


IMG-20260617-WA0003.jpg
+2 more
Explain the given x ray in detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
I have enough background from the library references and my own knowledge to give a thorough analysis. Let me now deliver the full detailed X-ray explanation based on the three images provided.
Detailed X-Ray Analysis
Disclaimer: This analysis is for educational purposes. A formal radiological report must be issued by a licensed radiologist in a clinical context.
IMAGE 1 - Skull PA (Frontal) + Skull Lateral
Patient: Muntasir Musalman, 30Y M | Date: 05/03/2025 | Institution: B & C Teaching Hospital
View 1A - PA (Postero-Anterior) Skull
Calvarium (Skull Vault):
- The outer and inner tables of the skull appear intact with no visible discontinuity or step-off suggesting a fracture.
- Diploic space (cancellous bone between inner and outer tables) appears normal in density.
- No obvious lytic or sclerotic lesions are identified.
- Coronal and sagittal sutures are visible and appear within normal limits for a 30-year-old (should be largely fused/closed at this age).
Facial Skeleton:
- Bilateral orbital rims appear symmetric and intact.
- Nasal bones are visible; no obvious deviation.
- Maxillary sinuses: appear relatively clear (no obvious opacification or air-fluid levels).
- Mandible is visible and appears intact.
- Dentition is present with no obvious missing teeth on this view.
Sella Turcica: On PA view, the posterior clinoid processes and dorsum sellae are faintly projected - no gross enlargement appreciated.
Pineal gland: No calcification is clearly visible in this view (mild calcification at midline is a normal incidental finding in adults).
Symmetry: The skull appears symmetric without lateral shift of midline structures.
View 1B - Skull Lateral (Right side, from same film)
Calvarium:
- The outer table, diploic space, and inner table are visible - no obvious step-off or linear lucency consistent with a fracture.
- Vascular markings (middle meningeal artery grooves) are visible as fine branching radiolucent lines within the calvarium - this is normal.
- No abnormal vascular channels or widening noted.
Sella Turcica:
- Visible in the lateral view. The floor, anterior and posterior clinoid processes are identifiable.
- No obvious ballooning, erosion, or "double floor" sign (which would suggest a pituitary mass).
- Normal-sized sella for a 30-year-old male.
Facial bones:
- Frontal sinus: visible as a radiolucent area above the nasal bridge - appears pneumatized normally.
- Sphenoid sinus: visible posteriorly - appears clear.
- Nasal bones and hard palate are visible.
- Mandible and dentition: mandibular condyle, ramus, and body visible. Upper and lower teeth are present and aligned.
Cervical Spine (visible on lateral skull view):
- C1-C5 levels are partially visible.
- Vertebral bodies appear normally aligned.
- No gross anterior wedging or listhesis visible on this view.
- Prevertebral soft tissue shadow appears within normal limits (no widening).
Overall Impression - X-ray 1: No acute fracture, no obvious intracranial calcification, no sinus opacification, no sella abnormality. Appears within normal limits for a 30-year-old.
IMAGE 2 - Skull Lateral (Left side)
Patient: DRTG DTRGDYG (likely a test/demo patient label) | Date: 10/12/2025 | Institution: B & C Teaching Hospital | Scale bar: 4 cm
This is a dedicated left-lateral skull X-ray with better detail.
Calvarium:
- The calvarium is well-corticated with intact inner and outer tables.
- Diploic space is normal.
- No linear lucencies, step-off deformities, or depressed fractures.
- Normal vascular channel impressions are present.
- Coronal suture: faintly visible anteriorly - normal in appearance.
Sella Turcica:
- Well-defined floor and posterior wall (dorsum sellae).
- No erosion of the dorsum. No double floor.
- Normal sella size - consistent with a normal pituitary.
Frontal / Sphenoid / Ethmoid Sinuses:
- Frontal sinus is clearly pneumatized - appears clear (dark/lucent) - no opacification.
