Explain about the pleomorphic adenoma
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pleomorphic adenoma"[MeSH Terms] AND salivary gland
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the content needed to write a thorough, well-illustrated answer.
Pleomorphic Adenoma
Pleomorphic adenoma (also called benign mixed tumour or pleomorphic salivary adenoma / PSA) is the most common neoplasm of the salivary glands. It accounts for approximately 50% of all salivary gland tumours, ~65% of parotid tumours, and ~40% of intra-oral minor salivary gland tumours. Annual incidence is reported at 2.4-3.05 per 100,000 population.
Epidemiology & Sites
| Feature | Detail |
|---|---|
| Most common age | 3rd-6th decade (average ~45 years) |
| Sex predilection | Slightly more common in women |
| Most common site | Parotid gland (>80%), usually the superficial lobe |
| Other sites | Submandibular gland, minor salivary glands (hard palate most common intraorally), buccal mucosa, lip |
| Risk factor | Radiation exposure increases risk |
- Bailey and Love's Short Practice of Surgery, 28th Ed.
Deep lobe parotid tumours may present as a paratonsillar bulge (dumbbell tumour). Tumours arising from accessory parotid tissue along Stensen's duct may only become visible on opening the mouth.
Clinical Presentation
- Painless, slow-growing, mobile, well-defined solitary mass
- Gradual progression over many years - can grow to enormous proportions if untreated
- Firm to soft consistency depending on the stromal component - chondroid/collagenous tumours feel hard; myxoid ones feel almost fluctuant
- No facial nerve involvement (involvement suggests malignancy)
- Red flags for malignant transformation: sudden increase in size, facial nerve palsy, fixation to surrounding structures, pain
Pathogenesis / Molecular Biology
- Thought to be derived from intercalated duct cells and myoepithelial cells that differentiate into both epithelial and connective tissue elements - hence "mixed tumour"
- PLAG1 overexpression (via chromosomal rearrangements) promotes cell growth through growth factor receptor signalling pathways - found in many cases
