Hyperkalemia treatment
Reading File
Finding Sources
Searching PubMed
"hyperkalemia" AND "treatment"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have excellent, comprehensive material. Here is the full answer:
Hyperkalemia Treatment
Overview
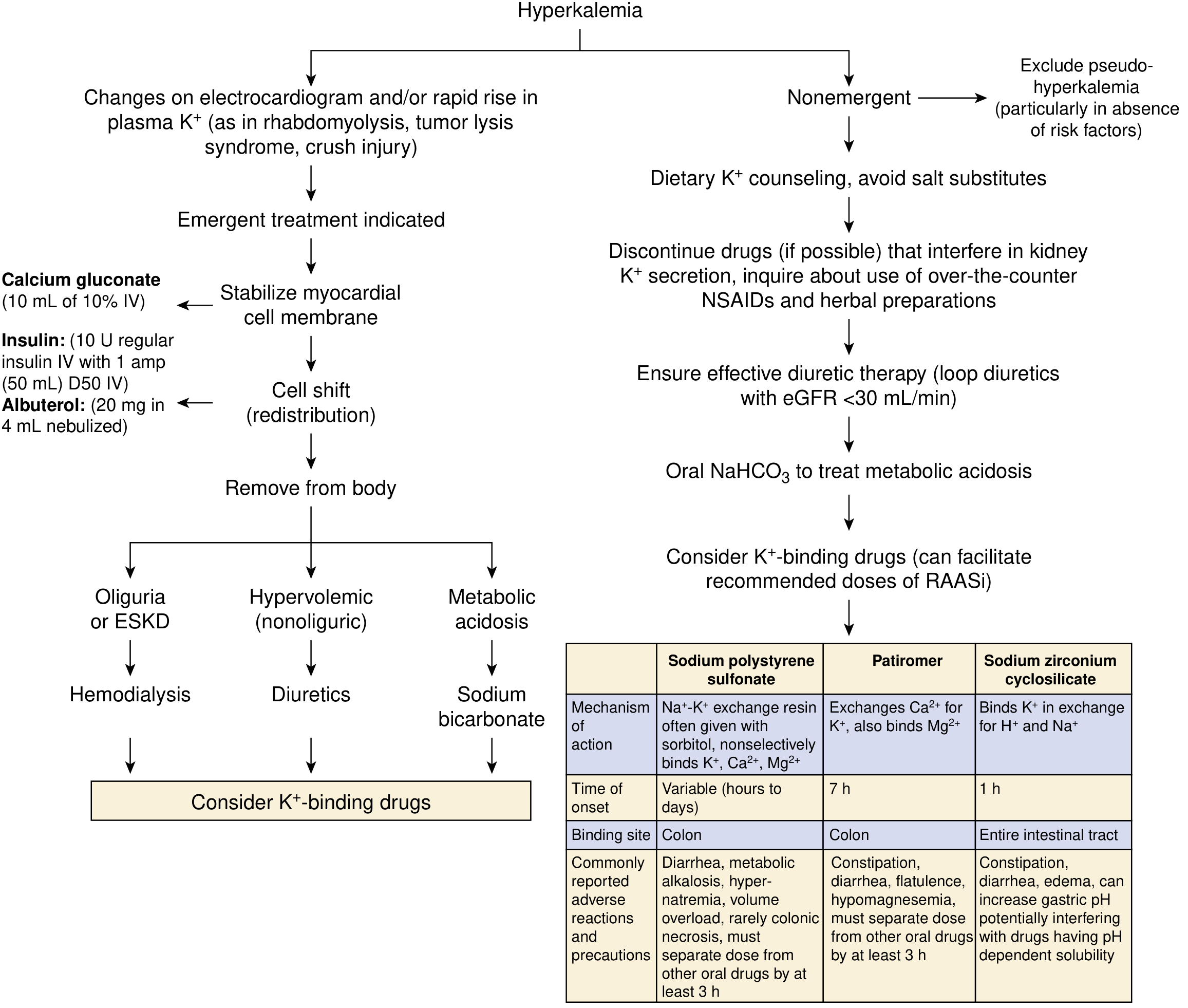
Treatment follows three sequential goals depending on severity:
- Stabilize the cardiac membrane (immediate)
- Shift K+ into cells (temporary, buys time)
- Remove K+ from the body (definitive)
A K+ >6-6.5 mEq/L, or any K+ with ECG changes, requires emergent management.