- Sphenoid sinus (posteriorly) also appears clear.
Calvarium thickness: Appears normal and uniform.
Temporomandibular Joint (TMJ):
- Mandibular condyle is visible articulating in the glenoid fossa.
- No obvious joint space narrowing or condylar erosion.
Dentition:
- Upper and lower molar teeth visible and appear present.
- Jaw is slightly open (mouth-open position for this view).
Cervical spine:
- C1 through approximately C6-7 are visible.
- Vertebral body heights appear preserved.
- Cervical lordosis is present (normal gentle anterior curve).
- Disc spaces appear maintained.
- No gross osteophytes or listhesis visible at this resolution.
Overall Impression - X-ray 2: Normal lateral skull X-ray. No fracture, no sella pathology, no sinus disease. Cervical spine appears intact with preserved lordosis.
IMAGE 3 - Cervical Spine AP + Lateral
Patient: Birendra Kumar Khadka, 80Y M | Date: 03/23/2025 | Institution: B & C Teaching Hospital | Scale bar: 8 cm
This is the most clinically significant set of images. The patient is an 80-year-old male - age is critical for interpretation.
View 3A - Cervical Spine AP (Antero-Posterior)
Vertebral alignment:
- The vertebral bodies from C3 to C7 are visible in the AP view, appearing in a vertical column.
- No gross lateral scoliotic curvature.
Vertebral bodies:
- Mild loss of height is possible at one or more levels - difficult to confirm precisely, but the disc spaces appear somewhat narrowed at multiple levels (most apparent in the lower cervical region), consistent with degenerative disc disease (spondylosis) in an 80-year-old.
- Endplate sclerosis (increased density at the upper and lower margins of vertebral bodies) may be present - a feature of degenerative change.
Uncinate processes (uncovertebral joints):
- In an elderly patient, these are often enlarged/osteophytic, visible as lateral bony projections on AP view. This appears to be present here.
Spinous processes:
- Midline alignment of spinous processes appears maintained (no rotational malalignment).
Paraspinal soft tissues:
- No gross widening of prevertebral soft tissues visible on this view.
Upper chest/lower neck (visible):
- Bilateral clavicles visible. No gross bony lesion.
- Upper ribs and lung apices visible - no obvious consolidation or mass.
View 3B - Cervical Spine Lateral
This is the most informative view for an 80-year-old.
Alignment - Cervical Lordosis:
- The normal cervical spine should have a gentle anterior concave curve (lordosis).
- On this film, the lordosis appears reduced or straightened - this is common in degenerative cervical disease and muscle spasm.
Vertebral Bodies (C2-C7 clearly visible):
- Anterior osteophytes are clearly visible - bony projections from the anterior margins of multiple vertebral bodies. These are characteristic of cervical spondylosis (degenerative osteoarthritis).
- The osteophytes are most prominent at multiple levels (C4-C5, C5-C6, C6-C7 appear most affected).
- This "lipping" or "beaking" pattern at multiple levels is typical of multi-level cervical spondylosis.
Disc Spaces:
- Multiple disc spaces appear narrowed compared to expected normal height - most evident at C5-C6 and C6-C7.
- Disc space narrowing + osteophytes = classic degenerative disc disease.
Posterior elements:
- Facet joint degeneration may be contributing to foraminal narrowing (cannot be fully assessed on plain films).
Posterior osteophytes (of clinical importance):
- If posterior osteophytes encroach on the spinal canal, this can cause cervical myelopathy or radiculopathy. These are suspected but require MRI to confirm cord/nerve root compression.
Prevertebral soft tissue:
- The prevertebral soft tissue shadow anterior to the vertebral bodies appears within acceptable limits at upper levels (C2-C3 should be <7 mm; C6-C7 <22 mm). No significant widening suggesting abscess or hematoma.
