Neck of femur fracture
Reading File
Finding Sources
Finding Sources
Searching PubMed
"femoral neck fracture" AND management
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Loading Image
I now have rich content from multiple authoritative sources. Let me compile the comprehensive answer.
Fracture of the Neck of Femur (NOF Fracture / Hip Fracture)
Anatomy & Why It Matters
The femoral neck is the segment between the femoral head and the trochanters. Its relationship to the hip joint capsule is the single most important anatomical factor in management.
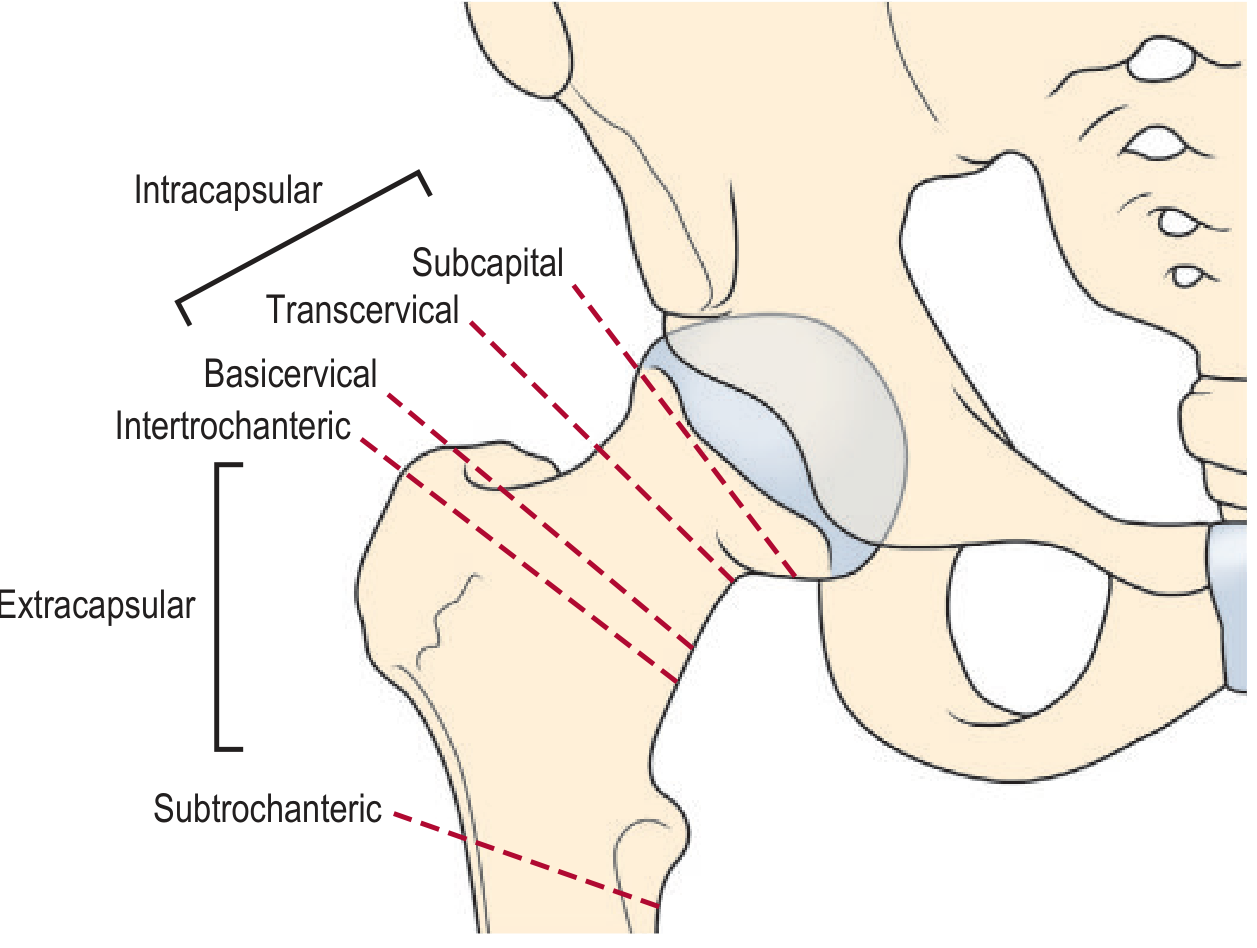
Intracapsular fractures (subcapital, transcervical, basicervical) lie within the capsule. The blood supply to the femoral head runs in retinacular fibres closely applied to the neck; a displaced intracapsular fracture disrupts these vessels and risks avascular necrosis (AVN) of the femoral head (incidence 15–35%).