Step 1 - Cardiac Membrane Stabilization
Calcium gluconate (or calcium chloride)
- Dose: 10 mL of 10% calcium gluconate IV over 1-3 minutes
- Does NOT lower K+ - it raises the threshold potential and counteracts the depolarizing effect on myocardial membranes
- Onset: near-immediate; duration: 30-60 minutes
- Repeat if no ECG improvement within 3-5 minutes
- Calcium chloride has more elemental calcium but is caustic if it extravasates peripherally - avoid in peripheral IV access
- Caution in digoxin toxicity: calcium potentiates digoxin cardiac effects
Step 2 - Transcellular Shift (Temporizing)
a. Insulin + Dextrose
- Fastest pharmacological method to lower plasma K+
- Dose: 10 units regular insulin IV + 50 mL D50W (1 amp) bolus, followed by D5W infusion at 100 mL/hr to prevent late hypoglycemia
- Onset: 15 minutes; peak effect up to 1 hour
- Watch for hypoglycemia, especially in renal failure (insulin half-life is prolonged; lispro/aspart may reduce this risk)
- If blood glucose >300 mg/dL (e.g., diabetic), can give insulin alone without dextrose
- Never give dextrose alone - hyperglycemia without insulin can paradoxically raise K+
b. Albuterol (beta-2 agonist)
- Dose: 20 mg nebulized over 10 minutes (much higher than asthma dose, as only a fraction is absorbed)
- Onset: ~30 minutes; effect additive to insulin
- IV albuterol (0.5 mg) is equivalent but not available in the US
c. Sodium Bicarbonate
- Promotes cellular K+ uptake and enhances renal K+ excretion
- Useful when metabolic acidosis is present (serum HCO3 <10 mmol/L)
- Limited role in patients without residual kidney function or in acute emergency
- Does NOT enhance the K+-lowering effect of insulin or albuterol
- Dose: 50-100 mEq IV over 10-20 minutes
Step 3 - Potassium Removal (Definitive)
a. Diuretics
- Loop diuretics (furosemide) + thiazides promote renal kaliuresis
- Effective only if adequate kidney function is present
b. Dialysis
- The most definitive treatment for severe hyperkalemia
- Indicated when kidney function is severely impaired (severe AKI or ESKD)
- Typically cannot be initiated fast enough to replace the above temporizing measures - use them first
c. Potassium-binding resins (for non-emergency / chronic use)
| Agent | Mechanism | Onset | Dose | Notes |
|---|---|---|---|---|
| Sodium polystyrene sulfonate (SPS/Kayexalate) | Na+-K+ exchange resin in colon | Hours to days | 50 g oral in sorbitol or retention enema | FDA black-box warning: risk of colonic necrosis, especially with sorbitol; NOT for acute/urgent use |
| Patiromer | Binds K+ in exchange for Ca2+ in colon | ~7 hours | 8.4 g once daily (oral), titrate weekly | Approved for chronic hyperkalemia; causes hypomagnesemia; separate from other drugs by 3 hours |
| Sodium zirconium cyclosilicate (SZC) | Binds K+ in exchange for H+/Na+ throughout GI tract | ~1 hour (faster onset) | 10 g TID x 48 h, then 5-10 g once daily | 9x higher K+-binding capacity than SPS; can raise gastric pH |
SZC has the fastest onset among binders (~1 hour) and can potentially be used as an adjunct in urgent settings, though it is not a replacement for calcium or insulin/dextrose.
