Course of arteries and nerves in internal auditory meatus
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is the complete answer:
Internal Auditory Meatus (Internal Auditory Canal) - Arteries and Nerves
Overview
The internal auditory meatus (IAM) is a short canal approximately 1 cm in length, lined with dura mater, running laterally from the cerebellopontine angle (CPA) into the petrous part of the temporal bone. It transmits the facial nerve (VII), vestibulocochlear nerve (VIII), internal auditory artery, and internal auditory vein.
The lateral end (fundus) is closed by a perforated bony plate. A horizontal shelf on the inner surface of this plate - the crista falciformis (transverse crest) - divides the fundus into upper and lower compartments. A vertical ridge called Bill's bar further subdivides the upper compartment.
Nerves in the IAM
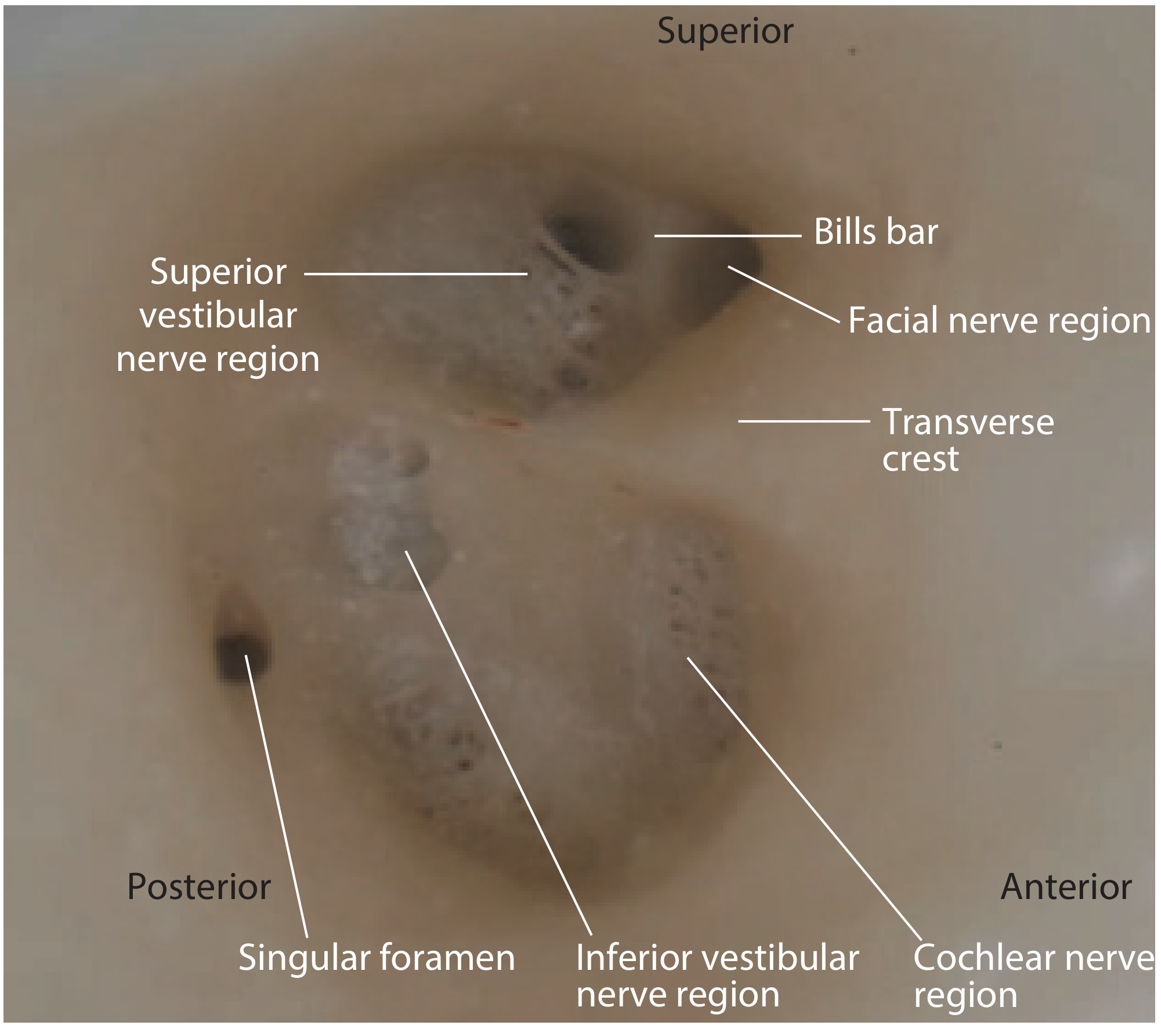
Endoscopic view of the left IAM apex showing: transverse crest, Bill's bar, facial nerve region, superior vestibular nerve region, inferior vestibular nerve region, cochlear nerve region, and the singular foramen.
