Thyroxine sysnthesis and metabolism.
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have all the content needed for a comprehensive answer. Here is the full, well-structured response:
Thyroxine (T4) - Synthesis and Metabolism
1. Regulation of Thyroid Hormone Production (HPT Axis)
The hypothalamic-pituitary-thyroid (HPT) axis forms a classic negative feedback loop:
- Hypothalamus releases TRH (thyrotropin-releasing hormone)
- TRH stimulates the anterior pituitary to secrete TSH (thyroid-stimulating hormone, a 31-kDa glycoprotein with α and β subunits)
- TSH binds its receptor (TSH-R, a 7-transmembrane GPCR) on follicular cells, activating adenylyl cyclase → ↑cAMP, driving hormone synthesis and secretion
- High circulating T4/T3 feeds back to suppress TRH and TSH, primarily via thyroid hormone receptor TRβ2
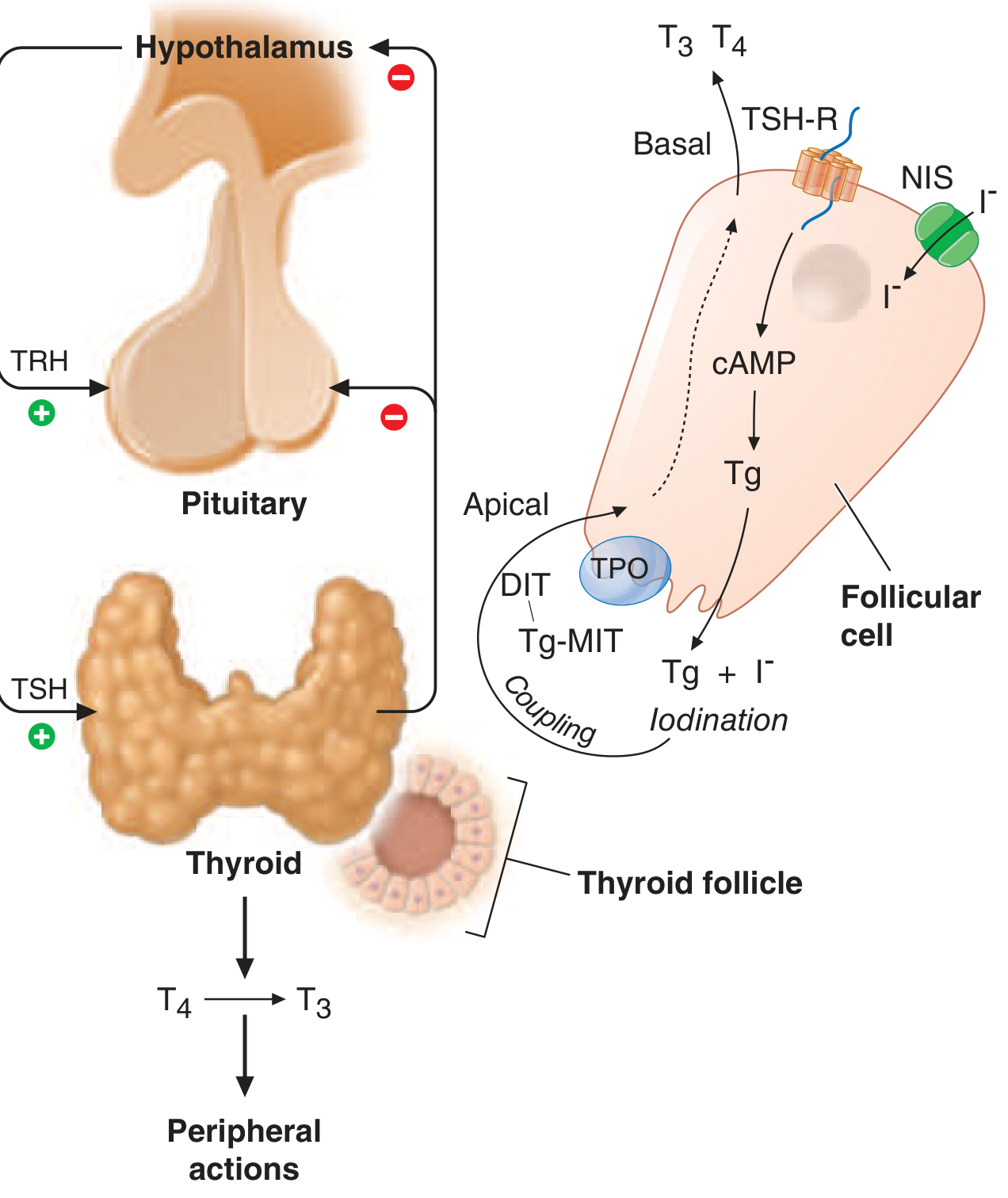
FIGURE 394-2 from Harrison's: Left - HPT axis feedback. Right - Intrafollicular biosynthesis steps (NIS, Tg, TPO, iodination, coupling).