- HMGA2 gene mutations (encoding a DNA-binding protein) account for most remaining cases lacking PLAG1 overexpression
- All tumour elements - including the apparent mesenchymal components - are believed to be of myoepithelial or ductal reserve (stem) cell origin
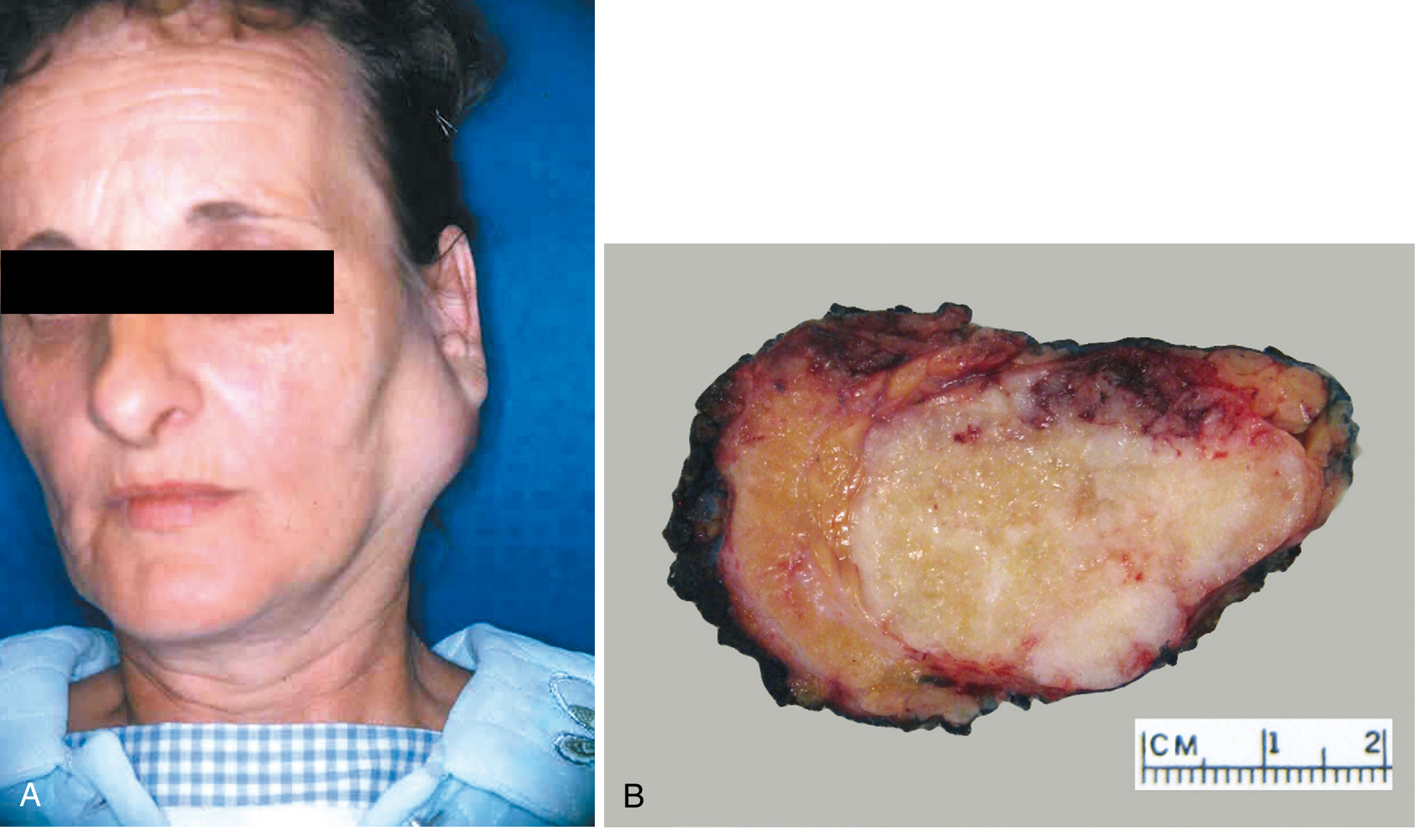
Macroscopic Appearance

- Rounded/ovoid, well-demarcated mass, rarely exceeds 6 cm
- Bosselated (nodular) surface
- Cut surface is gray-white with myxoid and blue chondroid (cartilage-like) areas
- May show cystic change, calcification, or bone
- Capsule: variably present; in virtually all PSAs the capsule is <20 microns thick in at least one area, and is incomplete in ~50% - especially the myxoid type
- Protuberant peri-capsular nodules may be attached by slender pedicles - these are easily left behind if the tumour is merely enucleated, forming foci for recurrence
Microscopic / Histological Appearance
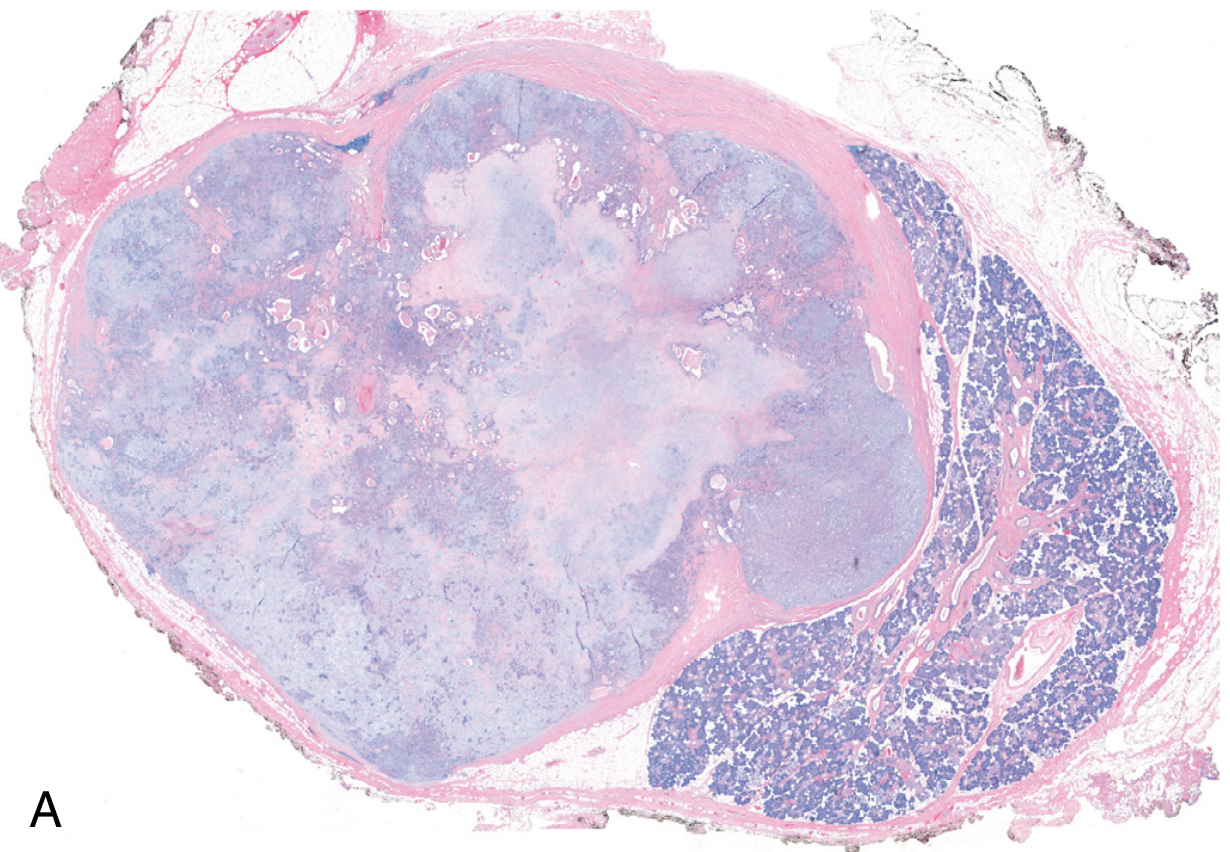
The hallmark is morphologic heterogeneity (not true nuclear pleomorphism - the name refers to the varied tissue types):
Three basic components:
- Ductal (epithelial) elements - cuboidal to columnar cells lining duct-like structures; express CK7 (strong and diffuse)
- Myoepithelial cells - oval, plasmacytoid, spindle, or clear morphology; express p63, S-100, SOX10, SMA
- Chondromyxoid stroma - loose myxoid and hyaline tissue, islands of cartilage, occasionally bone
Additional features:
- Squamous metaplasia with keratinization - common; does not imply malignancy
- Metaplastic changes: lipomatous, osseous, neuroid, angiomatoid
- Degenerative changes: cystic change, infarction, mineralization, hyalinization, elastosis
- No significant epithelial dysplasia or mitotic activity in benign lesions
- Ductal atypia, diffuse fibrosis, and necrosis should raise suspicion for malignant transformation
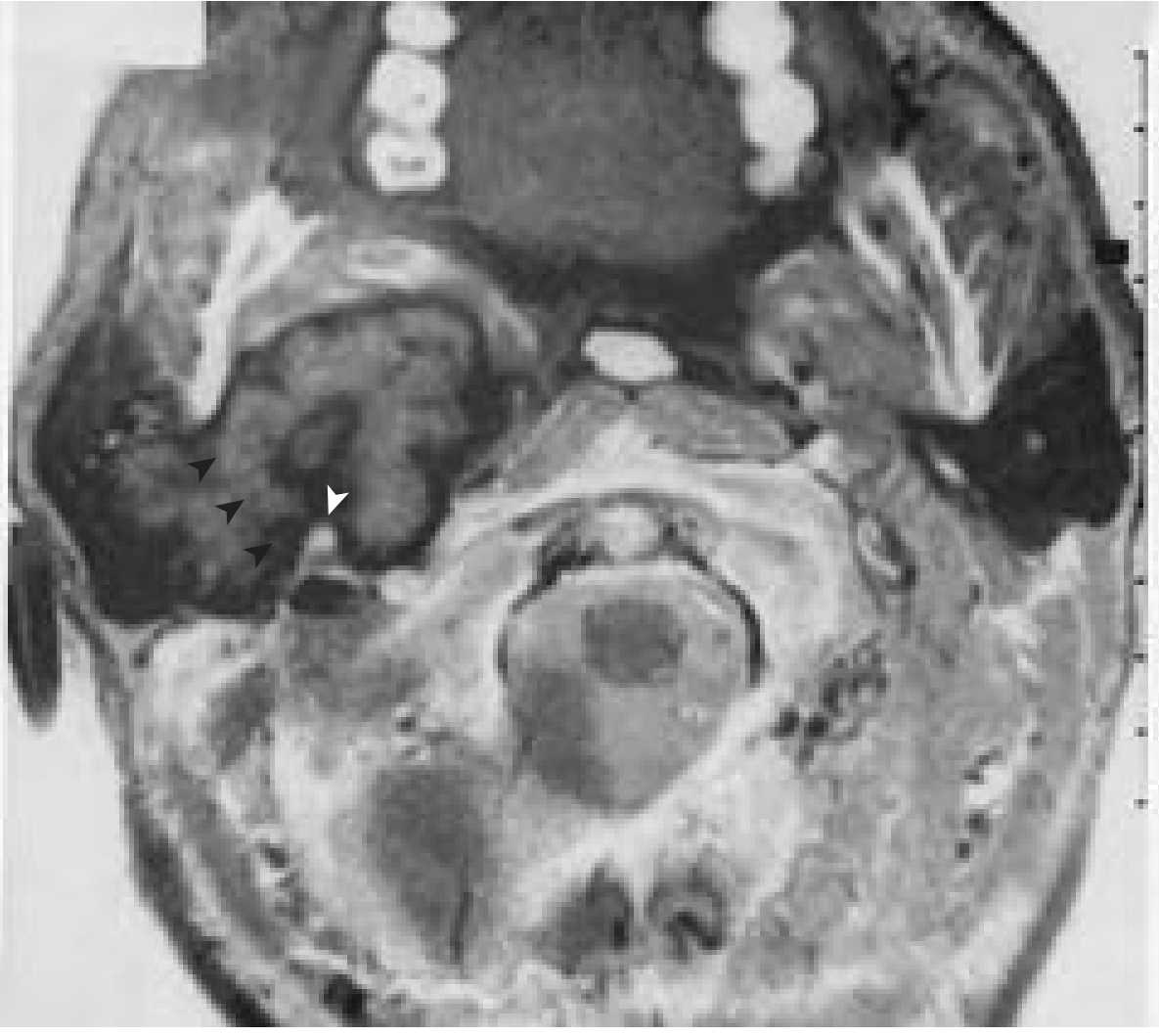
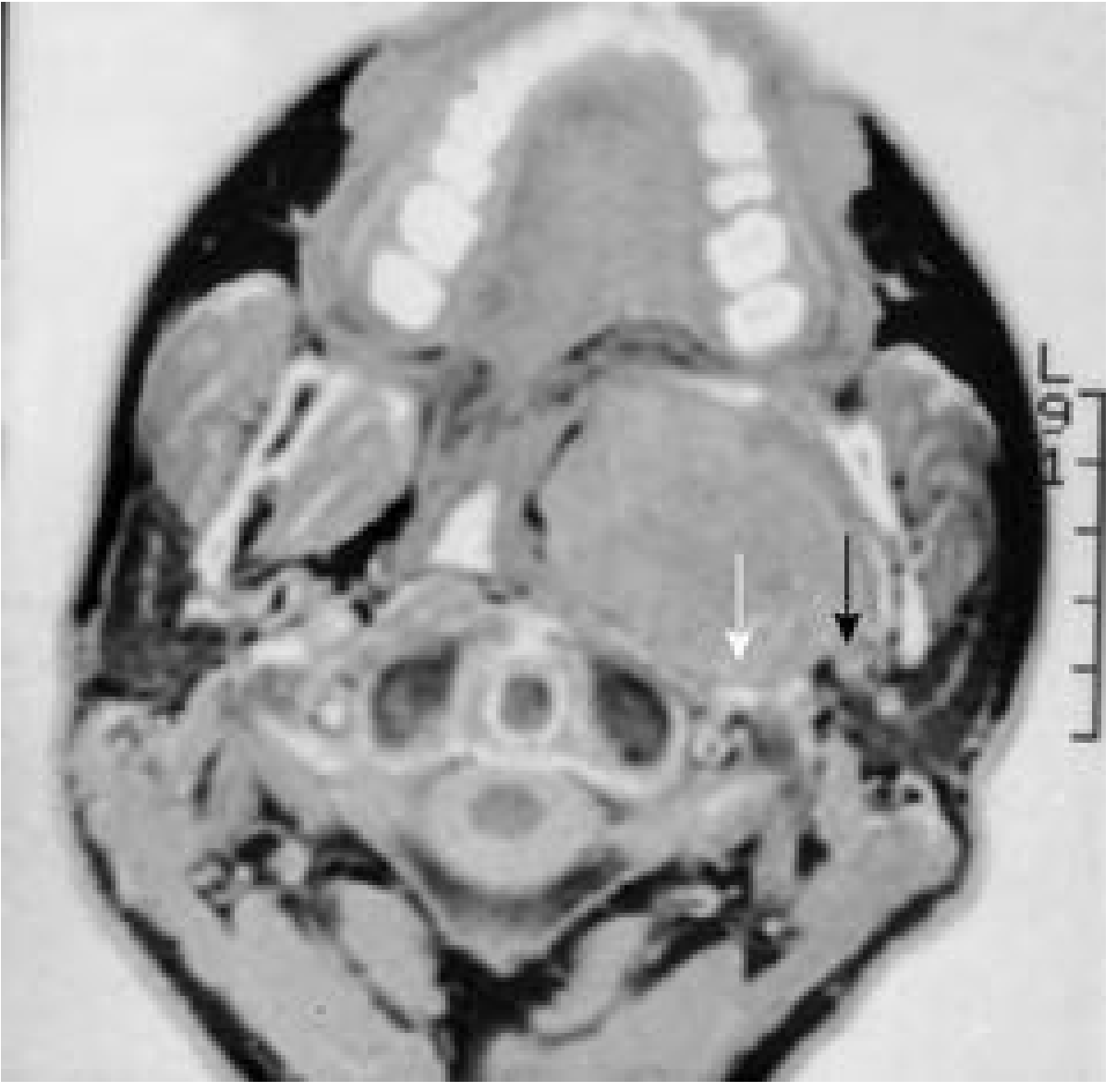
Imaging
- CT/MRI: well-demarcated, homogeneous or heterogeneous mass in the parotid or other salivary gland
- Calcifications or bone formation on imaging strongly suggest pleomorphic adenoma (no other salivary gland tumour is likely to develop these)