1. Facial Nerve (CN VII)
- Emerges from the ventrolateral aspect of the lower pons, then travels laterally through the CPA together with CN VIII.
- On entering the meatus, the motor division lies on the superoanterior surface of the vestibulocochlear nerve (CVN). The nervus intermedius lies between the motor division and CN VIII.
- At the fundus, it occupies the anterosuperior quadrant, separated from the superior vestibular nerve region by Bill's bar.
- No major branches arise within the meatal segment.
- At the lateral end, it enters the facial (fallopian) canal to begin the labyrinthine segment - the narrowest and shortest segment - which runs anterolaterally to the geniculate ganglion.
2. Vestibulocochlear Nerve (CN VIII)
CN VIII occupies the inferior and posterior portions of the IAM and splits into cochlear and vestibular divisions at or near the fundus.
Above the transverse crest:
| Division | Location at fundus | Distribution |
|---|---|---|
| Facial nerve | Anterosuperior (separated by Bill's bar) | Facial muscles, parasympathetics, taste |
| Superior vestibular nerve | Posterosuperior (multiple foramina) | Superior + lateral semicircular canals, utricle, part of saccule |
Below the transverse crest:
| Division | Location at fundus | Distribution |
|---|---|---|
| Cochlear nerve | Anteroinferior (spiral foramina + central canal = cochlear area) | Organ of Corti |
| Inferior vestibular nerve | Posteroinferior (one or two foramina) | Saccule |
| Singular nerve | Foramen singulare (behind + below inferior vestibular foramen) | Posterior semicircular canal ampulla |
The singular nerve runs obliquely through the petrous bone close to the round window to supply the sensory epithelium of the posterior semicircular canal ampulla.
Arteries in the IAM
Internal Auditory Artery (Labyrinthine Artery)
- A branch of the anterior inferior cerebellar artery (AICA) in ~80% of cases; less commonly arises directly from the basilar artery.
- Enters the IAM alongside the facial and vestibulocochlear nerves.
- Gives a branch to CN VIII at the CPA before entering the meatus.
- Within the IAM it supplies ganglion cells, nerves, dura, and arachnoid, then splits into two main branches:
| Branch | Supplies |
|---|---|
| Anterior vestibular artery | Anterior and lateral semicircular canals, utricular macula |
| Common cochlear artery (splits further) | → Cochlear artery (cochlea proper) and posterior vestibular artery (posterior semicircular canal, saccular macula, part of cochlea) |
Because the labyrinthine artery is an end artery with no collateral supply, occlusion produces sudden sensorineural hearing loss and/or vertigo.
The labyrinthine artery also supplies the facial nerve in its cisternal, meatal, and labyrinthine segments (the more distal tympanic and mastoid segments are supplied by the petrosal branch of the middle meningeal artery and the stylomastoid artery from the posterior auricular artery).
Internal Auditory Vein
Drains the labyrinth and accompanies the artery, emptying into the inferior petrosal sinus or the sigmoid sinus.
