Pneumocephalus
Reading File
Finding Sources
Finding Sources
Searching PubMed
pneumocephalus
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive, well-sourced information. Let me compile the full answer.
Pneumocephalus
Pneumocephalus (also called aerocele or pneumocranium) is the presence of air or gas within the cranial cavity. It may be epidural, subdural, subarachnoid, intraventricular, or intraparenchymal in location.
Etiology and Causes
Air enters through any defect that breaches the skull and dura. Common causes include:
- Cranial surgery - ~66% of postcraniotomy CT scans show some degree of pneumocephalus - Schwartz's Principles of Surgery, p. 1537
- Head trauma with skull fracture - especially skull base fractures, fractures through paranasal sinuses or mastoid air cells
- Posterior fossa procedures in the sitting position - air enters the subarachnoid space "much as air enters an inverted pop bottle" as CSF is lost during surgery
- CSF leak / CSF rhinorrhea - pneumocephalus is pathognomonic for a CSF fistula, with an associated meningitis risk as high as 30% - Scott-Brown's Otolaryngology, p. 1681
- Skull base tumors or infections (rare)
- Lumbar drain or VP shunt - these lower ICP and create a vacuum that draws air inward, particularly if there is communication with the mastoid air cells
Mechanisms of Air Entry
Two major mechanisms are recognized - Schwartz's Surgery, p. 1548:
-
Ball-valve mechanism - air enters the intracranial cavity during periods of positive pressure (e.g., coughing, nose-blowing, positive-pressure ventilation). The skull defect acts as a one-way valve, allowing air in but not out.
-
Inverted-bottle (siphon) mechanism - air enters due to a negative pressure gradient created by CSF drainage. Occurs with traumatic or iatrogenic CSF leaks, lumbar drains, or EVDs. The analogy is fluid draining out of an inverted bottle, with air rushing in to replace it.
Classification
| Type | Features |
|---|---|
| Simple pneumocephalus | Air present but not under tension; usually self-limiting |
| Tension pneumocephalus | Air under pressure; mass effect; neurosurgical emergency |
Tension Pneumocephalus
This is the dangerous variant. Air becomes trapped within the cranial cavity and cannot equilibrate with atmospheric pressure, acting as an expanding mass lesion.
Pathophysiology: During posterior fossa or supratentorial surgery in a head-up position, hypocapnia + venous drainage + osmotic diuresis + CSF loss reduce intracranial volume. Air fills this space. Once the cranium is closed and the patient returns to near-supine, CSF and venous blood reaccumulate and the air pocket becomes unyielding (nitrogen diffuses very slowly) - Miller's Anesthesia, p. 8153.
Clinical features:
- Delayed awakening or failure to wake after neurosurgery
- Progressive headache, confusion, obtundation
- Deteriorating neurological exam consistent with raised ICP
- Potential herniation if untreated
CT Radiographic signs - Schwartz's Surgery, p. 1539:
- "Mount Fuji" sign - the bifrontal air pocket separates the frontal lobes and widens the interhemispheric fissure, mimicking the silhouette of Mt. Fuji
- "Air bubble" sign - multifocal pockets of air throughout the subarachnoid cisterns
Below is a CT demonstrating the Mount Fuji sign with bifrontal air separation and intraparenchymal air:
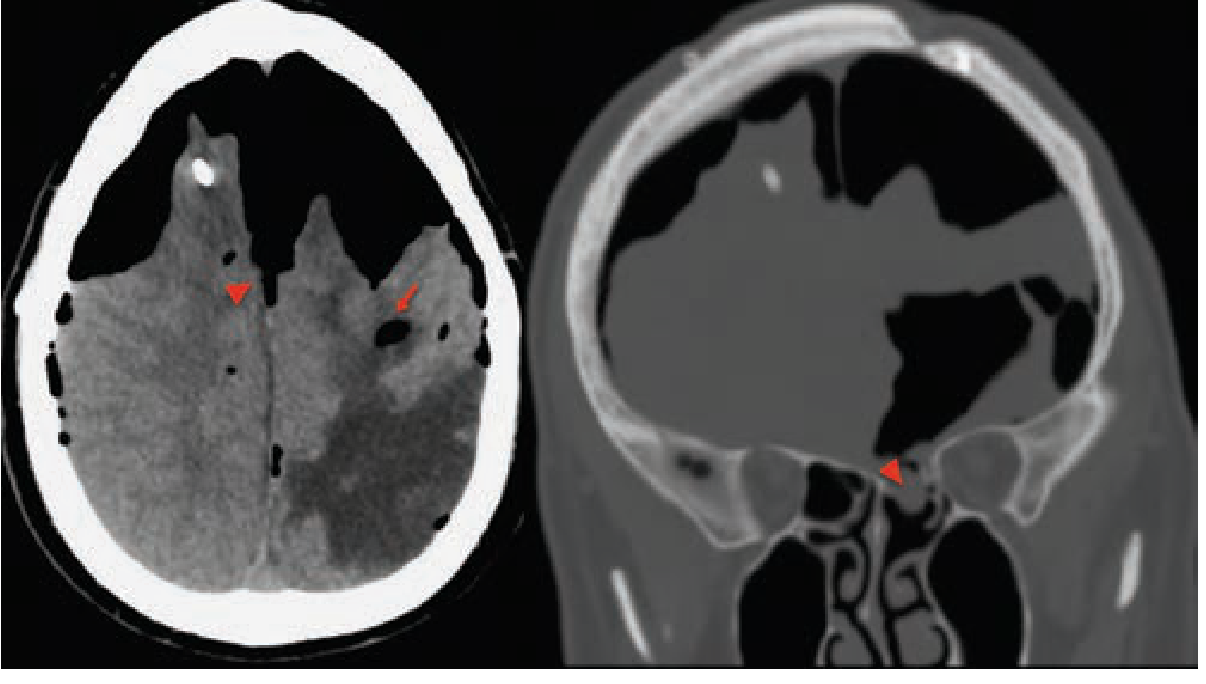
