Tell me about cow mik protein allergy in detail
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cow's milk protein allergy" AND management
Finding Sources
Finding Sources
Searching PubMed
"cow milk allergy" AND diagnosis
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching the Web
cow milk protein allergy CMPA pathophysiology diagnosis management 2024 2025
Reading File
Reading File
Reading Article
PMID: 40534871
Loading Image
Loading Image
I now have thorough information from multiple authoritative sources. Here is the comprehensive answer:
Cow's Milk Protein Allergy (CMPA) - A Detailed Overview
Cow's milk protein allergy (CMPA) is the most common food allergy in young children and one of the earliest allergens encountered in life. It is an immune-mediated hypersensitivity reaction to proteins in cow's milk - distinct from lactose intolerance, which is a non-immune, enzyme-deficiency disorder.
1. Epidemiology
- Affects approximately 2-3% of infants globally; some estimates run higher.
- More common in formula-fed than breastfed infants.
- Resolves in the majority of cases during childhood (most children tolerate milk by age 5-6 years).
- Uncommon in adults.
- Rising reported prevalence of food allergies globally.
2. The Culprit Proteins
Cow's milk contains over 25 proteins, but the main allergens are:
| Protein | Type | Notes |
|---|---|---|
| Casein | 80% of milk protein | Major allergen; heat-stable; cross-reacts with other ruminant milks |
| Beta-lactoglobulin (β-LG) | Whey protein | Absent in human breast milk; major sensitizer |
| Alpha-lactalbumin (α-LA) | Whey protein | Present in human milk; less allergenic |