Summary Diagram (Quadrant Map of the Fundus)
ANTERIOR POSTERIOR
─────────────────────────────
SUPERIOR │ Facial n. (VII) │ Superior vestibular n. │
│ │ (separated by Bill's bar)│
─────── Transverse crest (crista falciformis) ──
INFERIOR │ Cochlear n. │ Inferior vestibular n. │
│ │ (+ singular n. below) │
─────────────────────────────
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2 - "The internal auditory meatus"
- Localization in Clinical Neurology, 8e - "Anatomy of the Peripheral Course of the Facial Nerve"; "Meatal Segment"; blood supply of cochlea
- Cummings Otolaryngology Head and Neck Surgery - blood supply of the labyrinth
O Steiner redlich zone
ObSteiner redlich zone
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Excellent. I have comprehensive textbook material. Here is the full answer:
Obersteiner-Redlich Zone
Definition
The Obersteiner-Redlich (O-R) zone marks the morphological junction between the central nervous system (CNS) and the peripheral nervous system (PNS) along a nerve root or cranial nerve. It is the point where:
- Central myelin (produced by oligodendrocytes) ends
- Peripheral myelin (produced by Schwann cells) begins
The zone is named after Heinrich Obersteiner and Emil Redlich, who described it in the context of posterior nerve roots in the late 19th century.
Structural Basis
| Feature | CNS side (central to O-R zone) | PNS side (peripheral to O-R zone) |
|---|---|---|
| Myelinating cell | Oligodendrocyte | Schwann cell |
| One cell wraps | Multiple axons | One axon (if myelinated) |
| Connective tissue | Absent (only delicate arachnoid) | Endoneurium, perineurium, epineurium |
| Vulnerability | Less to trauma, more to demyelinating disease | More mechanically robust |
At the O-R zone itself, myelin is so thin that the fibers appear almost unmyelinated - creating a structurally weak transition point.
Location on Different Nerves
| Nerve | Location of O-R zone |
|---|---|
| Spinal nerve roots | Just past the emergence of the posterior root from the spinal cord |
| CN VII (Facial) | A few mm from the brainstem surface, within the cisternal/CPA segment; distinct from but near the root entry/exit zone (REZ) |
| CN VIII (Vestibulocochlear) | Within the internal auditory canal (IAC), near the fundus |
| CN V (Trigeminal) | Near the porus trigeminus (Gasserian ganglion region) |
For the facial nerve, both the REZ and the more distal O-R zone are surgical targets in microvascular decompression for hemifacial spasm.
Clinical Significance
1. Site of Vestibular Schwannoma Origin (Classical Teaching)
The classical teaching holds that vestibular schwannomas arise at the O-R zone of the vestibular nerve, where Schwann cells accumulate at the glial-Schwann junction. "Whorl-like" Schwann cell nests, eosinophilic bodies, and ganglion cells have been described here histologically (Prisig et al.), and these nests were proposed as forerunners of vestibular schwannomas.
However, this is now contested: imaging and surgical observations of early tumors show they more frequently originate near the fundus of the IAC, lateral to the O-R zone (i.e., in the more peripheral part of the IAC). The inferior vestibular nerve is now recognized as the predominant site of origin (up to 94% in some reports), not necessarily the O-R zone itself.
2. Hemifacial Spasm
Vascular compression of CN VII at or near the REZ/O-R zone (the transition between central and peripheral myelination) is the most common cause of hemifacial spasm. The central myelin at this region is less resistant to vascular pulsation, making it particularly vulnerable.
3. Demyelinating and Infectious Disease
The O-R zone in posterior spinal roots is a site of predilection for immunologic diseases - for example, the immune-mediated demyelination seen in the late stages of syphilis (tabes dorsalis) targets this thin-myelin transition zone.
4. Surgical Relevance
In CPA surgery (e.g., vestibular schwannoma removal via retrosigmoid approach), the CPA portion of CN VII and CN VIII is covered only by delicate arachnoid with no robust connective tissue sheath - rendering the nerves extremely vulnerable to surgical trauma and difficult to identify during tumor dissection.