And a CT of postoperative tension pneumocranium with massive right frontal air causing right-to-left midline shift and compression of the right frontal lobe:

Diagnosis
- CT head - modality of choice; air appears as extremely low-density (darker than CSF) collections
- Brow-up lateral skull X-ray - can detect intracranial air as crescent-shaped lucency
- CSF rhinorrhea may coexist; confirm with beta-2-transferrin or tau protein testing, or CT cisternography with water-soluble contrast - Adams & Victor's Neurology, p. 894
Role of Nitrous Oxide (N₂O)
N₂O diffuses into any closed gas space and expands its volume. If a trapped intracranial air pocket exists after dural closure, N₂O can convert simple pneumocephalus into a life-threatening tension pneumocephalus. Key points:
- N₂O is not absolutely contraindicated before dural closure (the space is not yet sealed), and may actually speed resorption of residual gas pre-closure
- N₂O should be discontinued at or before dural/scalp closure when head-up posterior fossa surgery has been performed
- Tension pneumocephalus can also occur entirely without N₂O - Miller's Anesthesia, p. 8152
Management
Simple / Asymptomatic Pneumocephalus
- Observation; most resorb spontaneously within 7-10 days
- 100% supplemental oxygen - increases the nitrogen diffusion gradient between the intracranial air and the bloodstream, accelerating resorption - Schwartz's Surgery, p. 1548
- Avoid positive-pressure ventilation and nose-blowing (prevents worsening via ball-valve)
- Head-of-bed positioning depends on mechanism:
- Ball-valve: lay flat (minimizes upward air travel)
- Inverted-bottle/CSF leak at skull base: elevate HOB to reduce ventricular CSF pressure
Tension Pneumocephalus (Neurosurgical Emergency)
- Urgent neurosurgical consultation
- Twist-drill burr hole + needle puncture of the dura to release trapped air - Miller's Anesthesia, p. 8153
- Aspiration via craniotomy burr hole
- Surgical exploration to seal air leaks if necessary - Scott-Brown's Otolaryngology, p. 1689
- Search for associated CSF fistula (~one-third of cases have a concurrent CSF leak); repair may be performed electively or urgently
Special Circumstances
- Mastoid/eustachian tube communication (e.g., after posterior fossa surgery with VP shunt): occlusion of the eustachian tube and mastoid obliteration, potentially including transcochlear obliteration of petrous apex air cells - Shambaugh Surgery of the Ear, p. 5002
- CSF rhinorrhea persisting or complicated by meningitis: surgical dural repair, sometimes via endoscopic approach
Prognosis
- Small simple collections resolve without treatment
- Tension pneumocephalus carries a high mortality if unrecognized; prompt surgical decompression is life-saving
- Meningitis risk with pneumocephalus associated with open CSF fistula can be as high as 30%, warranting close monitoring
Recent evidence: A 2025 systematic review and meta-analysis (PMID 40344816) found that massive pneumocephalus is a significant risk factor for recurrence after chronic subdural hematoma surgery, reinforcing the importance of minimizing air entry during neurosurgical procedures.
Sources: Adams & Victor's Principles of Neurology 12e | Miller's Anesthesia 10e | Morgan & Mikhail's Clinical Anesthesiology 7e | Schwartz's Principles of Surgery 11e | Scott-Brown's Otorhinolaryngology Vol 2 | Shambaugh Surgery of the Ear
This is a shared conversation. Sign in to Orris to start your own chat.