skin problems
Key Principles Summary
| Parameter | Optimal Value |
|---|---|
| Latency period | 5-7 days |
| Distraction rate | 1 mm/day |
| Distraction rhythm | 4x/day (0.25 mm each) |
| Ossification type | Intramembranous (with stable fixation) |
| Cell source | Periosteum (primary), endosteum, marrow |
| Central growth zone | Interzone |
| Key prerequisite | Preserved periosteum + medullary blood supply |
| Frame requirement | Rigid, stable fixation |
Primary sources: Rockwood and Green's Fractures in Adults, 10th ed. (2025); Campbell's Operative Orthopaedics, 15th ed. (2026); Cummings Otolaryngology Head and Neck Surgery (2025)
This is a shared conversation. Sign in to Orris to start your own chat.