Sources:
- THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System - "Obersteiner-Redlich zone in a posterior root"
- Scott-Brown's Otorhinolaryngology, Vol. 2 - "Intraparenchymal elements, organization and course" (facial nerve chapter)
- Shambaugh Surgery of the Ear - "Pathology" (vestibular schwannoma chapter)
- Localization in Clinical Neurology, 8e - "Peripheral nerve lesions and the cerebellopontine angle syndrome"; "Hemifacial spasm"
FISCH approach
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
I now have all the information needed for a comprehensive answer.
Fisch Infratemporal Fossa Approaches
Developed by Ugo Fisch, these are a structured series of postauricular lateral skull base approaches to the infratemporal fossa. They are classified into Types A, B, and C based on the region accessed, with Type D used separately for glomus tumor intracranial extension classification.
Overview of the Three Surgical Approaches
| Type | Primary Region Accessed | Key Structures Exposed |
|---|---|---|
| A | Jugular bulb, vertical petrous ICA, posterior infratemporal fossa | Jugular bulb, vertical ICA, sigmoid sinus, posterior fossa dura |
| B | Petrous apex, clivus, superior infratemporal fossa | Petrous ICA to foramen lacerum, middle cranial fossa floor, clivus |
| C | Nasopharynx, peritubal space, rostral clivus, parasellar region, pterygopalatine fossa, anterosuperior infratemporal fossa | Sphenoid sinus, cavernous sinus, foramen rotundum (V2), inferior orbital fissure |
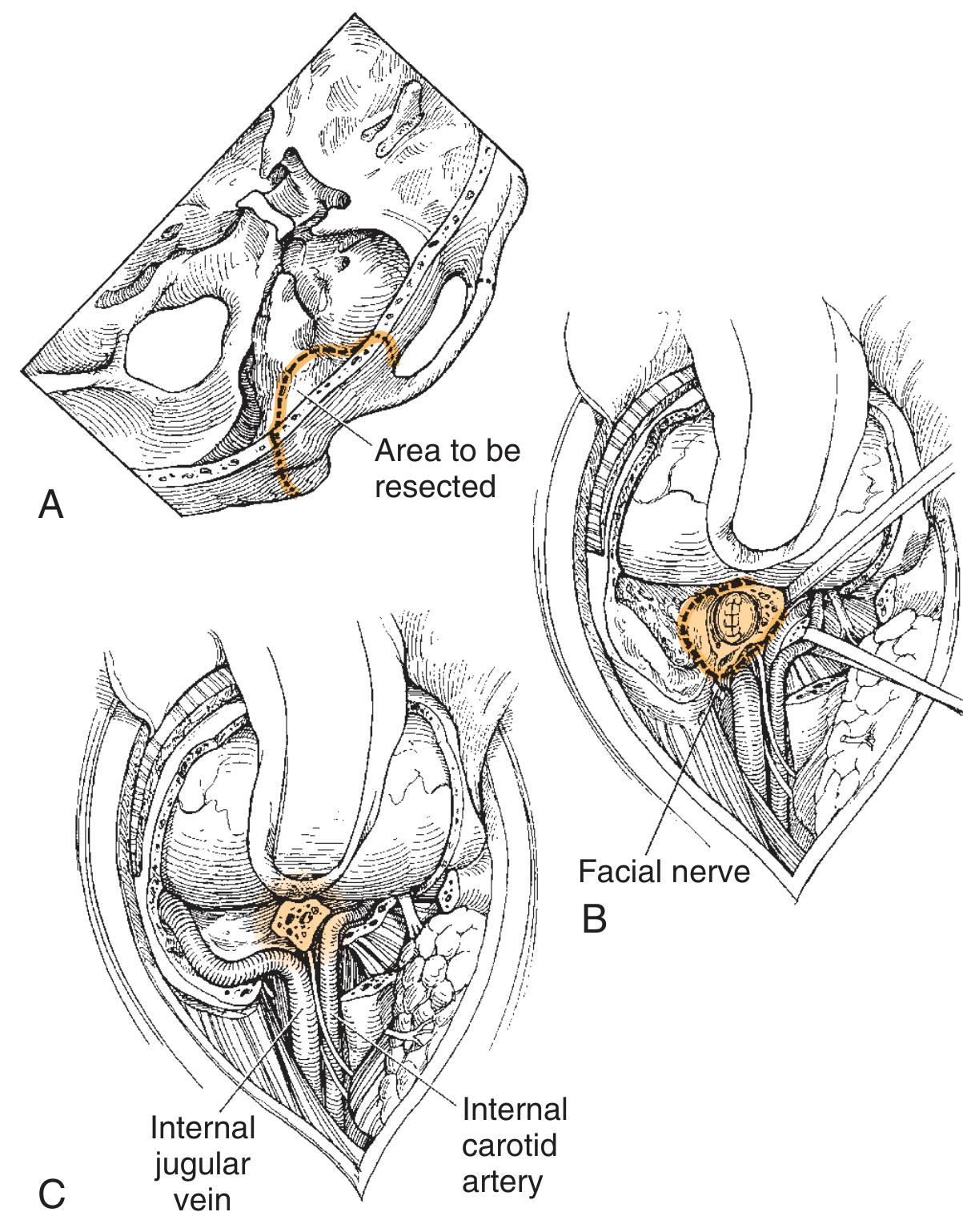
Fisch Type A Approach
Indications: Glomus jugulare (paraganglioma), jugular foramen schwannomas (intraforaminal/combination), petrous ICA lesions
Hallmark: Anterior transposition of the facial nerve - the defining and most distinguishing step
Surgical Steps:
- Incision: Large C-shaped postauricular incision extending anterosuperiorly into the temporal scalp and anteroinferiorly into the neck
- Flap elevation: Superficial to temporalis, SCM, and postauricular musculature
- Blind sac closure of EAC: Cartilaginous EAC transected; meatal skin everted and closed primarily; reinforced with anteriorly based mastoid periosteal flap. This prevents post-op CSF otorrhea and infection
- Middle ear entered: EAC skin + TM + malleus removed; incudostapedial joint separated; incus removed; tensor tympani tendon cut
- Radical mastoidectomy: Sigmoid sinus and jugular bulb skeletonized; middle and posterior fossa plates exposed
- Sigmoid sinus ligation: Below the mastoid emissary vein
- Cervical dissection: Internal jugular vein identified and controlled in the neck
- Anterior transposition of facial nerve (CN VII): Entire intratemporal course of facial nerve (from IAM porus to stylomastoid foramen) mobilized anteriorly. This is what distinguishes Type A and provides the wide inferior exposure
- Jugular bulb/ICA exposure: Bone over the jugular bulb and vertical petrous ICA removed; jugular bulb ligated; ICA skeletonized
