lumbar puncture neurology and neuro surgery
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Now I have comprehensive material to write a thorough answer. Let me compile everything.
Lumbar Puncture - Neurology & Neurosurgery
Overview
Lumbar puncture (LP) is the procedure of inserting a needle into the lumbar subarachnoid space to obtain cerebrospinal fluid (CSF), measure intracranial pressure, or instill therapeutic agents. It is one of the most important diagnostic tools in neurology and neurosurgery.
- Adams and Victor's Principles of Neurology, 12th Ed.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
- Pye's Surgical Handicraft, 22nd Ed.
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma
Anatomy
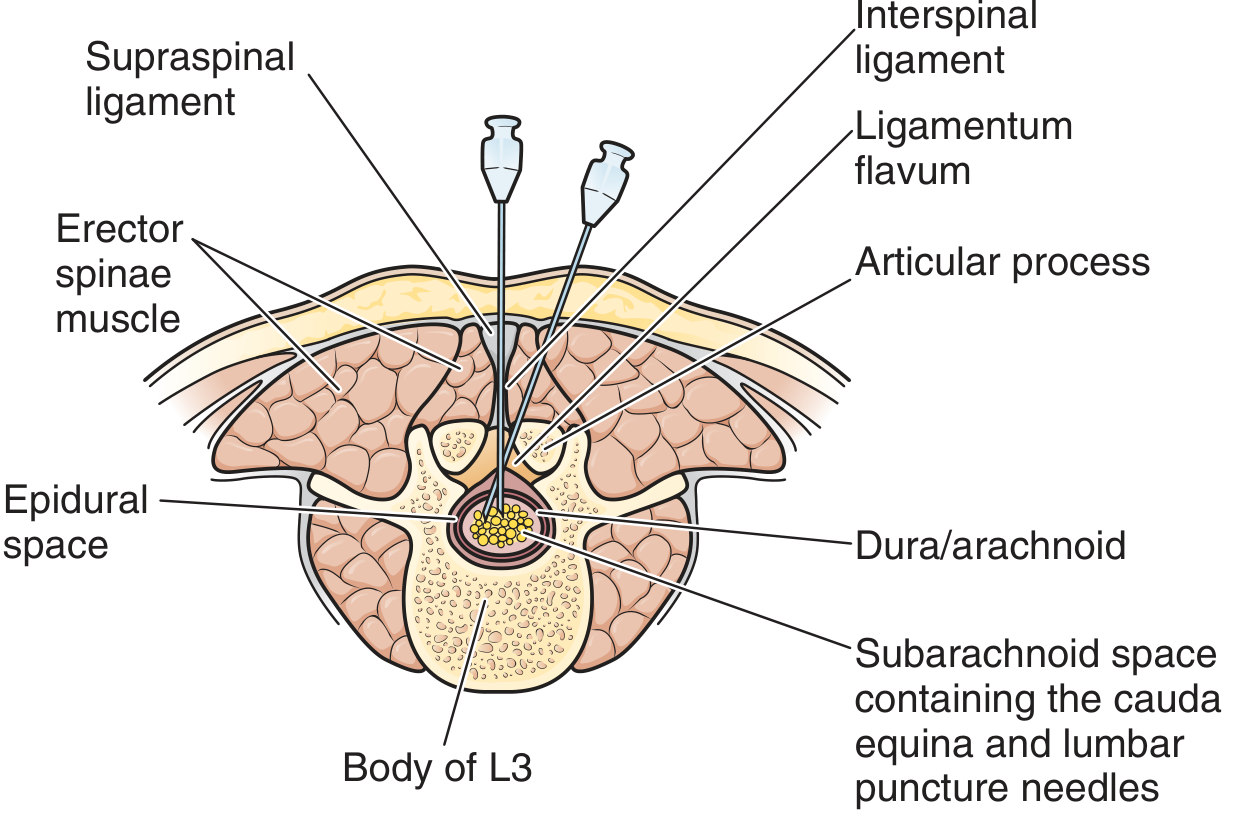
The needle is inserted between L3-L4 or L4-L5 (below the termination of the spinal cord at L1-L2). The structures penetrated in order are:
- Skin and subcutaneous fat
- Supraspinal ligament
- Interspinous ligament
- Ligamentum flavum (a distinct "give" is felt here)
- Epidural space
- Dura mater + arachnoid mater (another "give" felt)
- Subarachnoid space - CSF obtained here (cauda equina floats freely)
Midline approach passes through all ligaments. The lateral (paramedian) approach avoids the supraspinous ligament (important if calcified) and only pierces the ligamentum flavum.