- Deep lobe tumours extend into the parapharyngeal space - "dumbbell" appearance on CT/MRI
Behaviour & Complications
Recurrence
- Simple enucleation carries a recurrence rate approaching 25% due to capsule incompleteness and peri-capsular nodule spillage
- Recurrences after adequate parotidectomy occur in only ~4%
- Recurrence is typically multifocal (seeding pattern), particularly if myxoid capsular rupture occurs intra-operatively
Malignant Transformation - Carcinoma ex Pleomorphic Adenoma
This is the most feared complication. Risk increases with duration of the lesion:
- Present <5 years: ~2% risk of harbouring malignancy
- Present >15 years: ~10% risk
- Overall figure historically cited: ~6% risk of malignant change (some sources cite 1-5% over 10 years)
- Risk factors for transformation: older age, male sex, long tumour duration, multiple recurrences, deep lobe location
When carcinoma ex pleomorphic adenoma develops, cancers are usually adenocarcinomas or undifferentiated carcinomas - highly aggressive with mortality rates of 30-50% at 5 years.
Diagnosis
- Fine Needle Aspiration Biopsy (FNAB): first-line investigation; shows characteristic mixed epithelial and myoepithelial cells in chondromyxoid background
- Note: the tumour's histological heterogeneity can occasionally make diagnosis from limited FNAB samples difficult
- Imaging (CT / MRI / Ultrasound): delineates extent and relationship to facial nerve; identifies deep lobe involvement
- Core biopsy: occasionally required
Treatment
General Principles
Surgery is advised for virtually all patients because:
- It provides definitive histological diagnosis
- Tumours continue to grow if left untreated
- There is a risk of malignant transformation
Parotid Pleomorphic Adenoma
- Superficial lobe: superficial parotidectomy with facial nerve preservation
- Deep lobe / total parotid: total conservative parotidectomy
- Simple enucleation is contraindicated - risk of capsular rupture, tumour spillage, and multifocal recurrence
- A cuff of surrounding normal tissue should be included wherever possible to account for pseudopods extending beyond the capsule