- Tumor removal with full vascular control
- Closure: Abdominal fat obliteration; layered closure; pressure dressing
Key morbidity: High rate of permanent facial nerve weakness from anterior transposition - avoided if possible for schwannomas, but often necessary for large glomus jugulare
Fisch Type B Approach
Indications: Petrous apex lesions (cholesteatoma, chordoma, low-grade chondrosarcoma), clival tumors
Steps are identical to Type A up to the facial nerve, but anterior transposition is usually NOT required
Additional steps beyond Type A:
- Temporalis muscle reflected anteriorly (still attached to coronoid process and zygoma) to expose the superior infratemporal fossa
- Limits of exposure defined by: middle cranial fossa floor, mandibular condyle, reflected temporalis
- Middle meningeal artery and V3 (mandibular nerve) transected to expose the superior 4 cm of infratemporal fossa
- ICA uncovered from vertical segment to foramen lacerum by separating from soft tissue around the eustachian tube
- Petrous apex accessible with careful anterolateral ICA retraction; ICA can be elevated from foramen lacerum to canalis caroticus for temporary transposition
- For extensive benign lesions with nonserviceable hearing: transotic or transcochlear approach added (posterior transposition of facial nerve by cutting the GSPN and mobilizing CN VII from porus to stylomastoid foramen)
Fisch Type C Approach
Indications: Nasopharyngeal tumors (e.g., juvenile nasopharyngeal angiofibroma), parasellar tumors, clival chordomas, cavernous sinus lesions, tumors of pterygopalatine fossa
Type C = anterior extension of Type B
Additional steps:
- Pterygoid base removed - exposes V2 in foramen rotundum and inferior orbital fissure
- Uncovers the sphenoid sinus, which is entered
- Pterygoid process and lateral nasopharynx removed for nasopharyngeal exposure
- Provides access anterior to the foramen lacerum up to the posterior aspect of the maxillary sinus and nasopharynx
- Access to: rostral clivus, cavernous sinus, sphenoid sinus, peritubal space, pterygopalatine fossa, anterosuperior infratemporal fossa, nasopharynx
Fisch Classification of Glomus Tumors (Separate from Surgical Types)
Fisch also created a tumor staging system for glomus tumors (paragangliomas):
| Stage | Description |
|---|---|
| Type A | Limited to the middle ear cleft |
| Type B | Limited to tympanomastoid area; no infralabyrinthine involvement |
| Type C | Involves the infralabyrinthine compartment and petrous apex |
| - C1 | Limited involvement of carotid canal |
| - C2 | Invasion of vertical portion of carotid canal |
| - C3 | Invasion of horizontal portion; does not involve foramen lacerum |
| - C4 | Involves entire course of intrapetrous carotid |
| Type D | Intracranial extension |
| - De1 | Extradural, < 2 cm |
| - De2 | Extradural, > 2 cm |
