Tetracycline
Reading File
Finding Sources
Searching PubMed
"tetracycline" AND "clinical use"
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive data. Here is the full reference answer:
Tetracyclines
Chemical Structure & Classification
Tetracyclines are a family of antibiotics built around a four-ring (naphthacene) core with various substituents that distinguish individual members. Members in clinical use include:
| Drug | Route | Half-life | Dosing | Notes |
|---|---|---|---|---|
| Tetracycline | Oral | ~8 h | Every 6 h | Prototype; renal elimination |
| Doxycycline | Oral/IV | ~18 h | Every 12 h | Nonrenal; minimal food interaction |
| Minocycline | Oral/IV | ~16 h | Every 12 h | Vestibular toxicity; hepatic metabolism |
| Tigecycline | IV | ~42 h | q12h (50 mg) | Glycylcycline; overcomes resistance |
| Eravacycline | IV | - | q12h (1 mg/kg) | Fluorocycline; broadest gram-negative coverage |
| Omadacycline | Oral/IV | - | Once daily | Aminomethylcycline; empty stomach required |
Mechanism of Action
Tetracyclines inhibit bacterial protein synthesis by binding reversibly to the 30S ribosomal subunit, blocking the A (acceptor) site and preventing aminoacyl-tRNA from docking on the mRNA-ribosome complex. The result is arrest of peptide chain elongation.
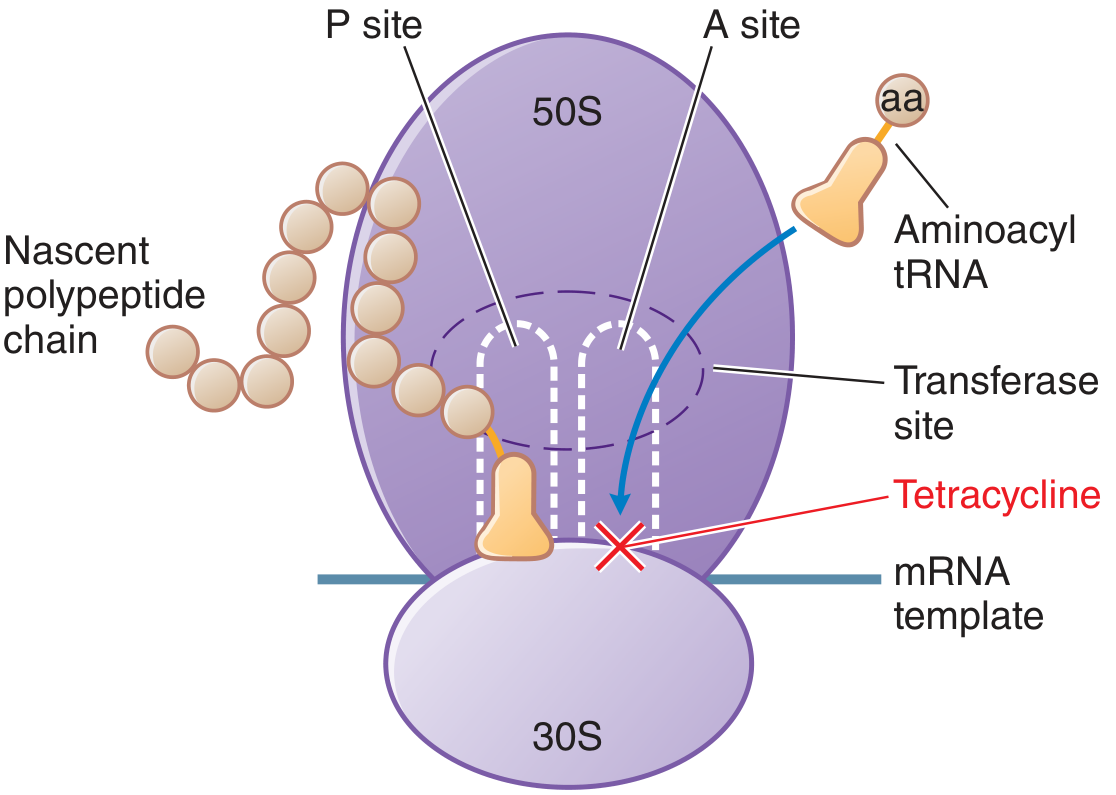
Figure: Tetracyclines bind the 30S subunit and block tRNA binding to the A site, halting protein synthesis (Goodman & Gilman's)
Entry into gram-negative bacteria occurs via passive diffusion through porin channels in the outer membrane and by active transport across the cytoplasmic membrane.