2. Thyroid Hormone Synthesis - Step by Step
All steps take place within the thyroid follicle, centered on thyroglobulin (Tg), a large iodinated glycoprotein of 3,022 amino acid residues.
Step 1 - Iodide Uptake (Trapping)
- Dietary iodine (minimum ~100 µg/day for adults) is absorbed and circulates as iodide (I-)
- Iodide is actively transported from blood into the follicular cell across the basolateral membrane by the sodium-iodide symporter (NIS) - an energy-dependent co-transporter driven by the Na+/K+ ATPase gradient
- The intracellular iodide concentration is many times higher than serum
- NIS is also expressed (at low levels) in salivary glands, lactating breast, and placenta; this selective expression is exploited for radioiodine scanning and therapy
- Iodide then moves toward the apical border and exits into the colloid via pendrin (an apical iodide transporter; pendrin mutation causes Pendred syndrome - goiter + sensorineural deafness)
Step 2 - Oxidation of Iodide
- In the colloid, iodide (I-) is oxidized to I₂ (reactive iodine) by thyroid peroxidase (TPO) using H₂O₂ as the oxidant
- H₂O₂ is generated by NADPH oxidases (DUOX1/DUOX2) at the apical membrane
Step 3 - Organification (Iodination of Thyroglobulin)
- TPO catalyzes the iodination of tyrosine residues on Tg within the colloid
- A single iodine on tyrosine → monoiodotyrosine (MIT)
- Two iodines on tyrosine → diiodotyrosine (DIT)
- This entire process is called organification of iodine
Step 4 - Coupling Reaction
- TPO also catalyzes the coupling of iodotyrosyl residues still on the Tg backbone:
- DIT + DIT → T4 (tetraiodothyronine / thyroxine) - contains 4 iodine atoms
- DIT + MIT → T3 (triiodothyronine) - contains 3 iodine atoms
- The coupling forms an ether linkage between the residues
- The thyroid secretes T4 in ~15-fold excess over T3
Step 5 - Reuptake and Proteolysis
- When stimulated by TSH, follicular cells endocytose Tg from the colloid
- Lysosomal proteases cleave Tg, releasing free T4, T3, MIT, and DIT
- MIT and DIT are deiodinated within the cell by iodotyrosine deiodinase (DEHAL1), recycling iodine
- Free T4 and T3 are secreted into the bloodstream
Key enzymes: NIS (iodide uptake), TPO (oxidation, organification, coupling), DUOX2 (H₂O₂ generation), pendrin (apical iodide efflux)
Wolff-Chaikoff effect: Excess iodide transiently inhibits organification. The normal thyroid "escapes" this effect; autoimmune glands may not escape, leading to hypothyroidism with iodide loading.
3. Transport in Blood
Once in the bloodstream, thyroid hormones bind tightly to plasma proteins, limiting free diffusion:
| Binding Protein | Affinity | T4 carried | T3 carried |
|---|---|---|---|
| Thyroxine-binding globulin (TBG) | Highest | ~80% | ~80% |
| Transthyretin (TTR / prealbumin) | Intermediate | ~10% | Little |
| Albumin | Lowest | ~10% | ~30% |
- ~99.98% of T4 and ~99.7% of T3 are protein-bound
- Only the free (unbound) fractions are biologically active
- T4 serum half-life: 7 days | T3 serum half-life: 2 days
- Total T4: ~8 µg/dL | Total T3: ~0.14 µg/dL
TBG levels rise with estrogen (pregnancy, OCPs), increasing total T4/T3 without changing free hormone levels. Salicylates can displace thyroid hormones from binding proteins, transiently raising free levels.