| - Di1 | Intradural, < 2 cm |
| - Di2 | Intradural, > 2 cm |
| - Di3 | Intradural, unresectable |
Key Points Summary
- All three surgical approaches use a postauricular incision and blind sac EAC closure
- Type A = radical mastoidectomy + anterior facial nerve transposition + cervical dissection for jugular bulb/ICA control
- Type B = Type A steps (without facial transposition) + temporalis reflection + middle meningeal/V3 division for petrous apex/clivus
- Type C = Type B + pterygoid base removal for nasopharynx/parasellar access
- The facial nerve transposition in Type A carries significant risk of permanent facial palsy
- For jugular foramen schwannomas: Type A dissection is safest but facial transposition should be avoided if possible; the Fallopian bridge technique is an alternative to preserve the nerve
Sources:
- Cummings Otolaryngology Head and Neck Surgery - "Infratemporal Fossa Approaches"; "Fisch Type A Approach"; "Fisch Type B and C Approaches"
- K.J. Lee's Essential Otolaryngology - "Glomus Tumor Classification Schemes"
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2
Incisions in different types of FISCH approaches
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
I now have everything needed. Let me compile a focused, detailed answer specifically on the incisions used in each Fisch approach type.
Incisions in Fisch Infratemporal Fossa Approaches
Common to All Types: The Postauricular C-Shaped Incision
All three Fisch approaches share the same fundamental skin incision as their base - the large postauricular C-shaped incision. What differs between types is how far this incision is extended and what additional cuts (zygomatic arch division, pterygoid resection) are made to gain progressively more anterior access.
Fisch Type A - Incision
Primary incision: Large C-shaped postauricular incision
Course of incision:
- Begins in the temporal scalp (anterosuperiorly, above and in front of the auricle)
- Curves posteriorly behind the ear in a broad C
- Extends anteroinferiorly into the neck - the length in the neck varies depending on how much cervical and anterior exposure is needed
Additional soft tissue steps tied to the incision:
- Flap elevated superficial to the temporalis muscle, SCM, and postauricular musculature
- Dissection carried anteriorly over the parotid and into the neck in a subplatysmal plane
- Cartilaginous EAC is transected at the bony-cartilaginous junction - the meatal skin is everted and primarily closed (blind sac closure), reinforced by an anteriorly based mastoid periosteal flap
- Superficial parotidectomy performed as part of the exposure
- The pinna and skin flap are reflected anteriorly
Key feature: The incision and dissection extend into the neck to allow cervical vascular control (ICA, IJV, CN IX-XII) - this is the defining feature of the Type A incision compared to approaches that stay purely in the temporal region.