Indications
Diagnostic:
- Suspected meningitis (bacterial, viral, tuberculous, fungal)
- Suspected subarachnoid hemorrhage (SAH) when CT is negative but clinical suspicion is high
- Encephalitis (viral, autoimmune)
- Carcinomatous meningitis / leptomeningeal spread
- CNS lymphoma / leukemia (including CNS staging)
- Neurosyphilis, neuroborreliosis
- Demyelinating disease (multiple sclerosis - oligoclonal bands)
- Guillain-Barre syndrome (albuminocytologic dissociation)
- Normal pressure hydrocephalus (opening pressure + gait/cognition response to drainage)
- Myelography / radionuclide cisternography (contrast instillation)
Therapeutic:
- Intrathecal antibiotics, antifungals, or antitumor agents (e.g., methotrexate)
- Spinal anesthesia instillation
- CSF drainage for pseudotumor cerebri (idiopathic intracranial hypertension) - repeated LP may be therapeutic
- Reduce drug concentration in CSF (e.g., inadvertent intrathecal drug overdose - additional 30-40 mL CSF withdrawn)
Patient Positioning
Two positions are used:
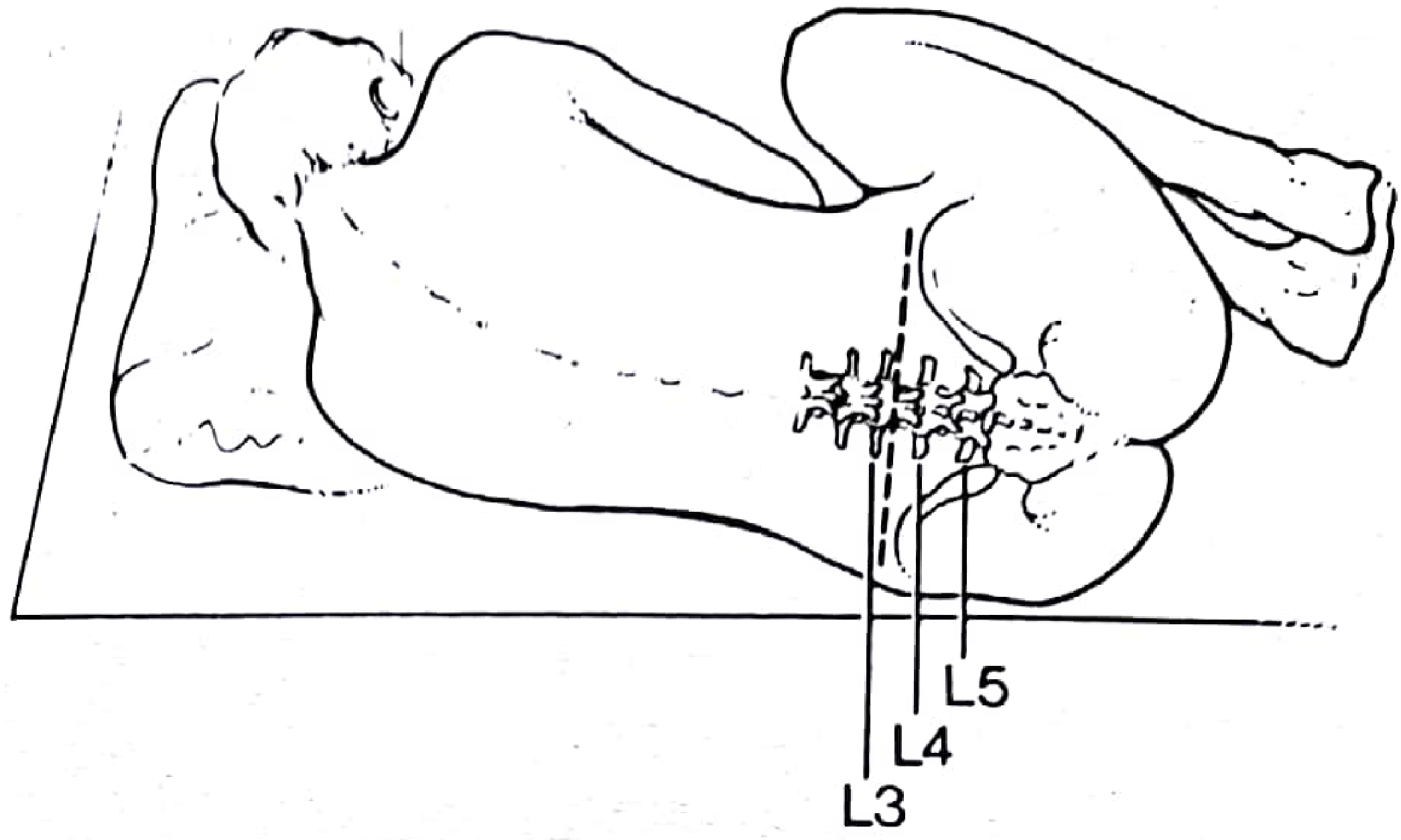
1. Left lateral decubitus (fetal position) - most common:
- Patient lies on their left side with hips, knees, and neck fully flexed (knees to chest, chin tucked)
- Maximally opens the interspinous spaces
- Allows accurate opening pressure measurement
2. Sitting position:
- Patient sits upright, hunched forward with arms resting on a pillow
- Useful in obese patients or when midline identification is difficult
- Better for procedures in infants
- Note: opening pressure measurement is unreliable in this position
Pre-Procedure Assessment
Before LP, always assess for:
- Signs of raised ICP: headache, papilledema, altered consciousness, focal neurological signs
- Coagulation status: INR ≤1.4 and platelets >50,000/mm³ are generally acceptable; aspirin alone at conventional doses is not a contraindication
- Infection at the proposed skin site: cellulitis is a contraindication