Submandibular Gland
- Excision of the entire submandibular gland (extra-capsular dissection)
Minor Salivary Glands (Oral Cavity)
- Transoral complete surgical excision; recurrences are rare given the encapsulated nature
- CO₂ laser may be used as a cutting tool
Summary Table
| Feature | Detail |
|---|---|
| Type | Benign mixed tumour |
| Most common site | Parotid (superficial lobe) |
| Clinical | Painless, mobile, slow-growing mass |
| Gross | Bosselated, chondromyxoid cut surface |
| Histology | Ductal cells + myoepithelial cells + chondromyxoid stroma |
| Key markers | CK7 (luminal), p63/S-100/SOX10/SMA (myoepithelial) |
| Recurrence (enucleation) | ~25% |
| Recurrence (parotidectomy) | ~4% |
| Malignant transformation | ~2-10% depending on duration |
| Treatment | Surgical excision with cuff of normal tissue |
Sources:
- Robbins & Kumar Pathologic Basis of Disease (Robbins Cotran, p. 697)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Chapter 26, Chapter 9)
- Bailey and Love's Short Practice of Surgery, 28th Ed. (Chapter 54)
- Cummings Otolaryngology Head and Neck Surgery (Chapter 90)
so is the clinical presentation different in the tumor that arises from tail of parotid and deep lobe of parotid
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Excellent - I have all the content and imaging needed. Here is the detailed comparison:
Clinical Presentation: Tail of Parotid vs. Deep Lobe Pleomorphic Adenoma
The short answer is yes - the presentations are strikingly different, primarily because of the anatomy. The stylomandibular ligament acts as the critical dividing structure.
Anatomy First - Why It Matters
The parotid gland wraps around the mandibular ramus and is divided by the facial nerve into a superficial lobe and a deep lobe. The deep lobe projects medially through the stylomandibular tunnel (bounded by the stylomandibular ligament) into the prestyloid parapharyngeal space. The tail is the most inferoposterior extension of the superficial lobe, lying between the ramus of the mandible and the sternocleidomastoid muscle, overlying the digastric.