Atlantoaxial region (C1-C2):
- The odontoid process (dens) is visible. No obvious fracture or atlantoaxial subluxation.
- In elderly patients, dens fractures and C1-C2 instability are important - appears grossly intact here.
Overall Impression - X-ray 3: Multi-level cervical spondylosis with:
- Reduced cervical lordosis
- Multiple anterior osteophytes at C4 through C7
- Disc space narrowing at multiple levels (most prominent C5-C6, C6-C7)
- Findings consistent with advanced degenerative cervical spine disease expected in an 80-year-old
- No acute fracture or gross malalignment visible
- MRI of cervical spine would be warranted if the patient has symptoms of myelopathy (gait disturbance, hand clumsiness) or radiculopathy (arm pain, numbness, weakness)
Summary Table
| X-ray | Patient | Age | Key Finding | Impression |
|---|---|---|---|---|
| Skull PA + Lateral (Film 1) | Muntasir Musalman | 30M | No fracture, normal sella, clear sinuses | Normal skull X-ray |
| Skull Lateral (Film 2) | Demo patient | - | Normal calvarium, normal sella, preserved lordosis | Normal skull X-ray |
| C-spine AP + Lateral (Film 3) | Birendra Kumar Khadka | 80M | Multi-level osteophytes, disc narrowing, reduced lordosis | Multi-level cervical spondylosis |
Clinical note: Plain X-rays of the skull are limited in detecting soft tissue pathology (brain, meninges, discs, nerve roots). CT is preferred for acute trauma; MRI is the gold standard for assessing the spinal cord, discs, and nerve roots. These films should always be correlated with the patient's clinical presentation by the treating physician.
Sphenoid bone
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Here is a comprehensive account of the sphenoid bone, drawn from Gray's Anatomy for Students and Scott-Brown's Otorhinolaryngology.
The Sphenoid Bone
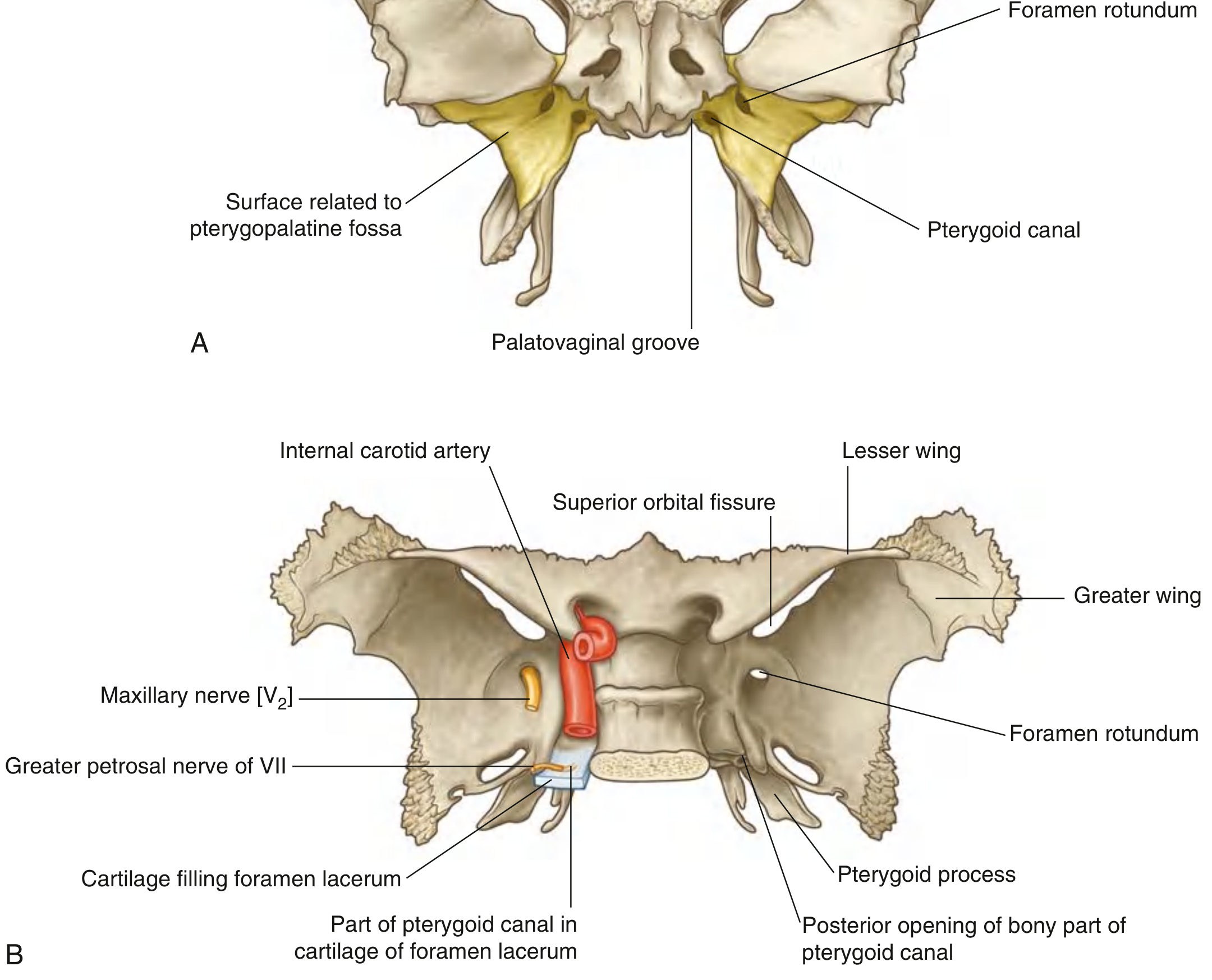
Sphenoid bone: (A) Anterior view showing pterygopalatine fossa relations; (B) Posterosuperior view showing wings, foramina, and key neurovascular structures - Gray's Anatomy for Students