Extracapsular fractures (intertrochanteric, subtrochanteric) lie outside the capsule; the retinacular blood supply is preserved and AVN is rare.
In elderly patients, the medullary blood supply is already attenuated due to fatty marrow replacement, and the artery within the ligamentum teres is often atherosclerotic — leaving the retinacular vessels as the sole supply, which is why displaced fractures almost inevitably cause AVN in this age group. - Gray's Anatomy for Students, p. 784
Epidemiology & Risk Factors
- Most common in elderly osteoporotic women (post-menopausal)
- Typically low-energy falls at home; the fracture often completes itself (stress fracture → fall, not fall → fracture)
- Younger patients require high-energy trauma
- Associated conditions: osteoporosis, Paget disease, metastases
Clinical Presentation
| Feature | Finding |
|---|---|
| Pain | Severe groin/hip pain; inability to weight-bear |
| Deformity | Shortened and externally rotated leg |
| Mechanism | Psoas major inserts on lesser trochanter → when neck is detached, pulls femur proximally and into ER; adductor spasm worsens ER |
| Occult fracture | May walk with groin pain aggravated by weight-bearing |
Classification — Garden (Intracapsular)
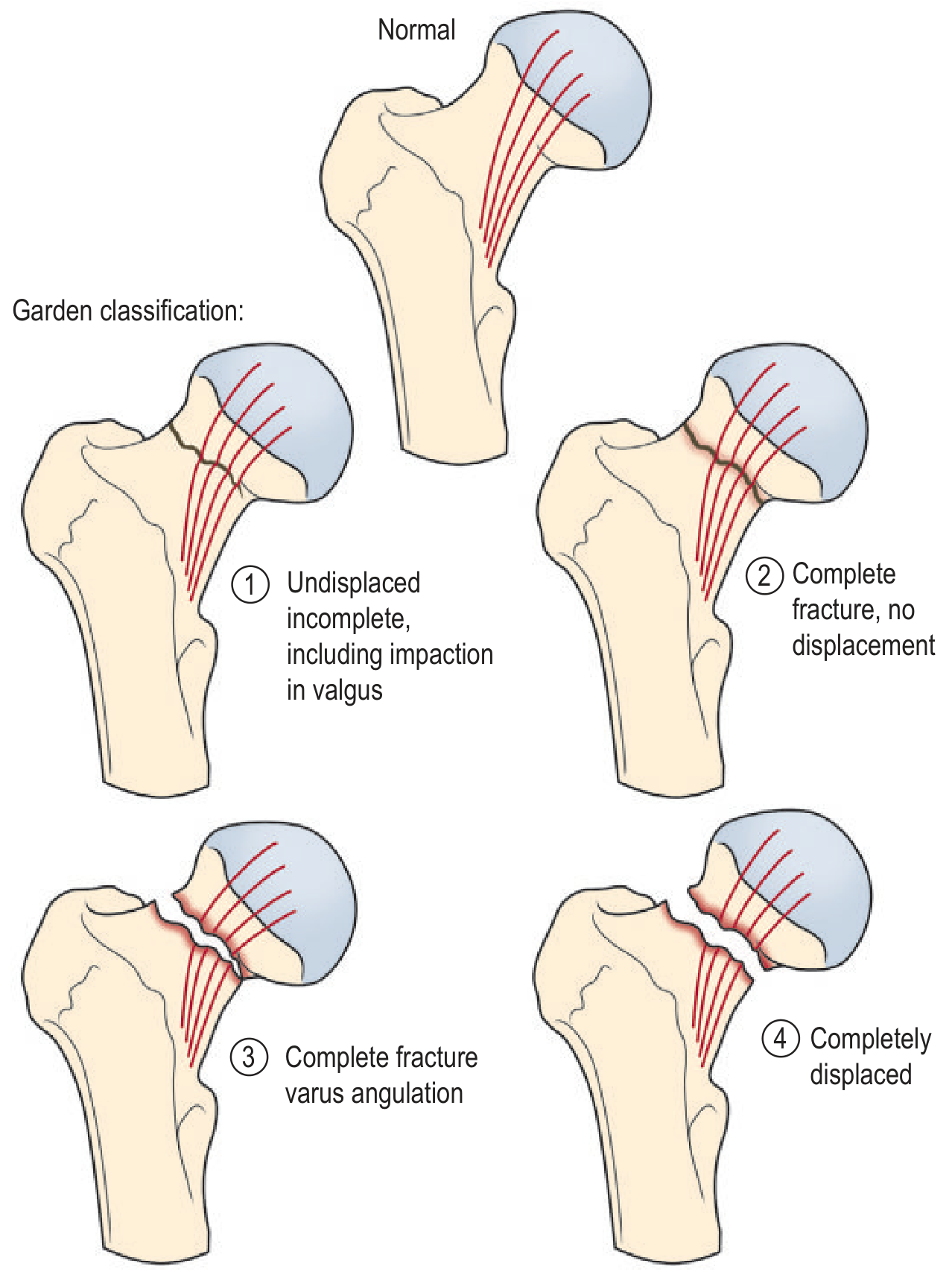
| Garden | Description | Displacement | AVN Risk |
|---|---|---|---|
| I | Incomplete / valgus impacted | Undisplaced | Low |
| II | Complete, no displacement | Undisplaced | Low |
| III | Complete, varus angulation | Displaced | High |
| IV | Completely displaced | Displaced | Highest |
Clinically, undisplaced = Garden I & II (stable, preserve head); displaced = Garden III & IV (arthroplasty favoured). - Grainger & Allison's Diagnostic Radiology, p. 1162
Imaging

- Plain AP pelvis + true lateral hip — first-line; ~15% of fractures missed on AP alone
- Look for: break in trabecular lines, sclerotic line (impacted), varus tilt
- MRI — gold standard for occult fractures; more sensitive/specific than bone scan or CT
- CT — useful when MRI unavailable
Management
Intracapsular Fractures
| Patient Group | Fracture Type | Preferred Treatment |
|---|---|---|
| Elderly (>60–65) — displaced (Garden III/IV) | Intracapsular | Hemiarthroplasty (cemented or uncemented) |
| Active, independently mobile elderly — displaced | Intracapsular | Total hip replacement (THR) |
| Young patient (<60) or undisplaced (Garden I/II) | Intracapsular | Internal fixation — dynamic hip screw (DHS) or multiple cannulated screws |
| Athletes with stress fracture | Intracapsular | Non-weight-bearing (walker) ± surgical fixation if tension-type |