Tail of Parotid Tumour
Presentation
- Presents as a visible and palpable lump in the upper neck, just below and anterior to the ear lobe
- Often mistaken for a cervical lymph node (level II adenopathy) or a submandibular gland tumour - this is a common diagnostic trap
- The swelling is in the superficial/subcutaneous plane; ultrasound is very helpful in distinguishing a tail of parotid mass from an adjacent lymph node
- Slow-growing, painless, mobile - the classic presentation
- No oropharyngeal symptoms - no dysphagia, no change in voice, no snoring
- No facial nerve involvement unless there is malignant transformation
Key Point
About 85% of all parotid pleomorphic adenomas are in the parotid, and most of these present in the tail of the parotid - so this is the most common clinical scenario you will encounter. - KJ Lee's Essential Otolaryngology
Surgery
The tail is the ideal location for extracapsular dissection (ECD) - a more limited procedure that avoids formal facial nerve dissection, suitable for mobile lesions in expert hands.
Deep Lobe Tumour
Presentation
This is where things become distinctly different. About 10-12% of pleomorphic adenomas originate entirely from the deep lobe.
-
Externally, the neck may look normal or show only a subtle parotid swelling - because the mass is hidden medial to the mandibular ramus, it is not easily visible or palpable from the outside
-
The tumour grows medially into the parapharyngeal space, so the classic presentation is:A paratonsillar bulge - the patient (or their dentist) notices a smooth swelling of the lateral oropharyngeal wall, pushing the tonsil and soft palate medially. The patient may complain of:
- A feeling of fullness in the throat
- Snoring or obstructive sleep apnoea-like symptoms
- Muffled voice (hot-potato voice) in large tumours
- Dysphagia in large tumours
-
There is no external neck mass until the tumour is very large
-
The facial nerve is at greater risk during surgery for deep lobe tumours
The Dumbbell Tumour (Mixed Superficial + Deep)
A subset of tumours starts in the superficial lobe and extends through the stylomandibular tunnel into the deep lobe. The tunnel constricts the tumour's isthmus, giving it a dumbbell shape on imaging.
Comparison Table
| Feature | Tail of Parotid | Deep Lobe / Parapharyngeal |
|---|---|---|
| External swelling | Yes - visible neck lump | Absent or minimal |
| Intraoral presentation | None | Paratonsillar bulge / lateral pharyngeal wall fullness |
| Throat symptoms | None | Dysphagia, snoring, muffled voice (large tumours) |
| Common clinical mistake | Mistaken for cervical lymph node or submandibular lump | Missed on routine examination; may be found incidentally |
| Palpability | Easily felt | Bimanual palpation (intraoral + neck) needed |
| Imaging needed | Ultrasound usually sufficient | CT + MRI both required to plan surgery |
| Imaging appearance | Superficial, well-defined mass | Prestyloid parapharyngeal mass; displaces carotid posteriorly |
| Dumbbell sign | No | Yes (if it extends from superficial through stylomandibular tunnel) |
| Surgical approach | Extracapsular dissection / superficial parotidectomy | Transparotid + transcervical approach; transoral only if truly ectopic |
| Facial nerve risk | Lower | Higher - the facial nerve must be traced into the deep lobe |
One Practical Point on Imaging
On imaging, all parapharyngeal pleomorphic adenomas - whether from the deep lobe or from ectopic salivary tissue - occupy the prestyloid compartment and displace the carotid artery posteriorly. This distinguishes them from poststyloid tumours (e.g., glomus tumours, schwannomas) which push the carotid anteriorly. Pre-operative CT and MRI are both necessary to:
- Determine whether the tumour is connected to the deep lobe (affects surgical approach)
- Assess capsule thickness (myxoid tumours are fragile and prone to rupture)
- Define the relationship to the facial nerve and great vessels
- Cummings Otolaryngology Head and Neck Surgery
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery
- KJ Lee's Essential Otolaryngology
Explain about Ranula
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I have all the material needed. Here is the comprehensive answer:
Ranula
Etymology & Definition
The word ranula comes from the Latin rana meaning "little frog." The name was coined because the swelling in the floor of the mouth resembles the belly of a frog, and large ranulas cause a characteristic croaking quality of speech. It was first described by Banister in his surgical compilation of 1585.
A ranula is a fluid-filled cystic lesion arising from the floor of the mouth due to extravasation or obstruction involving the sublingual salivary gland or its ducts. It is classified as an extravasation pseudocyst - it lacks a true epithelial lining and is instead contained by loose connective tissue/granulation tissue (unlike a true retention cyst).
Prevalence: approximately 0.2 cases per 1000 people.