- Spinal anatomy: prior surgery, spinal stenosis, or deformity may complicate access
When to obtain CT first (before LP):
- Age ≥60 years
- Immunocompromised state
- History of CNS disease (mass, stroke, focal infection)
- Seizure within 1 week
- Altered level of consciousness
- Focal neurological findings (papilledema, gaze palsy, arm drift, leg drift, facial palsy, abnormal visual fields)
(Hasbun et al. criteria, N Engl J Med 2001 - if any of these features are present, CT head first)
Technique (Step-by-Step)
- Explain the procedure to the patient and obtain consent
- Position the patient (lateral decubitus, hips and neck flexed)
- Identify the L3-L4 or L4-L5 interspace using the posterior superior iliac crest as a surface landmark (Tuffier's line = line connecting the iliac crests = approximately L4 spinous process)
- Prepare the skin with antiseptic solution using aseptic technique, drape the area
- Infiltrate ~2 mL of 1% lidocaine (lignocaine) into the skin and subcutaneous tissue
- Insert the LP needle (with stylet in place) in the midline, aimed slightly cephalad (toward the umbilicus), advancing through each layer
- A "give" (loss of resistance) is felt as the needle passes through the ligamentum flavum; a second give as it pierces the dura
- Remove the stylet - CSF should drip freely
- Attach a manometer and measure opening pressure (normal: 70-180 mm H₂O in lateral decubitus)
- Collect CSF into numbered tubes (typically 4 tubes, 1-2 mL each)
- Measure closing pressure if desired
- Replace stylet before removing the needle (reduces post-LP headache)
- Apply firm dressing; patient kept supine
Needle selection: Atraumatic (pencil-point, Sprotte or Whitacre) needles significantly reduce post-LP headache compared to standard Quincke (cutting-bevel) needles. Gauge 20 or smaller is preferred; needles larger than 20G may double the incidence of post-LP headache.
