can you give me the difference between anterior inferior and posterior MI with ecg
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I have all the information needed for a thorough, well-illustrated answer. Here it is:
Anterior vs. Inferior vs. Posterior MI - ECG Differences
These three MI types have distinct ECG signatures because each reflects injury to a different wall of the left ventricle, supplied by different coronary arteries.
1. Anterior MI
Culprit artery: Left Anterior Descending (LAD) artery
ECG leads showing changes: V1, V2, V3, V4 (precordial leads)
| Finding | Detail |
|---|---|
| ST elevation | V1-V4 (anteroseptal: V1-V3; anterior: V1-V4; anterolateral: V1-V6, I, aVL) |
| Pathological Q waves | Develop in V1-V4 over hours |
| Reciprocal ST depression | May appear in inferior leads (II, III, aVF) |
| Hyperacute T waves | Tall, broad T waves in V3-V4 (earliest sign) |
ECG - Anterior MI (distal LAD occlusion):
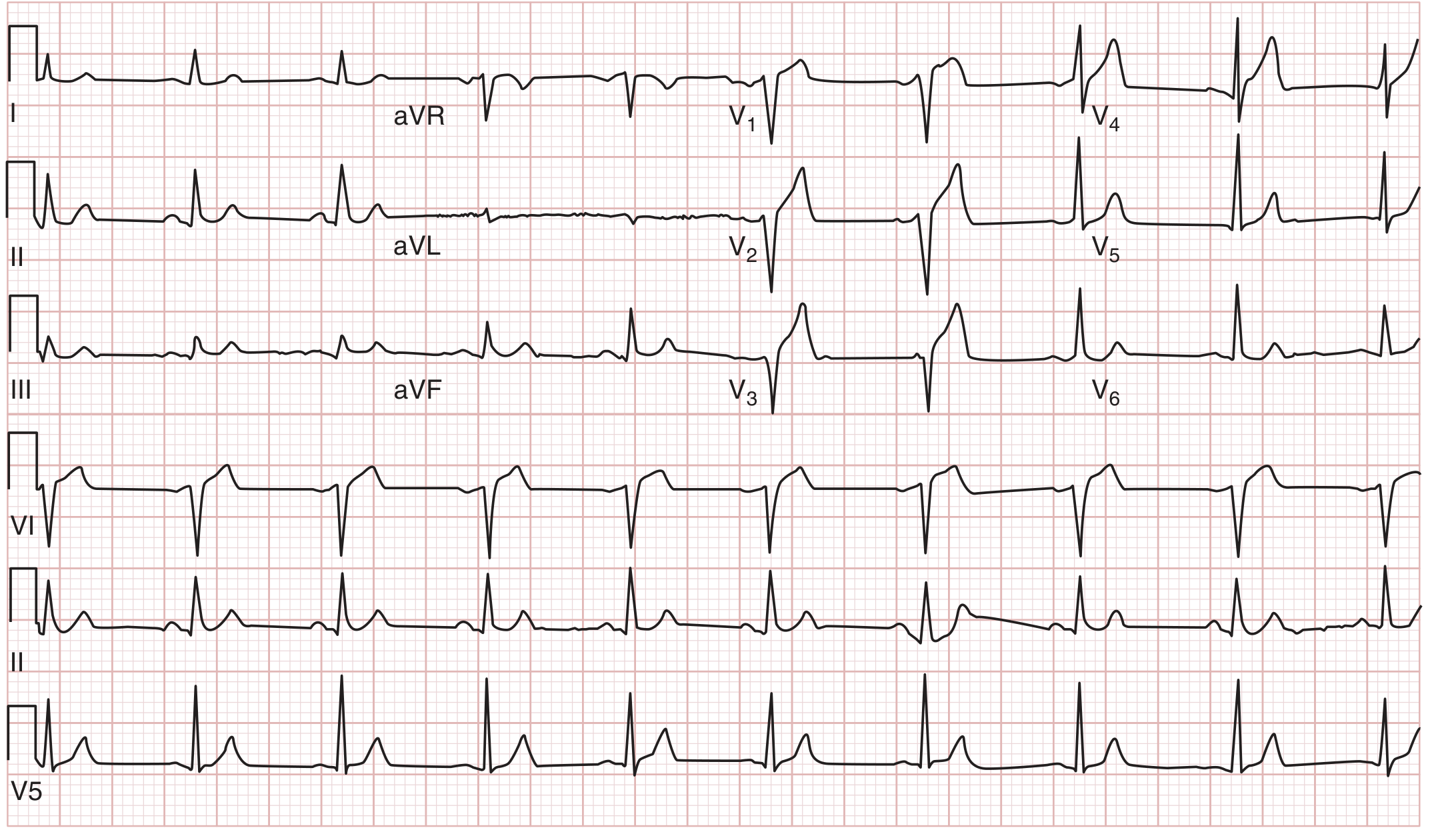
ST-segment elevation in leads I, V1, V2, V3 from 100% occlusion of the distal LAD. Note the absence of reciprocal ST depression in inferior leads, unlike inferior MI. (Tintinalli's Emergency Medicine)
Key tip: Proximal LAD occlusion tends to show ST depression in II, III, and aVF in addition to V1-V3 elevation. A "Wellens' pattern" (biphasic or deeply inverted T waves in V2-V3 when pain-free) signals critical proximal LAD stenosis before complete occlusion.