Types
There are two main types based on anatomical extent:
| Simple (Intraoral) Ranula | Plunging (Deep/Cervical) Ranula | |
|---|---|---|
| Location | Confined above the mylohyoid muscle, floor of mouth | Extends below the mylohyoid into the submandibular/submental space of the neck |
| Mechanism | Duct obstruction or acinar rupture → localised mucocele | Rupture + herniation through a defect (boutonniere anomaly) in the mylohyoid muscle |
| Presentation | Intraoral bluish swelling | Neck swelling ± intraoral component |
| Lining | Pseudocyst (no true epithelium) | Pseudocyst (effectively a mucocele) |
Aetiology
- More commonly acquired than congenital
- Caused by:
- Obstruction of the sublingual gland or its many small ducts (spontaneous or from periductal scarring)
- Trauma to the sublingual gland ducts - e.g., following floor-of-mouth procedures, dental procedures
- Rupture of the main duct or of obstructed acini of the sublingual gland
- May be congenital (a developmental defect in the mylohyoid allows natural herniation)
- Increased occurrence noted in HIV-infected individuals - due to blockage from inflammation and periductal fibrosis as part of HIV-associated salivary gland disease
- A congenital predisposition has been suggested based on higher rates in certain ethnic groups and among siblings
Clinical Presentation
Simple Ranula
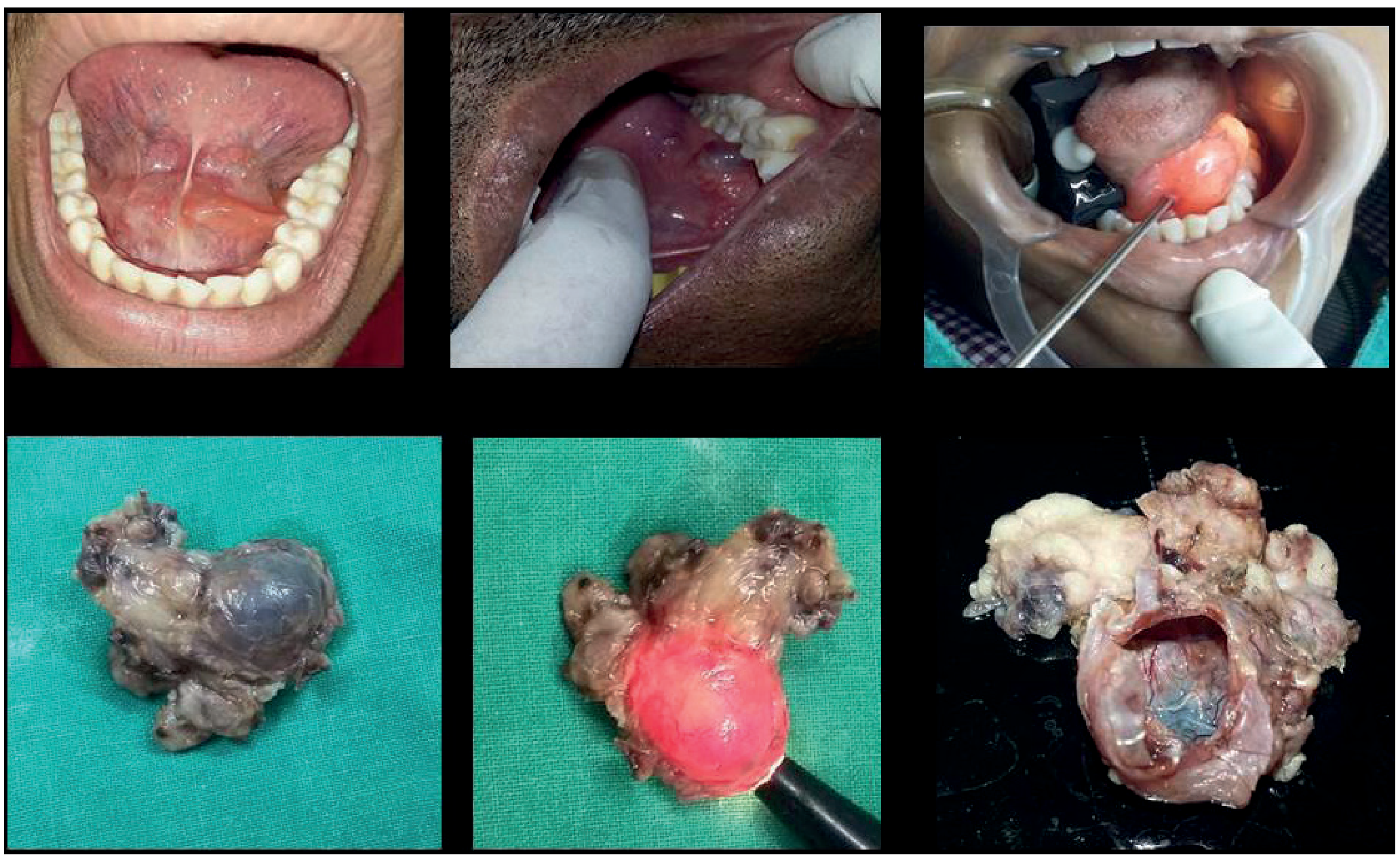
- Smooth, soft, fluctuant, painless swelling in the floor of the mouth
- Located on one side of the frenulum linguae - almost always unilateral
- Characteristic bluish translucent appearance (due to thin mucosa and fluid content)
- The submandibular (Wharton's) duct can sometimes be seen traversing the dome of the swelling
- Usually detected in the second decade of life; slight female predisposition
- A very large ranula may fill the entire floor of the mouth
- If large enough: elevation of the tongue causing difficulty with:
- Swallowing (dysphagia)
- Speech (croaking/muffled voice)
- Mastication
- Breathing (rarely - respiratory obstruction is rare but reported)
- Painless unless infected (when it becomes red, tender, and indurated)
- Aspiration yields thick, sticky, viscous saliva - this distinguishes it from a lymphangioma (which yields clear lymph fluid) and is both diagnostic and confirmatory
Plunging Ranula
- Usually presents as a painless, persistent, or slowly enlarging swelling in the submandibular/submental triangle of the neck