CSF Analysis - Normal Values & Formulas
| Parameter | Normal Range |
|---|---|
| Opening pressure | 70-180 mm H₂O (lateral decubitus) |
| Appearance | Clear, colorless |
| WBC | 0-5 cells/mm³ (all lymphocytes) |
| RBC | 0 |
| Protein | 15-45 mg/dL |
| Glucose | 50-80 mg/dL (~60-70% of serum glucose) |
Characteristic CSF Profiles (from Adams & Victor, Table 2-1)
| Condition | Cells | Protein | Glucose | Other |
|---|---|---|---|---|
| Bacterial meningitis | WBC >50/mm³ (often thousands), neutrophil predominant | 100-250 mg/dL | <50 mg/dL (<50% blood glucose) | Gram stain positive; pressure elevated |
| Viral/fungal/spirochetal | WBC 10-100/mm³, lymphocyte predominant | 50-200 mg/dL | Normal or slightly reduced | Special cultures needed |
| Tuberculous meningitis | WBC >25/mm³, lymphocytes | 100-1000 mg/dL | <50 mg/dL, markedly reduced | PCR and special cultures; smear low sensitivity |
| Subarachnoid hemorrhage | RBC >500/mm³; slight WBC increase | 60-150 mg/dL | Normal initially, slightly reduced later | Xanthochromia differentiates from traumatic tap |
| Guillain-Barre syndrome | Normal or slight increase | Markedly elevated (200-400+ mg/dL) | Normal | Albuminocytologic dissociation |
| MS / demyelinating | Normal or mild lymphocytosis | Normal or mildly elevated | Normal | Oligoclonal bands; elevated IgG index |
| Carcinomatous meningitis | Variable; malignant cells on cytology | Elevated | Reduced | Malignant cells; repeat LP increases yield |
LP for Subarachnoid Hemorrhage
When CT is negative but SAH is clinically suspected, LP remains the gold standard to exclude SAH:
- RBC count in CSF - counts <500/mm³ make SAH exceedingly unlikely
- Xanthochromia (yellow tint due to hemoglobin breakdown): appears 2-4 hours after SAH, persists up to 4 weeks; indicates true blood in subarachnoid space, not traumatic tap
- Traumatic tap vs. true SAH:
- Traumatic tap: RBCs clear between tube 1 and tube 4 (≥25-30% reduction); blood may streak into clear CSF; clot may form in tube (defibrination occurs at hemorrhage site in SAH, so clot does NOT form)
- True SAH: uniform blood across all tubes; xanthochromia present; no clot formation
- D-dimer in CSF can identify fibrinolysis as evidence of SAH (false positives with DIC, prior traumatic tap, or thrombolytics)
- Fluoroscopically guided LP reduces traumatic tap rate but requires radiology suite
Contraindications
Absolute:
- Infection (cellulitis) overlying the LP site
- Clinical evidence of herniation (Cushing's triad, blown pupil, decorticate/decerebrate posturing)
- Suspected intracranial mass with mass effect (asymmetric lesions near tentorium or foramen magnum are particularly dangerous)
Relative:
- Raised ICP without known cause (get CT first)
- Coagulopathy (INR >1.4, platelets <50,000)
- Anticoagulant therapy (timing depends on agent - see below)
- Spinal deformity, prior lumbar surgery
Key principle: A normal CT scan does NOT eliminate the risk of herniation post-LP. Herniation occurs in approximately 5% of patients with acute bacterial meningitis and accounts for ~30% of deaths in this condition.