2. Inferior MI
Culprit artery: Right Coronary Artery (RCA) in ~80% of cases; Left Circumflex (LCx) in the rest
ECG leads showing changes: II, III, aVF (inferior leads)
| Finding | Detail |
|---|---|
| ST elevation | II, III, aVF |
| ST elevation III > II | Strongly suggests RCA occlusion (90% sensitive) |
| Reciprocal ST depression | Lead aVL (most reliable - 150° from lead III), and possibly lead I |
| Pathological Q waves | Develop in II, III, aVF |
ECG - Inferior MI with reciprocal changes:
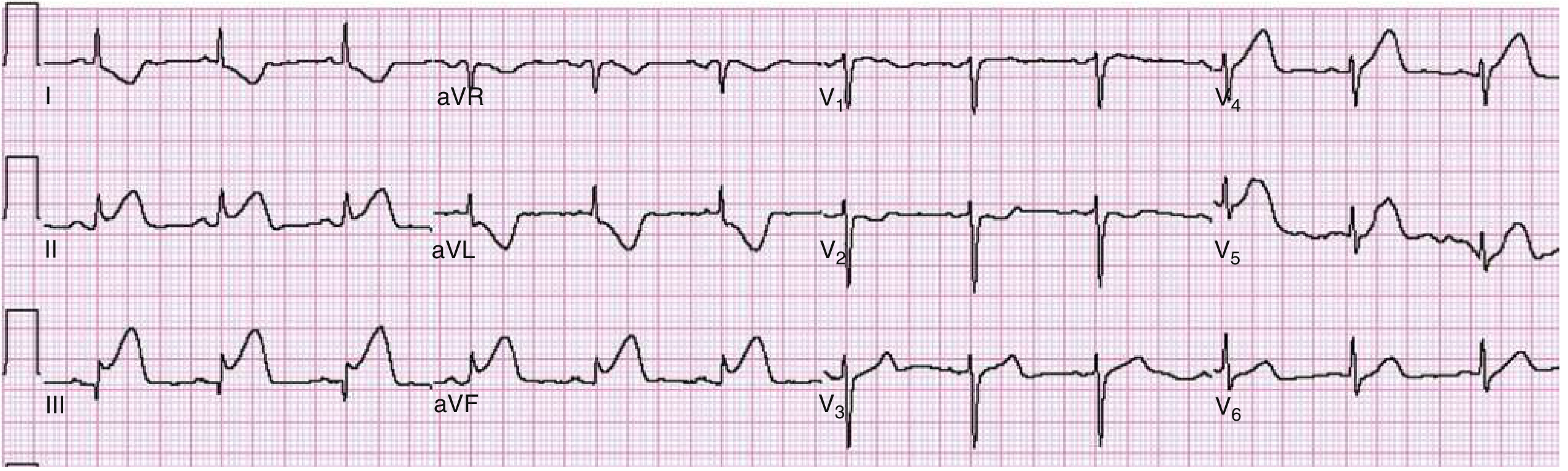
Marked ST elevation in II, III, and aVF with reciprocal depression most prominent in aVL. This is the classic inferior STEMI pattern. (Rosen's Emergency Medicine)
Key distinctions for inferior MI:
- ST elevation III > II + ST depression in I/aVL → RCA occlusion (~90% sensitive, ~71% specific)
- ST elevation II ≥ III + isoelectric or elevated aVL → LCx occlusion (often "electrocardiographically silent")
- ST elevation in V1 alongside inferior STEMI → suspect right ventricular (RV) infarction - get right-sided leads (V3R-V6R); STE in V4R is highly specific
- ST depression in V1-V3 with inferior MI → suspect posterior extension (see below)
Inferior MI is the type that most frequently shows reciprocal changes, and their presence correlates with larger infarct size and worse outcomes.