| Bovine serum albumin (BSA) | Whey protein | Minor allergen |
Casein and β-lactoglobulin are the two clinically most significant allergens.
3. Immunological Classification
CMPA is broadly divided into three types based on immunologic mechanism:
3a. IgE-Mediated (Immediate-Type) CMPA
- Accounts for approximately 50% of cases.
- Reaction onset: within minutes to 2 hours of exposure.
- Involves sensitization of mast cells via IgE antibodies.
The three-phase mechanism:
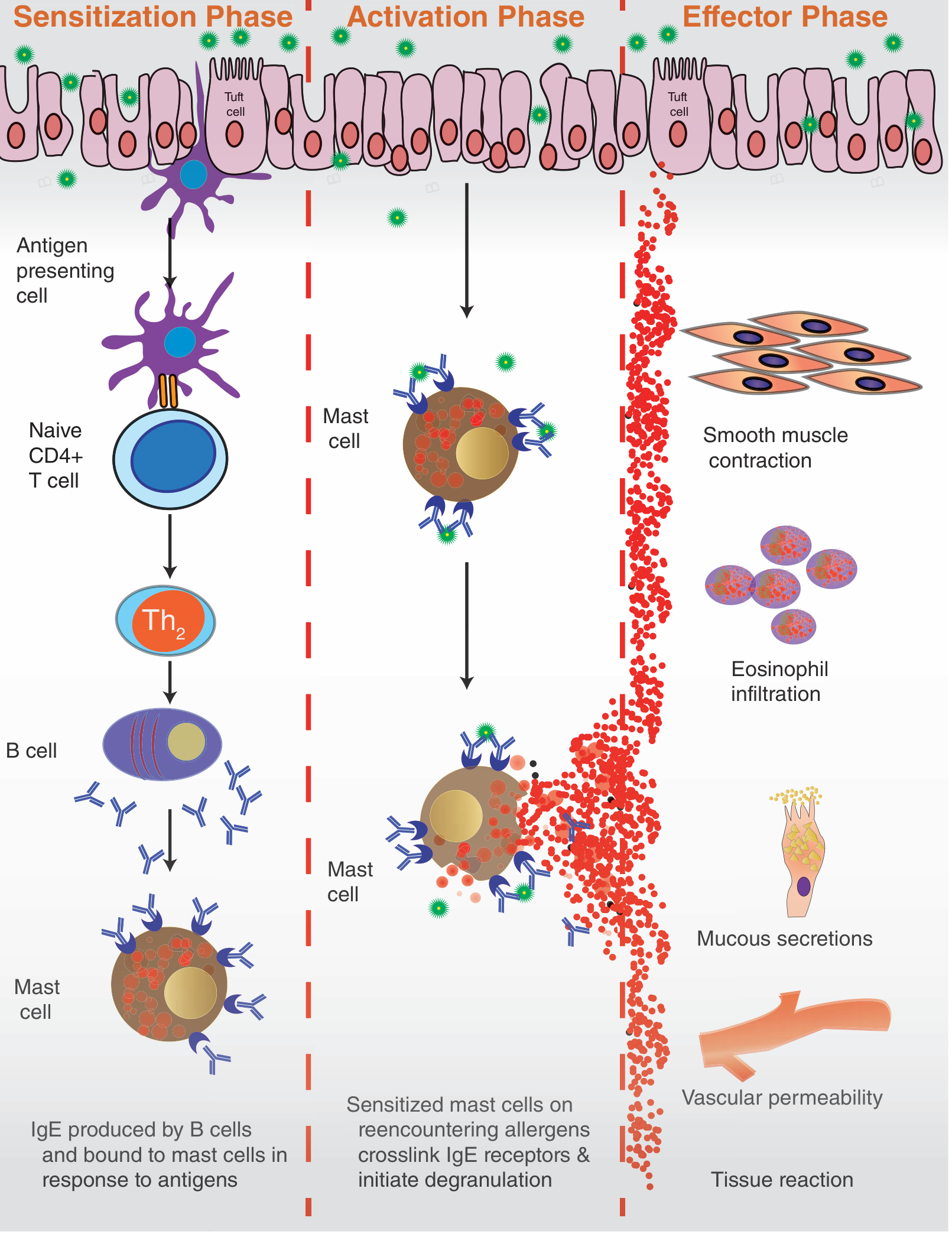
- Sensitization Phase: Antigen-presenting cells present milk proteins to naive CD4+ T cells → Th2 polarization → B-cell class switching → IgE production → IgE binds to mast cell Fc receptors.
- Activation Phase: Re-exposure to milk proteins cross-links mast cell-bound IgE → degranulation.
- Effector Phase: Release of histamine, prostaglandins, leukotrienes → smooth muscle contraction, mucous secretion, eosinophil recruitment, vascular permeability.
Susceptible individuals show:
- Predominance of Th2 lymphocytes with elevated IL-4 and IL-5
- Enhanced mast-cell degranulation
- Increased antigen resorption due to loss of mucosal integrity
- Genetic predisposition (atopic background)
3b. Non-IgE-Mediated (Delayed-Type) CMPA
- T-cell and eosinophil-mediated.
- Reaction onset: hours to days after exposure.
- Skin-prick tests and serum-specific IgE are typically negative.
- Harder to diagnose.
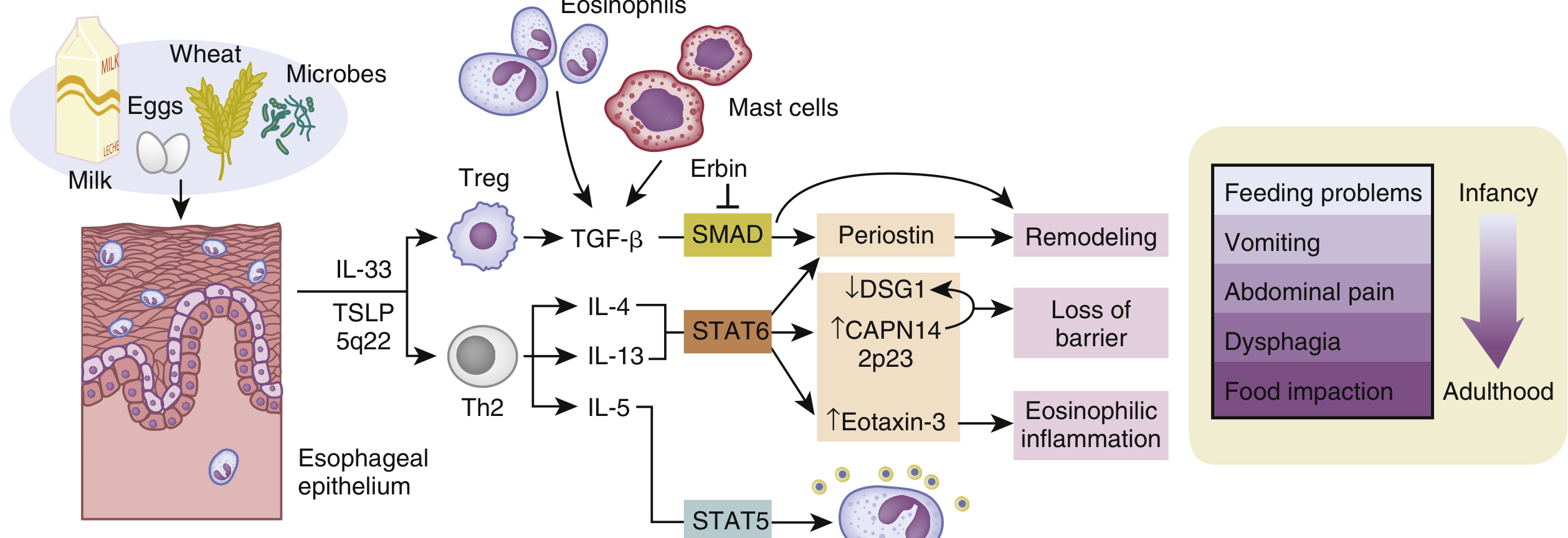
3c. Mixed (IgE + Non-IgE) CMPA
- Seen in eosinophilic esophagitis (EoE), eosinophilic gastroenteritis, and allergic eosinophilic proctocolitis.