Nonemergent / Chronic Management
- Dietary K+ restriction and counseling; avoid salt substitutes (contain KCl)
- Discontinue offending drugs: ACE inhibitors, ARBs, potassium-sparing diuretics, NSAIDs, heparin, trimethoprim
- Loop diuretics when eGFR <30 mL/min
- Oral NaHCO3 if metabolic acidosis is present
- K+ binders (patiromer or SZC) allow continued use of RAASi when clinically needed
- Fludrocortisone if hyperkalemia is due to hypoaldosteronism
Quick Reference by ECG Finding
| ECG / Clinical Situation | Priority Action |
|---|---|
| Loss of P waves, wide/slurred QRS (near-arrest) | IV Calcium salts immediately |
| Peaked T waves (early changes) | Insulin + dextrose, consider dialysis |
| Elevated K+, no ECG changes | K+ binders, loop diuretics, dietary restriction |
Recent Evidence (2025)
A 2025 systematic review and meta-analysis (PMID 39761907) in Resuscitation on pharmacological interventions for acute hyperkalemia treatment provides updated evidence on the relative efficacy of insulin, albuterol, and bicarbonate. A separate network meta-analysis (PMID 40542996) in Drugs (2025) confirms novel K+ binders (patiromer, SZC) are effective in CKD/HF patients and enable continued RAASi use.
Sources: NKF Primer on Kidney Diseases 8e, p. 128-129; Morgan & Mikhail's Clinical Anesthesiology 7e, p. 2180; Sabiston Textbook of Surgery 21e
Anesthetic management noncardiac sugery for cardiac diseaes
Finding Sources
Searching PubMed
"noncardiac surgery" AND "cardiac risk" AND "anesthesia"
Finding Sources
Searching PubMed
"noncardiac surgery" AND "cardiac"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive material. Let me compile the full answer:
Anesthetic Management for Noncardiac Surgery in Cardiac Disease
1. Preoperative Cardiovascular Evaluation
Risk Assessment Framework (ACC/AHA)
Cardiovascular complications account for 25-50% of deaths following noncardiac surgery. Perioperative MI, pulmonary edema, arrhythmias, stroke, and thromboembolism are the main threats.
Step 1 - Assess surgical urgency
Emergency surgery proceeds without delay; risk modification happens postoperatively.
Step 2 - Screen for Active Cardiac Conditions (require cardiology intervention before elective surgery):
- Unstable coronary syndromes (unstable angina, recent MI <60 days)
- Decompensated heart failure (NYHA Class IV)
- Significant arrhythmias (high-degree AV block, symptomatic VT, uncontrolled AF)
- Severe valvular disease (severe AS, symptomatic MS)
Step 3 - Estimate Surgical Risk
- Low risk (<1% MACE): superficial, endoscopy, cataract, breast surgery
- Elevated risk (>1%): intraperitoneal, intrathoracic, orthopedic, prostate, head/neck
- High risk: aortic/major vascular surgery
Step 4 - Assess Functional Capacity (METs)
| METs | Activity | Implication |
|---|---|---|
| 1 MET | Self-care, walking indoors | Poor |
| 4 METs | Walk 1-2 blocks, light housework | Moderate |
| >10 METs | Strenuous sports (swimming, tennis) | Excellent |
Patients with >4 METs functional capacity and no active cardiac conditions can generally proceed to elevated-risk surgery without further cardiac testing.