Fisch Type B - Incision
Primary incision: The same postauricular C-shaped incision as Type A
Additional extension:
- The incision is the same at the skin level, but the temporalis muscle is additionally reflected - remaining attached to the coronoid process and the zygoma - and swung inferiorly as a hinged flap. This muscular reflection (not a separate skin incision) exposes the superior infratemporal fossa
- The zygomatic arch may be divided anteriorly and posteriorly and reflected inferiorly attached to masseter (as described by Scott-Brown's) to gain access to the superolateral quadrant of the infratemporal fossa
- Facial nerve transposition is usually NOT required (unlike Type A)
- The limits of exposure are defined by: middle cranial fossa floor, mandibular condyle, and reflected temporalis muscle
- Middle meningeal artery and V3 (mandibular nerve) are transected to open the superior 4 cm of the infratemporal fossa
Distinction from Type A: No routine cervical extension for jugular/ICA control; the exposure is directed superiorly toward the petrous apex and clivus rather than inferiorly toward the jugular bulb.
Fisch Type C - Incision
Primary incision: The same postauricular C-shaped incision as Types A and B - Type C is simply an anterior extension of Type B
Additional maneuvers beyond Type B:
- Zygomatic arch divided anterior to the TMJ and just behind the orbital rim (without damaging the frontal branch of CN VII), then reflected inferiorly attached to the masseter muscle
- The temporalis muscle and fascia are elevated from the temporal fossa and reflected inferiorly
- Pterygoid process removed (both lateral and medial plates) - this is the key bony step unique to Type C, exposing:
- V2 in the foramen rotundum
- Inferior orbital fissure
- Sphenoid sinus (entered)
- Dissection along the eustachian tube with access to anterior third and nasopharynx
- Nasopharyngeal mucosa incised (pharyngobasilar membrane) to enter the nasopharyngeal cavity
Complications specific to Type C incision/approach:
- Temporary frontal facial paresis in ~30% (from frontal branch manipulation during zygomatic arch exposure)
- Hypoaesthesia of lower half of face and ipsilateral tongue (V3 is sacrificed)
- Temporary post-operative trismus and malocclusion (from temporalis and masseter displacement)
- Permanent conductive hearing loss
Summary Table
| Feature | Type A | Type B | Type C |
|---|---|---|---|
| Base incision | Postauricular C-shaped | Same as A | Same as A & B |
| Superior extent | Into temporal scalp | Into temporal scalp | Into temporal scalp |
| Inferior extent | Into the neck (cervical) | Less neck exposure | Less neck exposure |
| EAC | Blind sac closure | Blind sac closure | Blind sac closure |
| Zygomatic arch | Not routinely divided | Divided + reflected | Divided + reflected |
| Temporalis | Reflected | Reflected inferiorly | Reflected inferiorly |
| Facial nerve | Anteriorly transposed (defining step) | Usually preserved | Usually preserved |
| Pterygoid removal | No | No | Yes (unique to Type C) |
| Nasopharynx entered | No | No | Yes |
| Cervical dissection | Yes (ICA, IJV, CN IX-XII) | Limited | Limited |
Sources:
- Cummings Otolaryngology Head and Neck Surgery - "Fisch Type A Approach"; "Fisch Type B and C Approaches"
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2 - "Procedure" (infratemporal fossa approach chapter)
- K.J. Lee's Essential Otolaryngology - "Surgery of the Infratemporal Fossa"
Give about CT angiography and its correlation in ENT practice
Finding Sources
Finding Sources
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.