- There may be no visible intraoral component - the neck swelling is the presenting complaint
- Rarely may spread to the upper chest wall
- On bimanual palpation (one finger intraoral, one hand on neck): cross-fluctuation is demonstrable between the floor of mouth and the neck extension - a key clinical sign
- The mylohyoid defect through which it herniates is called the boutonniere anomaly
Investigations
Simple Ranula
- Imaging is not necessary to confirm the diagnosis - it is clinical
- However, imaging is required if:
- Previous surgery has been performed
- There is a cervical component
- The diagnosis is clinically uncertain
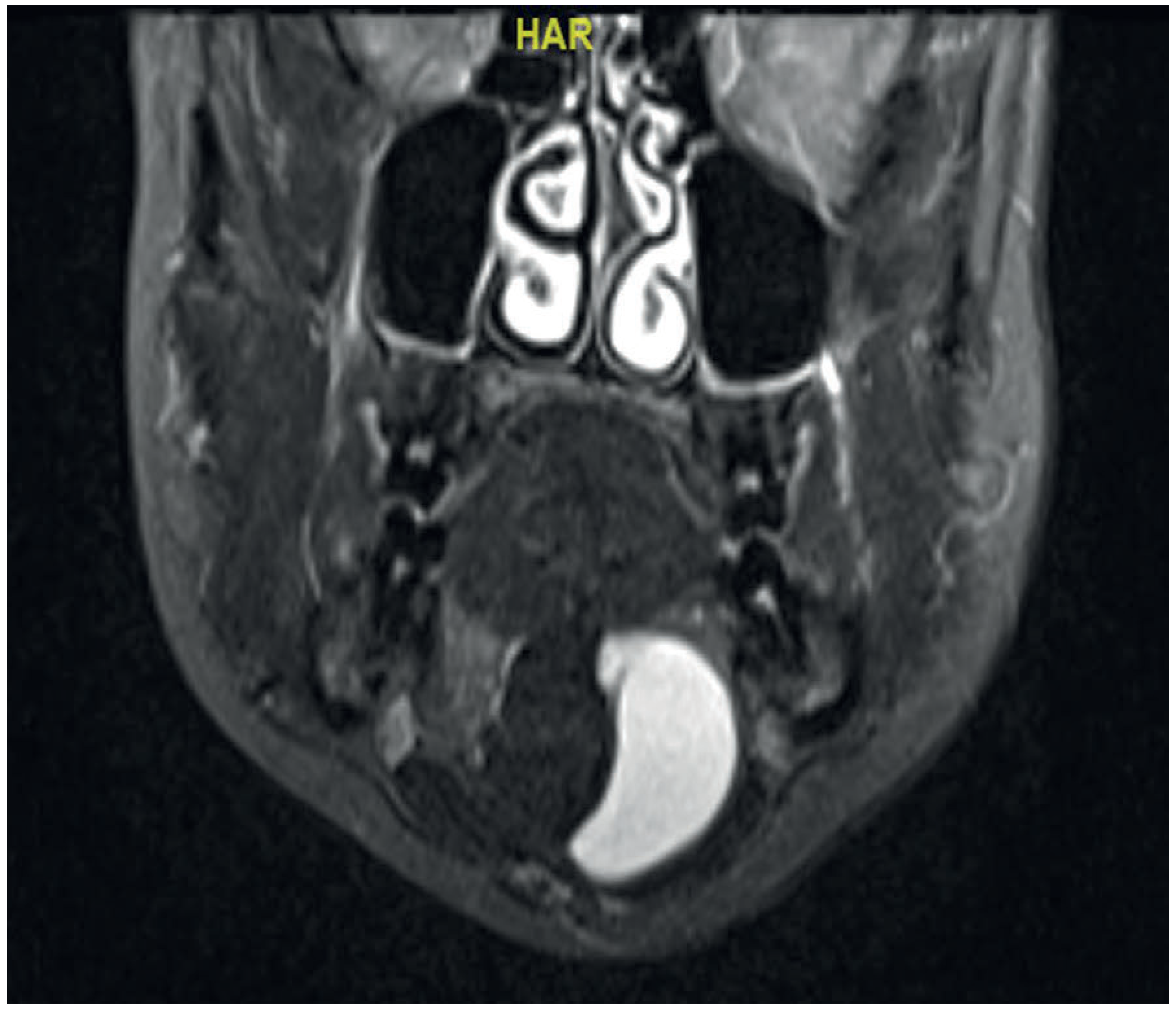
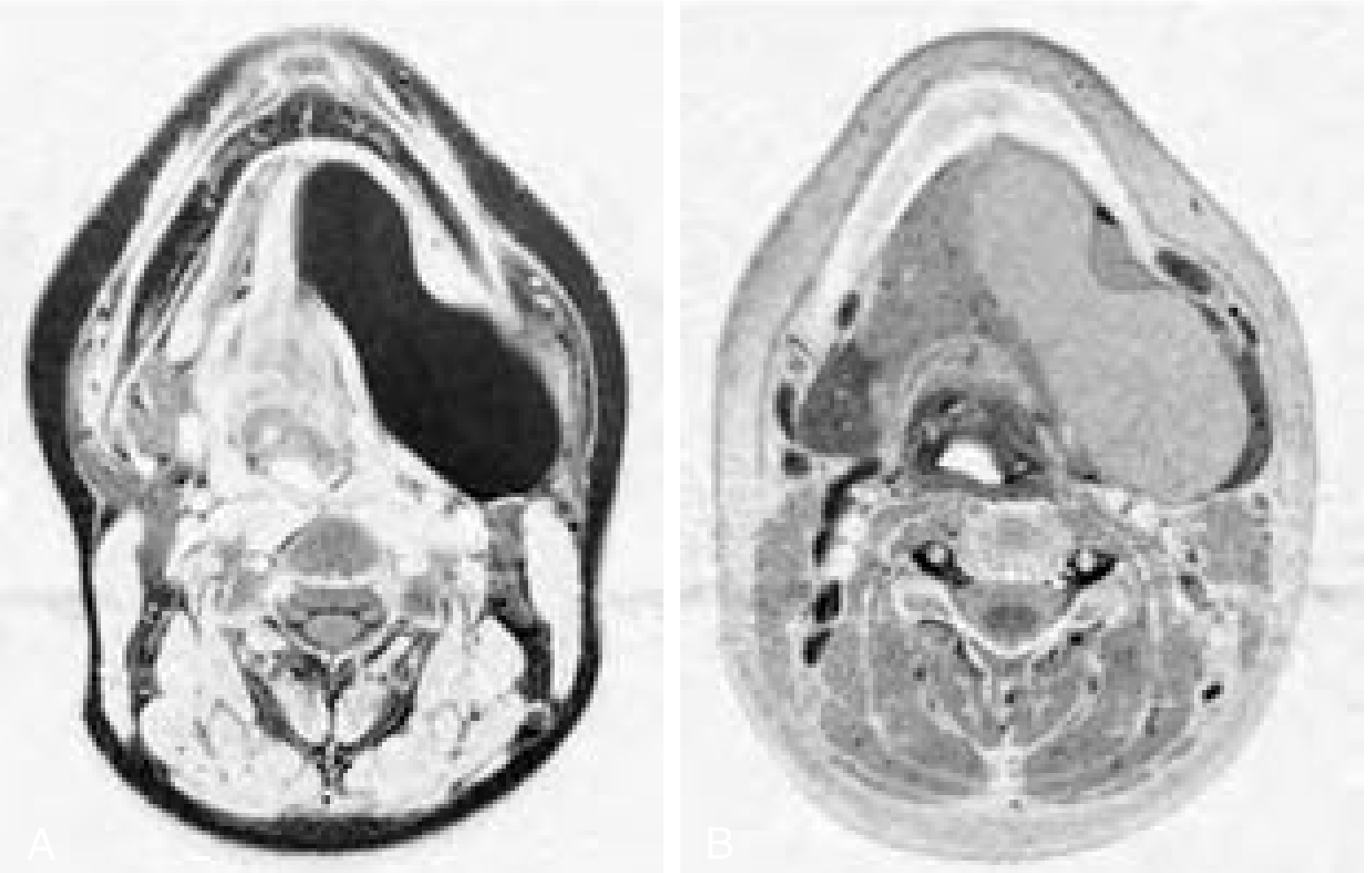
Plunging Ranula / Uncertain Cases
- MRI is preferred - it best defines soft tissue planes and extent
- CT: simple ranula appears as a solitary, low-attenuation, non-enhancing thin-walled mass; plunging ranulas may show some peripheral enhancement (granulation tissue)
- Ultrasound: unilocular, well-defined cystic mass; may contain fine internal echoes from debris (prior inflammation)
- On MRI: low T1 signal, high T2 signal, no contrast enhancement of the cyst wall
Differential Diagnosis
| Condition | How to distinguish |
|---|---|
| Lymphatic malformation | Also transilluminates; contains clear lymph on aspiration (not viscous saliva); has true epithelial lining on histology |
| Sublingual dermoid cyst | Opaque, non-translucent; contains sebaceous material; doughy consistency; midline location more common |
| Retention cyst (mucocele) | Has true epithelial lining; usually from minor salivary glands |
| Submandibular lymph node | Firm, not translucent; no connection to floor of mouth |
| Thyroglossal cyst | Midline, moves on swallowing and tongue protrusion |
| Branchial cyst | Upper neck, lateral position |
Key histological distinction from lymphatic malformation: a ranula is contained by loose connective tissue (pseudocyst), whereas a lymphatic malformation has a simple epithelial lining.
Treatment
Why Simple Aspiration/Drainage Fails
Simple aspiration or incision and drainage leads to a very high recurrence rate because the sublingual gland continues to leak saliva. Marsupialization of a plunging ranula has a recurrence rate of ~80% and is therefore inadequate.
Definitive Treatment: Sublingual Gland Excision