Hemiarthroplasty: Femoral head removed; femoral neck trimmed to trochanters; medullary cavity reamed; metal prosthesis inserted; head articulates with native acetabulum. Acetabulum is not replaced in straightforward cases. - Gray's Anatomy for Students, p. 784
THR vs Hemiarthroplasty: Recent evidence (2025 meta-analysis, PMID 41303766) confirms higher thromboembolic risk with THR vs hemiarthroplasty — a key peri-operative consideration.
Extracapsular Fractures
- Intertrochanteric/subtrochanteric: internal fixation (DHS, intramedullary nail); AVN not a concern
Complications
| Complication | Notes |
|---|---|
| Avascular necrosis | 15–35% displaced intracapsular; even if prosthesis placed, residual native head fragments must be monitored |
| Non-union | Higher risk with displaced fractures treated with fixation |
| DVT/PE | Significant risk; prophylaxis mandatory (LMWH ± mechanical) |
| Infection | Prosthetic joint infection |
| Leg length discrepancy | Post-operative |
| Mortality | ~30% 1-year mortality in elderly — largely driven by pre-existing comorbidities |
Stress Fractures (Athletes)
- Anterior groin pain, worse with weight-bearing; night pain if delayed
- Compression-type (inferior medial neck) — more stable, conservative management acceptable
- Tension-type (superior lateral neck) — unstable, prone to displace → surgical referral
- Conservative: restricted weight-bearing × 6 weeks, serial X-rays every 1–2 weeks
- Return to running only after pain-free walking ≥1 mile - Pfenninger & Fowler's Procedures for Primary Care, p. 1312
Pre-op Workup in Elderly
- Full medical workup mandatory — cardiac, respiratory, renal, metabolic
- Optimise for surgery urgently (aim within 36–48 h of admission)
- Treat coexisting osteoporosis (bisphosphonates, calcium/Vit D post-operatively)
- VTE prophylaxis
Recent Evidence (2024–2025)
- PMID 39436746 (2024, Systematic Review): Supercapsular percutaneously assisted THA vs standard posterior approach for NOF fracture in elderly — comparable outcomes with minimally invasive technique
- PMID 41303766 (2025, Systematic Review): THR carries higher thromboembolic risk vs hemiarthroplasty — relevant when choosing arthroplasty type
- PMID 39581960 (2024, Meta-Analysis): Global AVN incidence after femoral neck fracture surgery in adolescents — highlights the high-stakes nature of preserving the head in young patients
Sources: Gray's Anatomy for Students (p. 784); Grainger & Allison's Diagnostic Radiology (p. 1162); Pfenninger & Fowler's Procedures for Primary Care (p. 1312); Rockwood & Green's Fractures in Adults, 10th ed. (2025)
This is a shared conversation. Sign in to Orris to start your own chat.