4. Peripheral Metabolism - Deiodination
T4 is largely a prohormone; the more potent T3 is generated peripherally by deiodination.
Three Deiodinase Enzymes
| Enzyme | Location | Action |
|---|---|---|
| Type I (D1) | Liver, kidney, thyroid | Outer-ring deiodination: T4 → T3 (low affinity); also inactivates rT3 |
| Type II (D2) | Pituitary, brain, brown fat, thyroid | Outer-ring deiodination: T4 → T3 (high affinity); locally regulates T3; upregulated in hypothyroidism |
| Type III (D3) | Placenta, fetal tissues; activated in sick euthyroid syndrome (muscle, liver) | Inner-ring deiodination: T4 → reverse T3 (rT3) (inactive); T3 → 3,3'-T2 (inactive) |
- ~80% of circulating T3 comes from peripheral T4 → T3 conversion (only 20% secreted directly from thyroid)
- D2 is particularly important for brain and pituitary T3 supply; hypothyroidism upregulates D2 to protect these tissues
- Sick euthyroid / low T3 syndrome: D3 activation in illness shifts deiodination toward rT3, lowering active T3
Drugs that impair T4 → T3 conversion: propylthiouracil (PTU), propranolol, amiodarone, glucocorticoids, oral contrast agents, fasting
Cellular Action
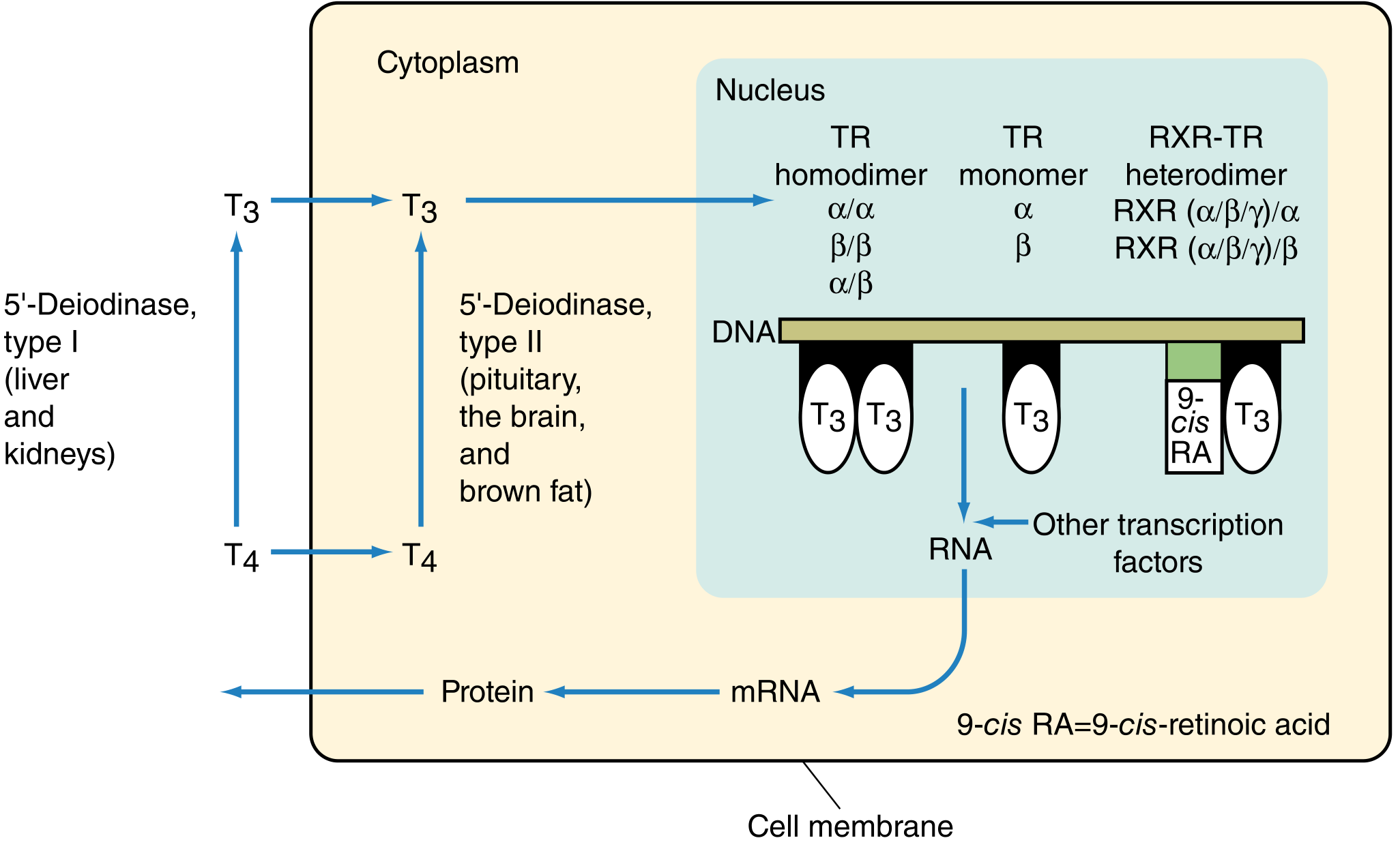
Cellular pathway: T4 enters the cytoplasm → converted to T3 by D1/D2 → T3 enters nucleus → binds TRα or TRβ (as homodimer, monomer, or RXR heterodimer) → binds thyroid response elements (TREs) on DNA → gene transcription → protein synthesis.
5. Other Metabolic Pathways
Conjugation (Hepatic and Renal)
- T4 and T3 undergo sulfation and glucuronidation in the liver and kidney, increasing water solubility
- Glucuronidated forms are excreted in bile; they may be deconjugated by gut bacteria and reabsorbed (enterohepatic circulation) - ~20% of T4 is excreted in feces
- Sulfated thyroid hormones are deiodinated and excreted in urine or feces
Decarboxylation / Thyronamines
- Iodothyronines can be further decarboxylated to thyronamines (biologically active metabolites)