Step 5 - Supplemental Preoperative Testing (Table 21-2 ACC/AHA)
| Test | Indication | Recommendation |
|---|---|---|
| 12-lead ECG | Known CAD, structural heart disease, non-low-risk surgery | IIa-B |
| LV function (Echo) | Unknown/worsening dyspnea or HF | IIa-C |
| Exercise stress test | Elevated risk + unknown functional capacity, if changes management | IIb-B |
| Pharmacological stress (DSE or MPI) | Elevated risk + poor functional capacity | IIa-B |
| Coronary angiography | Routine preoperative | Not recommended (III) |
2. Preoperative Medication Management
- Beta-blockers: Continue perioperatively - abrupt withdrawal risks rebound ischemia and tachycardia
- Statins: Continue - may be cardioprotective
- Antiplatelets (aspirin): Continue unless bleeding risk outweighs cardiac risk; dual antiplatelet therapy management depends on coronary stent timing
- ACE inhibitors/ARBs: Controversial - may cause intraoperative hypotension; some clinicians hold the morning dose but this risks rebound hypertension; decision should be individualized
- Diuretics: May cause hypokalemia - check electrolytes preoperatively
3. Intraoperative Anesthetic Management (ACC/AHA Table 21-10)
Choice of Anesthetic Technique
| Recommendation | COR | LOE |
|---|---|---|
| Either volatile anesthesia or TIVA is reasonable - no agent is clearly superior | IIa | A |
| Neuraxial anesthesia for postoperative analgesia after abdominal aortic surgery reduces MI | IIa | B |
| Epidural analgesia may reduce perioperative cardiac events in hip fracture patients | IIb | B |
| Prophylactic IV nitroglycerin is NOT effective in reducing intraoperative ischemia | III: No Benefit | B |
| Normothermia maintenance may reduce perioperative cardiac events | IIb | B |
Key Intraoperative Principles
For all cardiac patients:
- Avoid tachycardia (most important trigger for ischemia) - maintain HR <80 ideally
- Avoid hypertension and hypotension - both increase myocardial oxygen demand or reduce supply
- Avoid metabolic/respiratory acidosis
- Maintain normothermia
4. Monitoring
Standard + Advanced Monitoring
- Intraarterial pressure monitoring: Reasonable for severe CAD, major cardiac risk factors, or any procedure beyond minor surgery
- Central venous pressure: Useful in prolonged procedures with large fluid shifts
- Pulmonary artery catheter: May be considered when hemodynamics cannot be stabilized preoperatively; routine use NOT recommended (Class III, Level A)
- TEE: Reasonable for emergency use in hemodynamic instability during noncardiac surgery (IIa-C); routine intraoperative TEE during noncardiac surgery - not recommended (III: No Benefit)
ECG Monitoring
- Lead V5 detects ~75% of ischemic events; combination of II + V5 covers >90%
- Early ischemic changes: T-wave flattening or inversion
- Progressive: ST depression (subendocardial ischemia) or ST elevation (transmural ischemia)
- Hypertension + tachycardia are almost always the cause (not the result) of intraoperative ischemia
TEE for Ischemia Detection
- Regional wall motion abnormalities (RWMA) appear before ECG changes
- More sensitive early indicator than ECG
- Both regional and global abnormalities can also reflect changes in HR, preload, afterload, or drugs - not all RWMA = ischemia
5. Disease-Specific Management
A. Hypertensive Patients
- Continue antihypertensives up to surgery
- Elective surgery delay considered for sustained diastolic BP >110 mmHg
- Intraoperative: use depth of anesthesia and vasoactive drugs to control swings
- Postoperative: IV labetalol (hypertension + tachycardia); vasodilators if bradycardic
B. Ischemic Heart Disease (CAD)
- Maintain heart rate <80, MAP 60-80 mmHg
- Avoid succinylcholine if patient is digitalis-toxic (risk of arrhythmia)
- Treat intraoperative ischemia: increase O2 delivery (nitroglycerin for vasospasm), reduce demand (deepen anesthesia, beta-blocker if tachycardia, vasopressor if hypotension)
- Postoperative: continue monitoring, early re-ambulation, restart cardiac medications
C. Heart Failure
- Systolic HF: Avoid myocardial depressants; maintain preload/afterload; continue ACE-I/ARB, beta-blockers, diuretics perioperatively; watch for ACE-I-induced angioedema at intubation
- Diastolic HF: Maintain sinus rhythm, adequate filling time (avoid tachycardia), do not over-diurese
- BNP elevation preoperatively correlates with increased perioperative risk
- Optimize volume status before surgery
D. Hypertrophic Cardiomyopathy (HCM)
- Goal: minimize LVOT obstruction
- Maintain: adequate intravascular volume, normal/slow heart rate, increased SVR