- The definitive treatment for both simple and plunging ranulas is excision of the cyst together with the sublingual gland
- The sublingual gland has multiple small ducts - if the gland is left behind, these continue leaking and the ranula recurs
- Complete sublingual gland excision: recurrence rate as low as 3.6%
- Ranula excision alone (without gland removal): significantly higher recurrence
Surgical Approaches
- Transoral approach: for intraoral (simple) ranulas and for plunging ranulas with a predominantly intraoral component
- External transcervical approach: for plunging ranulas that present predominantly submentally or in the neck
- Combined transoral + transcervical: for large dumbbell-type plunging ranulas
- Important: during any floor-of-mouth dissection, the lingual nerve and Wharton's duct must be identified and preserved - injury risks obstructive sialadenitis and sensory loss
Alternative/Adjunct Treatments
- OK-432 (picibanil) injection: a sclerotherapeutic agent derived from Streptococcus; induces inflammation and fibrosis leading to cyst obliteration; effective especially in paediatric patients though experience is more limited in this group
- Botulinum toxin injection: reported good results but needs further evaluation
- CO₂ or diode laser excision: reported for intraoral ranulas with low recurrence rates
- Oral nickel gluconate: a medical treatment described by Garofalo et al. - nickel at low doses promotes enzymatic tissue-repair in salivary glands; promising early results reported
Summary
| Feature | Detail |
|---|---|
| Origin | Sublingual salivary gland |
| Nature | Extravasation pseudocyst (no epithelial lining) |
| Age | 2nd decade most common; may be congenital |
| Appearance | Bluish, translucent, fluctuant, floor of mouth |
| Aspiration yield | Thick, viscous, sticky saliva |
| Simple ranula | Above mylohyoid; intraoral |
| Plunging ranula | Below mylohyoid; neck swelling |
| Key imaging | MRI - T2 hyperintense, no enhancement |
| Treatment of choice | Sublingual gland excision ± cyst (recurrence 3.6%) |
| Avoid | Simple aspiration, marsupialization (high recurrence) |
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Chapter 9 / Chapter 37)
- Bailey and Love's Short Practice of Surgery, 28th Ed. (Chapter 54)
- Cummings Otolaryngology Head and Neck Surgery (Chapter 82)
- S. Das - A Manual on Clinical Surgery, 13th Ed.
- KJ Lee's Essential Otolaryngology
This is a shared conversation. Sign in to Orris to start your own chat.