4. Sensitization Pathways
Sensitization can occur through:
- Skin barrier disruption (especially eczema/atopic dermatitis) - now recognized as a major primary sensitization route.
- Gut exposure to undegraded protein antigens circulating in the bloodstream.
- The intestinal microbiome plays a role: disease-associated dysbiosis can promote food allergy susceptibility.
5. Clinical Manifestations
CMPA is a multi-system disease. Symptoms depend on the immune mechanism, degree of sensitization, and patient age.
Cutaneous (most common, ~50-70%)
- Urticaria and angioedema (IgE-mediated, immediate)
- Worsening of atopic dermatitis/eczema (often delayed, mixed)
- Flushing
Gastrointestinal (~50-60%)
- Reflux, regurgitation, vomiting
- Abdominal cramping, colic, bloating
- Diarrhea (with or without blood)
- Constipation
- Hematemesis, melena (blood in stool)
- Malabsorption, failure to thrive
- Allergic gastritis (mucosal hemorrhage, neutrophilic and eosinophilic infiltrate on biopsy)
Respiratory (~20-30%)
- Rhinitis, nasal congestion
- Wheezing, asthma exacerbation
- Cough
- Rarely: Heiner syndrome (food-induced pulmonary hemosiderosis) - diffuse pulmonary hemorrhage associated with cow's milk protein allergy in infants
Systemic
- Anaphylaxis (severe, life-threatening; IgE-mediated; risk is real with true IgE-mediated CMPA)
6. Specific Non-IgE-Mediated Syndromes (Cow's Milk as a Key Trigger)
| Syndrome | Primary Mechanism | Key Features |
|---|---|---|
| FPIES (Food Protein-Induced Enterocolitis Syndrome) | Non-IgE (T cell/innate) | Profuse vomiting 2-4 hrs post-ingestion; pallor, lethargy, hypotension (shock-like); milk + soy are top triggers |
| FPIAP (Food Protein-Induced Allergic Proctocolitis) | Non-IgE | Healthy infant with bloody, mucoid stools; benign self-limiting; sigmoidoscopy shows eosinophils |
| FPE (Food Protein-Induced Enteropathy) | Non-IgE | Non-bloody persistent diarrhea; malabsorption; hypoalbuminemia; NOT seen in exclusively breastfed infants |
| Heiner Syndrome | Mixed | Pulmonary hemosiderosis; diffuse pulmonary hemorrhage; infants |
FPIES deserves special mention: it is often misdiagnosed as sepsis, gastroenteritis, or a surgical emergency. Chronic FPIES (only from continuous cow's milk or soy exposure) presents with persistent vomiting/diarrhea and growth failure.
7. Diagnosis
There is no single gold-standard test for CMPA. Diagnosis is clinical and stepwise.
History
- Timing and pattern of symptoms after milk intake
- Family history of atopy
- Response to milk elimination
Allergy Testing (for IgE-mediated CMPA)
| Test | Notes |
|---|---|
| Skin-prick test (SPT) | Positive = ≥3 mm wheal; high sensitivity but variable specificity |
| Serum-specific IgE (sIgE) | For casein, β-LG, α-LA; elevated sIgE confirms sensitization, not necessarily allergy |
| Component-resolved diagnostics (CRD) | sIgE to specific components (e.g., casein sIgE) - better predictor of persistent allergy |
Important: Elevated IgG to milk proteins does NOT indicate allergy - it reflects only food exposure. Do not use IgG testing for diagnosis.
Fecal calprotectin is elevated in CMPA but not recommended as a routine diagnostic tool due to limited data.
Elimination and Challenge
- Elimination diet: Remove all cow's milk protein from diet (and from maternal diet if breastfeeding) for 2-4 weeks.