Overview
The sphenoid is a single, unpaired, butterfly-shaped bone that sits centrally at the base of the skull. It articulates with all other cranial bones, making it the keystone of the cranial base. It is divided into:
- Body (central)
- Lesser wings (2) - project anterosuperiorly
- Greater wings (2) - project posterolaterally
- Pterygoid processes (2) - descend inferiorly
1. Body
The body is the central cube-shaped portion. Key features:
- Superior surface - hollowed to form the sella turcica ("Turkish saddle"), which houses the pituitary gland. It is roofed by the diaphragma sellae (fibrous dura). The anterior and posterior clinoid processes border the sella.
- Cavernous sinuses lie on either side of the body, grooving its lateral surfaces.
- Inferior surface - forms the roof of the postnasal space (nasopharynx).
- Sphenoid sinuses are contained within the body - paired, pneumatized air spaces with significant clinical relevance (sinusitis, transsphenoidal pituitary surgery).
2. Lesser Wings
- Extend anterosuperiorly from the body as two flat, triangular plates.
- Optic canal perforates the base of each lesser wing, transmitting the optic nerve (CN II) and ophthalmic artery.
- The sharp posterior edge of the lesser wing forms the posterior boundary of the anterior cranial fossa.
- The gap between the lesser and greater wings forms the superior orbital fissure (see below).
3. Greater Wings
The greater wings project laterally and superiorly from the body and have multiple surfaces:
| Surface | Forms |
|---|---|
| Cerebral (superior) | Floor of the middle cranial fossa |
| Orbital (anterior) | Posterior wall of the orbit |
| Temporal (lateral) | Medial wall of the temporal fossa |
| Infratemporal (inferior) | Roof of the infratemporal fossa |
Articulations of the greater wing:
- Anteriorly - frontal bone
- Laterally - zygomatic bone
- Posteriorly - petrous temporal bone
The angular boundary between the temporal and infratemporal surfaces is the infratemporal crest.