- 3,5-T2 ("hot" hormone) - increases thermogenesis
- 3T1 ("cold" hormone) - decreases thermogenesis
- These nonclassical thyroid hormones are present at low plasma concentrations but are now recognized as having real physiologic effects
6. Nuclear Mechanism of Action
T3 is the primary intracellularly active form (relative metabolic potency T4:T3 = 0.3:1):
- Genomic actions: T3 binds nuclear thyroid hormone receptors (TRα, TRβ), which bind as monomers, homodimers, or heterodimers with retinoid X receptor (RXR) to thyroid response elements (TREs) in gene promoters → transcription of target genes
- TRα: abundant in brain, heart, muscle, kidney
- TRβ: high in pituitary and liver; TRβ2 mediates TSH negative feedback
- Nongenomic actions: T4 has higher affinity for cell-surface integrin αvβ3; rapid signaling via PI3K and cAMP kinase pathways (transcription-independent); direct mitochondrial effects increasing ATP production and oxygen consumption
Summary Table - Key Steps
| Step | Key Molecule / Enzyme | Site |
|---|---|---|
| Iodide uptake | NIS | Basolateral membrane |
| Iodide efflux into colloid | Pendrin | Apical membrane |
| H₂O₂ generation | DUOX2 | Apical membrane |
| Organification + coupling | TPO | Colloid |
| Tg proteolysis | Lysosomes | Follicular cell |
| MIT/DIT deiodination (recycling) | DEHAL1 (iodotyrosine deiodinase) | Follicular cell |
| T4 → T3 activation | D1, D2 | Liver, kidney, pituitary, brain |
| T4 → rT3 inactivation | D3 | Placenta, sick tissue |
| Conjugation | Sulfotransferases, UDP-glucuronosyltransferases | Liver, kidney |
Sources: Harrison's Principles of Internal Medicine 22E, Chapter 394 - Harrison's, p. 3065-3068 | Sabiston Textbook of Surgery, Chapter 73 - Sabiston Surgery, p. 1488-1490 | Tietz Textbook of Laboratory Medicine 7E - Tietz, p. 2308-2309
This is a shared conversation. Sign in to Orris to start your own chat.