- Avoid: vasodilation (reduces afterload - worsens obstruction), hypovolemia, tachycardia, inotropes
- Use beta-blockers; phenylephrine (pure alpha) preferred over ephedrine if vasopressor needed
E. Valvular Heart Disease
- Aortic Stenosis (severe): Maintain sinus rhythm, slow-normal HR, adequate preload; avoid vasodilation and hypotension (can be catastrophic); avoid spinal anesthesia
- Aortic Regurgitation: Avoid bradycardia (increases regurgitant volume); maintain slightly elevated HR; vasodilation is tolerated
- Mitral Stenosis: Maintain slow HR, sinus rhythm; avoid increases in pulmonary vascular resistance (hypoxia, hypercarbia, acidosis)
- Mitral Regurgitation: Slightly elevated HR; afterload reduction beneficial
6. Pacemakers and ICDs
Preoperative:
- Identify device type, indication, and programming; consult cardiologist
- Obtain device information card from patient; call manufacturer if needed
Intraoperative:
- Use bipolar electrocautery whenever possible to minimize electromagnetic interference (EMI)
- Place grounding pad far from the device
- Pacemaker-dependent patients: reprogram to asynchronous mode (VOO/DOO) before surgery
- ICDs: Consider disabling antitachycardia therapy before surgery; apply external defibrillation pads and keep attached to defibrillator
- Limit cautery to short bursts
- Magnet application: disables ICD antitachycardia function but does NOT convert pacemaker to asynchronous mode in most ICDs (consult manufacturer)
Postoperative:
- Interrogate device immediately after surgery to confirm all functions restored
- Monitor continuously until antitachycardia functions confirmed active
7. Arrhythmia Management
SVT:
- Hemodynamic collapse: synchronized cardioversion
- Stable: adenosine (AV block, breaks reentry), beta-blockers, non-DHP calcium channel blockers
- WPW: use procainamide or ibutilide - avoid amiodarone, adenosine, digoxin, verapamil (Class III - risk of accelerated ventricular response)
Atrial fibrillation: Rate control (beta-blockers, diltiazem); cardioversion if hemodynamically unstable; up to 35% of cardiac surgery patients develop postoperative AF
VT: Treat any broad complex tachycardia as VT until proven otherwise
8. Key 2024 Guideline Update
The 2024 AHA/ACC Guideline for Perioperative Cardiovascular Management (PMID 39316661) updated the stepwise risk algorithm, emphasizing the Revised Cardiac Risk Index (RCRI), biomarkers (BNP/NT-proBNP), and shared decision-making. Key updates include: greater use of preoperative NT-proBNP as a risk predictor, and refined guidance on antiplatelet management around coronary stents.
Sources: Morgan & Mikhail's Clinical Anesthesiology 7e, Chapter 21 (pp. 705-755); Sabiston Textbook of Surgery 21e; 2024 AHA/ACC Perioperative Cardiovascular Guidelines (PMID 39316661)
What is the Revised Cardiac Risk Index (RCRI) and how is it calculated?
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I have all the data needed - including the exact risk percentages from Miller's Anesthesia (VISION Study validated values). Here is the complete answer:
Revised Cardiac Risk Index (RCRI)
Background
The RCRI - also called the Lee Index - was derived and prospectively validated by Lee et al. (Circulation, 1999) to predict the risk of major cardiac complications in patients undergoing elective noncardiac surgery. It is the most widely endorsed preoperative cardiac risk tool, cited by the ACC/AHA, European Society of Cardiology (ESC), and European Society of Anaesthesiology guidelines.
The 6 Components - 1 Point Each
| # | Risk Factor | Criteria |
|---|---|---|
| 1 | High-risk surgery | Intraperitoneal, intrathoracic, or suprainguinal vascular surgery |
| 2 | Ischemic heart disease | History by any diagnostic criteria (angina, prior MI, positive stress test, Q waves on ECG, use of nitrates) |
| 3 | Congestive heart failure | History of CHF (pulmonary edema, paroxysmal nocturnal dyspnea, bilateral rales, S3 gallop, CXR with pulmonary vascular redistribution) |
| 4 | Cerebrovascular disease | History of stroke or TIA |
| 5 | Diabetes mellitus requiring insulin | Insulin-dependent diabetes only (not oral agents alone) |
| 6 | Preoperative renal impairment | Serum creatinine >2.0 mg/dL (>176 µmol/L) |
Each factor present = 1 point. Maximum possible score = 6.
Risk Interpretation
Risk percentages below are from the VISION Study validation (Roshanov et al., Can J Cardiol, 2021), as cited in Miller's Anesthesia 10e:
| RCRI Score | Risk of Major Cardiac Events* |
|---|---|
| 0 | 1.6% |
| 1 | 4.0% |
| 2 | 7.9% |
| ≥ 3 | 12.9% |
Major cardiac events = cardiac death, nonfatal MI, or nonfatal cardiac arrest.