- Symptom resolution with elimination supports CMPA.
- Oral Food Challenge (OFC) / Double-Blind Placebo-Controlled Food Challenge (DBPCFC) - considered the diagnostic gold standard. Carries anaphylaxis risk in IgE-mediated cases; must be done in a supervised setting.
Endoscopy (when needed)
- Can rule out eosinophilic esophagitis, Crohn's disease.
- Allergic gastritis on biopsy shows eosinophilic and neutrophilic infiltrate with mucosal hemorrhage.
8. Management
Step 1: Avoidance
- Complete elimination of cow's milk protein from the diet is the foundation of management.
- In breastfed infants: mother eliminates all dairy from her own diet.
- In formula-fed infants: switch to appropriate alternative formula.
Alternative Formulas
| Formula Type | Use Case |
|---|---|
| Extensively Hydrolyzed Formula (eHF) | First choice for most CMPA; treats ≥90% of children; 2-8% may still react if IgE-mediated |
| Amino Acid Formula (AAF) / Elemental formula | Severe CMPA, anaphylaxis, eosinophilic disease, failure with eHF |
| Partially hydrolyzed formula | NOT suitable for treatment; may be used for prevention only |
| Soy formula | Caution - 30-40% of CMPA infants also develop soy allergy; avoid in <6 months |
| Goat's milk formula | Not recommended - significant cross-reactivity with cow's milk proteins (especially casein) |
| Plant-based (rice, oat, almond, etc.) | Not nutritionally adequate for infants; not recommended as primary formula substitutes |
Pharmacologic Treatment
- Oral cromolyn: may help some patients.
- Antihistamines: symptomatic relief for mild IgE-mediated reactions.
- Epinephrine (adrenaline) auto-injector: prescribed for patients at risk of anaphylaxis; must be immediately available.
Oral Immunotherapy (OIT) - Emerging
A 2025 systematic review and meta-analysis (Wang et al., Frontiers in Immunology; 19 RCTs, 815 participants) found:
- OIT significantly facilitates desensitization in children with CMA (RR 2.51, 95% CI: 1.54-4.09).
- Tolerance threshold at oral food challenge increased significantly (SMD 3.58).
- Cow milk sIgE and casein sIgE titers decreased after OIT.
- Risk of adverse reactions was not higher than controls.
- Caution: late complication of eosinophilic esophagitis has been reported; long-term efficacy needs more study. [PMID: 40534871]
9. Prognosis and Natural History
- Approximately 50% of children tolerate milk by age 1 year.
- ~80-85% outgrow it by age 3-5 years.
- IgE-mediated CMPA tends to persist longer than non-IgE-mediated.
- High casein sIgE titers and component sensitization predict persistence.
- Coexisting multiple food allergies or severe eczema predicts slower resolution.
- Rarely persists into adulthood.
10. Key Differential Diagnoses
| Condition | How to Differentiate |
|---|---|
| Lactose intolerance | Non-immune; no rash or systemic reaction; diagnosis with lactose breath test; resolves with lactase enzyme |
| Gastroesophageal reflux disease (GERD) | No immune mechanism; no skin/respiratory involvement |
| Sepsis / surgical emergency | Overlaps with FPIES; FPIES suggested by reproducible pattern with milk exposure |
| Eosinophilic esophagitis | Confirmed on biopsy (>15 eosinophils/high-power field); may coexist with CMPA |
| Celiac disease | Triggered by gluten (not milk protein); confirmed with serology + biopsy |
Summary
CMPA is a clinically heterogeneous immune-mediated allergy to one or more proteins in cow's milk, presenting across a spectrum from mild GI/skin symptoms to anaphylaxis. It is classified as IgE-mediated, non-IgE-mediated, or mixed. Diagnosis requires a structured approach combining clinical history, allergy testing where appropriate, elimination diet, and oral food challenge. Management centers on strict avoidance with appropriate formula substitution in infants, epinephrine access for anaphylaxis-risk patients, and consideration of oral immunotherapy in suitable candidates. The prognosis in children is generally favorable, with most outgrowing it by school age.
Sources: Goldman-Cecil Medicine (International Edition); Sleisenger & Fordtran's GI and Liver Disease; Tietz Textbook of Laboratory Medicine, 7th Ed.; K.J. Lee's Essential Otolaryngology; Wang et al., 2025 - OIT meta-analysis (PMID: 40534871); Malaysian Paediatric Association CMPA Guidelines 2024
This is a shared conversation. Sign in to Orris to start your own chat.