3. Posterior MI
Culprit artery: RCA (posterior descending branch) or LCx
Key concept: No standard 12-lead electrode directly overlies the posterior wall, so you see mirror-image (reciprocal) changes in the right precordial leads V1-V3.
| Standard 12-lead (V1-V3) - "mirror image" | What it actually represents |
|---|---|
| ST depression (horizontal) | Mirror of ST elevation posteriorly |
| Tall, broad R wave (>0.04 s) | Mirror of posterior Q wave |
| Upright T wave | Mirror of inverted T wave posteriorly |
| R/S ratio ≥ 1 in V1-V2 | Mirror of posterior Q wave dominance |
ECG - Posterior MI findings in V1 and V2:
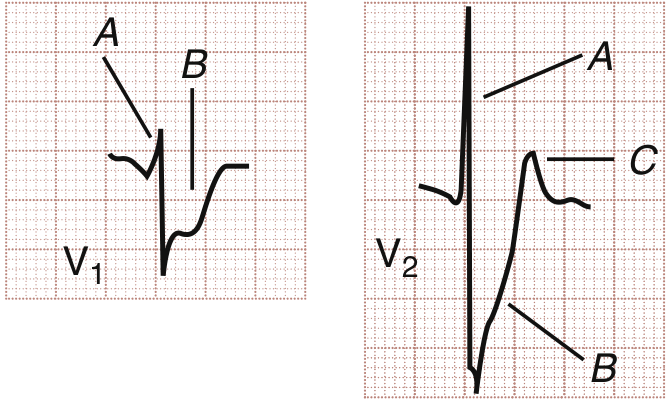
V1: horizontal ST depression (A) with prominent R wave (B). V2: tall R wave (A), deep S wave (B), upright T wave (C). These are the reciprocal "mirror image" of posterior ST elevation. (Rosen's Emergency Medicine)
Confirming with posterior leads: Place V7 (posterior axillary line), V8 (left scapular tip), V9 (left paraspinal) - these directly image the posterior wall and show ST elevation ≥ 0.5 mm, confirming posterior STEMI.
Clinical importance: Posterior MI accompanies inferior MI in ~15-20% of all AMIs. When found together (inferoposterior MI), the infarct is larger, ejection fraction is lower, and mortality is higher. Isolated posterior MI (~5% of AMIs) may be entirely missed on a standard 12-lead ECG without posterior leads.
Side-by-Side Comparison
| Feature | Anterior MI | Inferior MI | Posterior MI |
|---|---|---|---|
| Artery | LAD | RCA (>80%), LCx | RCA/LCx posterior branch |
| Primary leads | V1-V4 | II, III, aVF | No direct lead; V7-V9 if placed |
| ST elevation | V1-V4 (± I, aVL) | II, III, aVF | V7-V9 (posterior leads) |
| ST depression | May see in II, III, aVF | Best in aVL (reciprocal) | V1-V3 (reciprocal mirror) |
| Q waves | V1-V4 | II, III, aVF | None in standard leads |
| Tall R waves | None | None | V1-V2 (mirror of Q waves) |
| Upright T | V1-V4 (early) | II, III, aVF | V1-V2 (mirror pattern) |
| Special leads needed | None routinely | V4R (if RV infarct suspected) | V7-V9 posterior leads |
| Common complication | Heart block (proximal LAD), cardiogenic shock | RV infarction, heart block (AV node from RCA) | Underdiagnosis on standard 12-lead |
A Practical Memory Hook
- Anterior = "anterior wall burns" → ST elevation in anterior chest leads (V1-V4)
- Inferior = "floor of the heart burns" → ST elevation in inferior limb leads (II, III, aVF) with reciprocal depression in aVL
- Posterior = "back wall burns but we can only see the reflection" → ST depression + tall R + upright T in V1-V3 (the mirror image), confirmed by posterior leads
Sources: Tintinalli's Emergency Medicine (9e), Table 49-4, pp. 378-383; Rosen's Emergency Medicine (9e), pp. 1001-1006
This is a shared conversation. Sign in to Orris to start your own chat.