Clinical threshold: Patients with ≥2 risk factors are considered elevated risk. Beta-blocker initiation (in currently untreated patients) should be considered several days before surgery in those with ≥3 RCRI points.
How to Calculate - Worked Example
Patient: 68-year-old man scheduled for colectomy (intraperitoneal), with history of angina, no CHF, no stroke, on insulin for T2DM, creatinine 1.4 mg/dL.
| Factor | Present? | Points |
|---|---|---|
| Intraperitoneal surgery | Yes | 1 |
| Ischemic heart disease (angina) | Yes | 1 |
| CHF | No | 0 |
| Cerebrovascular disease | No | 0 |
| Insulin-dependent DM | Yes | 1 |
| Creatinine >2.0 | No (1.4) | 0 |
| Total | 3 |
Score = 3 → ~12.9% risk of major cardiac events - elevated risk; consider further evaluation and perioperative beta-blockade.
Limitations
- Does not predict mortality - only cardiac morbidity
- Does not account for age as an independent variable
- Less accurate for vascular surgery patients (underestimates risk)
- Does not incorporate biomarkers (BNP/NT-proBNP), which the 2024 AHA/ACC guidelines now recommend as supplementary predictors
- The Gupta MICA calculator (derived from ACS NSQIP data) is an alternative that adds ASA class and age, and may be more accurate in some settings
Clinical Use in Guidelines (2024 Update)
The 2024 AHA/ACC Perioperative Cardiovascular Guideline (PMID 39316661) continues to recommend the RCRI as the primary clinical risk stratification tool, but now supplements it with:
- NT-proBNP/BNP - preoperative elevation is an independent predictor of MACE and should be measured in high-risk patients
- ACS NSQIP calculator as an acceptable alternative/supplement
Sources: Sabiston Textbook of Surgery 21e; Miller's Anesthesia 10e, p. 3884; Mulholland & Greenfield's Surgery 7e; Lee TH et al., Circulation 1999;100:1043-1049; Roshanov et al., Can J Cardiol 2021;37:1215-1224
How do you manage perioperative antiplatelet therapy in high RCRI patients?
Finding Sources
Finding Sources
Searching PubMed