Key foramina in the greater wing (from anterior to posterior):
| Foramen | Transmits |
|---|---|
| Foramen rotundum | Maxillary nerve (CN V2) → pterygopalatine fossa |
| Foramen ovale | Mandibular nerve (CN V3) + lesser petrosal nerve → infratemporal fossa |
| Foramen spinosum | Middle meningeal artery + meningeal branch of V3 |
| Sphenoidal emissary foramina | Emissary veins connecting cavernous sinus to pterygoid plexus |
Projecting inferiorly just medial to the foramen spinosum is the spine of the sphenoid, which is the cranial attachment of the sphenomandibular ligament.
4. Superior Orbital Fissure
Formed between the lesser wing (above) and greater wing (below), this oblique fissure transmits:
- CN III (oculomotor)
- CN IV (trochlear)
- CN V1 (ophthalmic division of trigeminal, and its branches: lacrimal, frontal, nasociliary)
- CN VI (abducent)
- Ophthalmic veins
Clinically, a lesion here causes a superior orbital fissure syndrome (ophthalmoplegia + loss of corneal reflex + proptosis).
5. Pterygoid Processes
Each pterygoid process descends vertically from the junction of the body and greater wing, splitting into two plates:
Medial pterygoid plate
- Forms the posterior wall of the nasal cavity.
- Inferiorly ends as the pterygoid hamulus - a hook-like projection around which the tendon of tensor veli palatini curves (acts as a pulley).
- The scaphoid fossa at its root is the attachment for tensor veli palatini.
- The cartilaginous Eustachian tube grooves its posterior border superiorly.
- The pterygomandibular raphe attaches at its lower end.
Lateral pterygoid plate
- Projects posterolaterally into the infratemporal fossa.
- Lateral surface: attachment for the lower head of lateral pterygoid muscle.
- Medial surface: attachment for the deep head of medial pterygoid muscle.
- Both muscles are involved in jaw protrusion and opening.
6. Pterygoid Canal (Vidian Canal)
A horizontal bony canal running through the root of the pterygoid process. It transmits the nerve of the pterygoid canal (Vidian nerve), which carries:
- Preganglionic parasympathetic fibers from the greater petrosal nerve (from CN VII)
- Postganglionic sympathetic fibers from the deep petrosal nerve (carotid plexus)
These fibers synapse in the pterygopalatine ganglion inside the pterygopalatine fossa.
7. Clinical Correlates
| Condition | Sphenoid structure involved |
|---|---|
| Pituitary adenoma | Expands sella turcica, erodes clinoid processes or dorsum sellae |
| Transsphenoidal surgery | Surgical access to pituitary via sphenoid sinus |
| Sphenoid sinusitis | Can spread to cavernous sinus → cavernous sinus thrombosis |
| Middle meningeal artery rupture | Fracture of pterion (where greater wing meets temporal/parietal/frontal bones) |
| CN V2/V3 lesions | Foramina rotundum/ovale involvement (tumors, fractures) |
| Superior orbital fissure syndrome | Orbital apex fracture or tumor affecting all structures traversing it |
| Carotid-cavernous fistula | Abnormal connection between ICA and cavernous sinus adjacent to sphenoid body |
Summary
The sphenoid bone is the anatomical hub of the skull base. Its body houses the pituitary fossa and sphenoid sinus; its lesser wings carry the optic canals; its greater wings form critical cranial fossa floors and carry the key foramina (rotundum, ovale, spinosum); and its pterygoid processes anchor the muscles of mastication and palate. Its central location means that fractures, tumors, or infections involving the sphenoid can affect nearly every major cranial nerve and vascular structure at the skull base.
- Gray's Anatomy for Students, pp. 1114, 1133
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 2, pp. related to lateral skull base
This is a shared conversation. Sign in to Orris to start your own chat.