Anticoagulation and LP
| Drug | Recommended Hold Before LP |
|---|---|
| Aspirin alone (standard dose) | Generally safe; no hold required |
| NSAIDs alone | Generally safe |
| Clopidogrel / ticlopidine | 7-10 days (ASRA/AHA) or minimum 5 days |
| Tirofiban / eptifibatide | 8 hours |
| Abciximab | 24-48 hours |
| Unfractionated heparin (IV infusion) | Discontinue infusion; wait until aPTT in safe range |
| LMWH (therapeutic) | 24 hours |
| Warfarin | INR must be ≤1.4 |
| NOACs (direct oral anticoagulants) | Allow anticoagulant effect to wear off or use reversal agent |
- Aspirin + any other anticoagulant: do NOT proceed without risk-benefit assessment
- Spinal epidural hematoma (SEH) is the most feared complication in anticoagulated patients - presents with back pain, progressive leg weakness, bowel/bladder dysfunction; treat with emergency MRI and laminectomy
Complications
| Complication | Notes |
|---|---|
| Post-LP headache (PLPH) | Most common; orthostatic/positional (worse upright, better supine); due to persistent CSF leak through dural hole; incidence reduced with atraumatic/smaller needles; treat with supine rest, hydration, caffeine, or epidural blood patch |
| Cranial nerve palsy | Most common: CN VI (abducens - causes lateral gaze palsy); also CN III, IV; due to intracranial hypotension and traction on nerves; resolves when CSF pressure normalizes |
| Brain herniation | Rare but catastrophic; risk highest with asymmetric mass lesions, papilledema; can be transtentorial (uncal) or tonsillar (foramen magnum) |
| Spinal epidural hematoma (SEH) | Rare; risk increased dramatically in anticoagulated patients or with traumatic LP; presents as back pain + paraplegia; emergency laminectomy required |
| Infection (meningitis/arachnoiditis) | Very rare with strict aseptic technique |
| Traumatic tap | Blood-contaminated CSF; usually from epidural vein puncture; clears between tubes |
| Back pain | Common, usually self-limited |
| Radicular pain | If needle deflected laterally and contacts a nerve root; withdraw and redirect |
| Intraspinal epidermoid tumor | Late complication if procedure performed repeatedly without a stylet (especially in neonates) |
Special Situations
LP in Meningitis
- Do not delay empiric antibiotics to wait for LP if there is clinical concern - draw blood cultures and treat
- Only a large brain abscess or substantial brain swelling absolutely contraindicates LP in suspected bacterial meningitis
- CSF protein >45 mg/dL in >90% of bacterial meningitis cases
- CSF glucose <40 mg/dL or <50% of blood glucose suggests bacterial meningitis
- WBC >50,000/mm³ raises possibility of brain abscess ruptured into a ventricle
- Normal CSF pressure in bacterial meningitis should raise suspicion of needle occlusion or spinal block
LP in Infants
- Sitting position preferred (better midline identification)
- Avoid tight neck flexion - can cause airway obstruction
- Preoxygenation is recommended, especially in neonates with respiratory distress
- Use stylet during advancement and on withdrawal to prevent epidermoid implantation
- Opening pressure measurement unreliable in a struggling infant
Normal Pressure Hydrocephalus (NPH)
- Classic triad: gait apraxia, dementia, urinary incontinence ("wet, wacky, wobbly")
- LP serves both diagnostically (opening pressure typically 150-200 mm H₂O, within normal but in upper range) and therapeutically (large-volume LP - 30-50 mL removed; improvement in gait predicts response to VP shunt)
Pseudotumor Cerebri (IIH)
- Elevated opening pressure (>250 mm H₂O); therapeutic LP removes enough CSF to lower pressure and relieve headache/visual symptoms
- Repeated LPs are used as a temporizing measure while medical therapy (acetazolamide, weight loss) or surgical shunting is arranged
- LP is safer here than in mass lesions because ventricles communicate freely
Post-LP Headache Management
- Orthostatic headache beginning 24-48 hours after LP, lasting up to 2 weeks
- Mechanism: persistent dural leak → CSF hypotension → downward displacement of brain → traction on pain-sensitive structures
- Cranial nerve palsies (especially CN VI) may accompany severe PLPH due to traction from intracranial hypotension
- Conservative: supine rest, oral/IV hydration, caffeine (300-500 mg)
- Definitive: Epidural blood patch (autologous blood 10-20 mL injected into epidural space at same level) - highly effective (>85% success rate), considered gold standard for refractory PLPH
Summary
Lumbar puncture is indispensable in neurology and neurosurgery for diagnosing meningitis, SAH, demyelinating disease, and leptomeningeal spread, as well as for therapeutic drainage and intrathecal drug delivery. Safe execution requires confirming the absence of contraindications (especially raised ICP with mass effect), using appropriate needle size and technique, and monitoring for complications - particularly post-LP headache and, in anticoagulated patients, spinal epidural hematoma.
- Adams and Victor's Principles of Neurology, 12th Ed., p. 25 (Table 2-1 CSF formulas; LP technique)
- Roberts and Hedges' Clinical Procedures in Emergency Medicine (Chapter 60 - Lumbar Puncture, pp. 1436-1444)
- Pye's Surgical Handicraft, 22nd Ed., p. 2587 (procedure description)
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma, p. 414 (herniation risk, post-LP headache)
This is a shared conversation. Sign in to Orris to start your own chat.