"antiplatelet therapy" AND "perioperative" AND "noncardiac surgery"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
All key content retrieved. Here is the complete answer:
Perioperative Antiplatelet Management in High-RCRI Patients
The core challenge is balancing two competing risks:
- Continuing antiplatelet therapy → increased surgical bleeding
- Stopping antiplatelet therapy → stent thrombosis, MI, stroke
Management is stratified based on whether the patient has a coronary stent, the stent type, time since implantation, and the urgency/bleeding risk of the surgery.
Decision Framework - Coronary Stent Patients
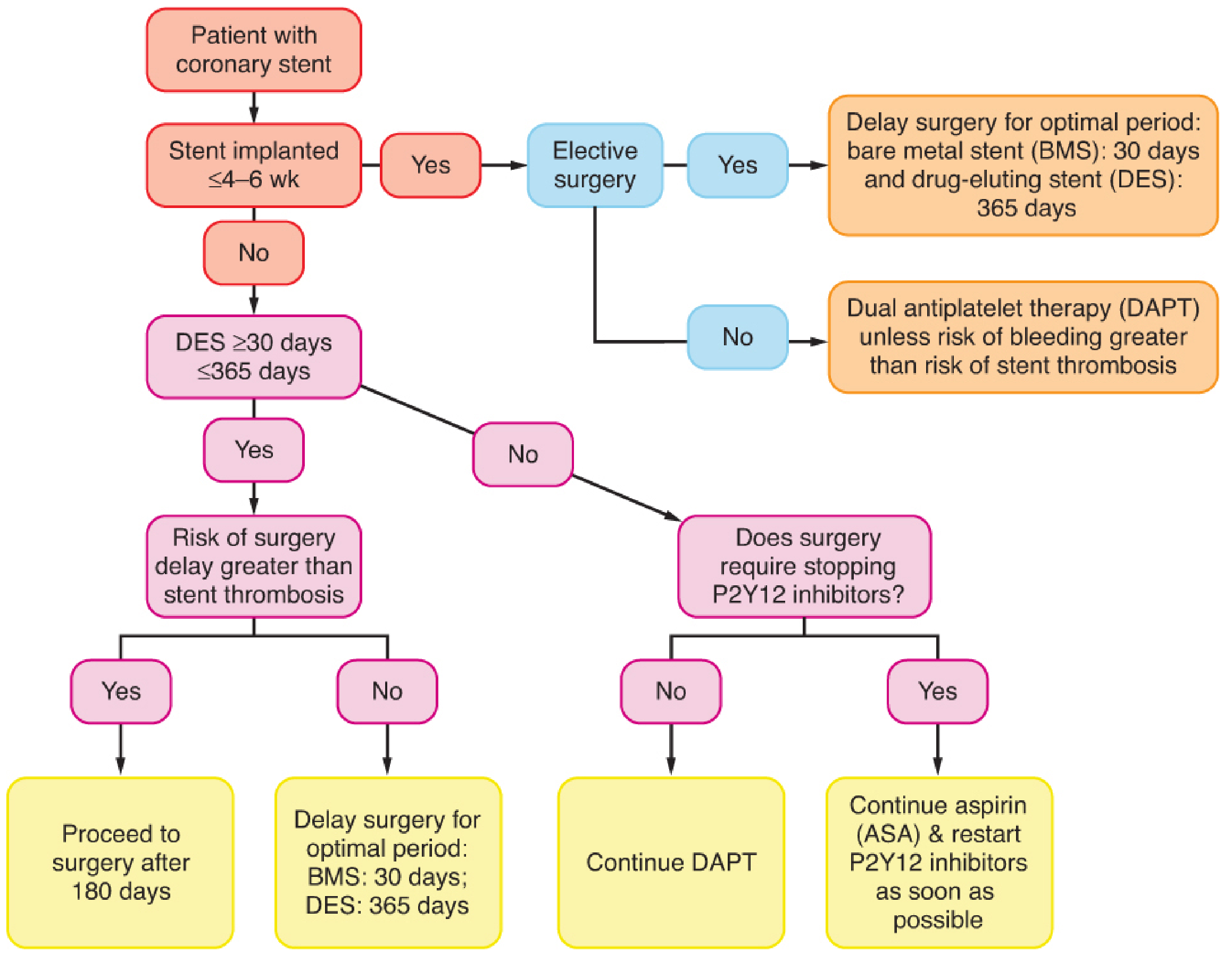
1. Timing of Surgery After Stent Implantation
The first 4-6 weeks after any stent placement represent the highest thrombosis risk window. Surgery during this period carries significant MACE risk and should be avoided whenever possible.
| Stent Type | Indication for PCI | Minimum DAPT Duration | Ideal Surgery Delay |
|---|---|---|---|
| Bare Metal Stent (BMS) | Any | 1 month | ≥30 days |
| Drug-Eluting Stent (DES) - older generation | Stable ischemic disease | 6 months | ≥6 months |
| DES - newer generation | Stable ischemic disease | 3 months | ≥3 months (can be 1 month in time-sensitive cases) |
| DES - any generation | ACS/acute MI | 12 months | ≥12 months (minimum 3 months for time-sensitive) |
The 2022 ESC guidelines updated these intervals to account for newer-generation DES, which have lower in-stent thrombosis rates than first-generation devices. PCI performed for ACS carries higher perioperative risk than elective PCI, even at the same time interval after implantation.
2. What to Do with Aspirin (Monotherapy or Part of DAPT)
In most high-RCRI patients with known CAD or prior stent: CONTINUE aspirin perioperatively.
The POISE-2 substudy of 470 patients with prior PCI found that continuing aspirin reduced the risk of death or MI by 50% (HR 0.50, 95% CI 0.26-0.95) without significantly increasing bleeding. This is a strong argument for aspirin continuation in high-risk patients.
Exceptions where aspirin may be held:
- Intracranial, spinal canal, or posterior eye surgery (bleeding in a closed space is catastrophic)
- Very high surgical bleeding risk where even aspirin is prohibitive - always a multidisciplinary decision
3. What to Do with P2Y12 Inhibitors (Clopidogrel, Prasugrel, Ticagrelor)
Hold times before surgery (to allow platelet function recovery):
| Agent | Hold Before Surgery |
|---|---|
| Clopidogrel | 5 days |
| Prasugrel | 7 days |
| Ticagrelor | 3-5 days |
When to hold:
- Surgery requires stopping the P2Y12 inhibitor (most major surgeries)
- Patient is beyond the minimum DAPT duration for their stent type
- Plan: continue aspirin, stop P2Y12, restart P2Y12 as soon as possible after surgery (within 24-48 hours ideally)
When to continue DAPT:
- Surgery does not require stopping P2Y12 inhibitors (minor procedures, dental extractions with local hemostasis)
- Within the mandatory DAPT window and surgery cannot be delayed
4. Bridging Therapy - Heparin is NOT an Option
A common historical misconception was to "bridge" patients off DAPT with heparin.
This is wrong and potentially harmful:
- Heparin and LMWH do not substitute for antiplatelet protection against stent thrombosis
- Heparin can paradoxically increase platelet aggregation
- Neither ACC/AHA nor ESC guidelines recommend heparin bridging for antiplatelet therapy discontinuation
What about GP IIb/IIIa inhibitors or IV P2Y12 agents?
For patients at very high risk of stent thrombosis who must undergo surgery (e.g., stent placed <30 days ago, emergency surgery required), bridging with:
- IV reversible glycoprotein IIb/IIIa inhibitors (tirofiban, eptifibatide) - short half-life, can be stopped 4-8 hours before surgery
- IV reversible P2Y12 inhibitor (cangrelor) - half-life ~3-5 minutes, discontinued 1 hour before surgery
This approach remains controversial with inconclusive evidence. It should be reserved for high-risk cases in centers with immediate interventional cardiology access.
5. Key Principles for Non-Stent High-RCRI Patients (Aspirin Only)
For patients on aspirin monotherapy for primary or secondary prevention without stents:
| Situation | Recommendation |
|---|---|
| Secondary prevention (prior MI, stroke, PAD) | Continue aspirin perioperatively |
| High-RCRI + elevated cardiac risk, no stent | Continue aspirin unless high bleeding-risk surgery |
| Primary prevention only | May hold aspirin (risk-benefit often favors holding) |
6. Multidisciplinary Decision-Making
All high-RCRI patients with coronary stents undergoing noncardiac surgery should have their antiplatelet plan developed by a team including:
- Anesthesiologist
- Surgeon
- Cardiologist/interventional cardiologist
Surgery in patients with recent stent placement should ideally be performed only at centers with immediate access to interventional cardiology for rescue PCI if needed.
7. Postoperative Monitoring
- Serial troponin measurement in high-RCRI patients postoperatively (watch for perioperative myocardial injury, MINS)
- Restart P2Y12 inhibitor as soon as hemostasis is confirmed - delay increases stent thrombosis risk
- Any suspected stent thrombosis: emergent PCI is the treatment of choice
Summary Algorithm
High-RCRI patient → has coronary stent?
│
YES → When was stent placed?
│ ├─ <30 days → Delay elective surgery; if urgent, maintain DAPT + interventional cardiology on standby
│ ├─ 30 days-6 months (DES) → Weigh risk of delay vs. stent thrombosis; if must proceed: continue aspirin, hold P2Y12 (5-7 days), restart ASAP
│ └─ >6 months (DES) or >30 days (BMS) → Continue aspirin; hold P2Y12 5-7 days before; restart ASAP after surgery
│
NO → Continue aspirin if secondary prevention; hold only for high-bleeding-risk surgery
Do NOT bridge with heparin
Sources: Miller's Anesthesia 10e, pp. 3897-3898 & 6776; Barash's Clinical Anesthesia 9e, p. 1772; Harrison's Principles of Internal Medicine 22e, p. 3951; POISE-2 substudy (Devereaux et al.); 2024 AHA/ACC Perioperative Guideline PMID 39316661
This is a shared conversation. Sign in to Orris to start your own chat.