Effect: Bacteriostatic (bactericidal in high doses/specific organisms)
Antimicrobial Spectrum
Tetracyclines are intrinsically more active against gram-positives than gram-negatives (gram-negatives efflux them more effectively):
- Gram-positive: S. pyogenes, S. pneumoniae (PCN-sensitive), MSSA, MRSA (doxycycline/minocycline)
- Gram-negative: H. influenzae, Vibrio cholerae, V. vulnificus, Campylobacter, H. pylori, Yersinia pestis, Francisella tularensis, Brucella spp., Pasteurella multocida; intrinsic resistance in Pseudomonas, Proteus
- Atypicals: Mycoplasma pneumoniae, Chlamydia spp., Legionella spp., Ureaplasma, Coxiella burnetii
- Rickettsiae: Rickettsia, Ehrlichia, Anaplasma
- Spirochetes: Borrelia burgdorferi (Lyme), Treponema pallidum (syphilis), Borrelia recurrentis
- Other: Plasmodium spp., Bacillus anthracis, nontuberculous mycobacteria (M. marinum)
Clinical Indications
First-line uses
- Chlamydia, lymphogranuloma venereum, granuloma inguinale
- Rickettsial diseases (Rocky Mountain spotted fever, ehrlichiosis)
- Lyme disease (Borrelia infections)
- Community-acquired pneumonia (doxycycline, outpatient)
- Tularemia (mild to moderate), plague (Yersinia pestis), brucellosis
- Purulent skin/soft-tissue infections and MRSA SSTIs
- Acne vulgaris
- H. pylori eradication (tetracycline + bismuth + metronidazole + PPI)
- Malaria prophylaxis and treatment (doxycycline with quinine for chloroquine-resistant strains)
- M. marinum infections
Alternative/second-line uses
- Syphilis (penicillin-allergic patients)
- Anthrax, actinomycosis, animal bites (Pasteurella)
- Cholera, Nocardia (minocycline + sulfonamide)
- SIADH (demeclocycline - exploits nephrogenic DI side effect)
(Fitzpatrick's Dermatology; Goodman & Gilman's; Goldman-Cecil Medicine)
Pharmacokinetics
- Oral absorption: Tetracycline ~60-70%; doxycycline ~93% (less affected by food/cations than others)
- Chelation: All oral tetracyclines are chelated by divalent/trivalent cations (Ca²⁺, Mg²⁺, Al³⁺, Fe²⁺) - avoid dairy, antacids, iron supplements (space by 2-4 h)
- Distribution: Wide; crosses placenta; concentrates in liver, bone, teeth
- Elimination:
- Tetracycline, demeclocycline: primarily renal - dose-adjust in renal failure
- Doxycycline, omadacycline: biliary + renal (no dose adjustment in renal failure)
- Minocycline: extensively hepatically metabolized
- Tigecycline, eravacycline: mostly excreted unchanged; dose-adjust in severe hepatic impairment
(Katzung's Basic & Clinical Pharmacology, 16e; Goodman & Gilman's)
Resistance Mechanisms
Three mechanisms (frequently plasmid-mediated, often inducible):
-
Active efflux pumps - the most common; Tet(A-E) in gram-negatives efflux tetracycline, doxycycline, minocycline; Tet(K) in staphylococci effluxes tetracycline only. Tigecycline, eravacycline, omadacycline are NOT substrates for most efflux pumps.
-
Ribosomal protection proteins - Tet(M) binds the tetracycline-ribosome complex and dislodges the drug, restoring protein synthesis. Confers cross-resistance to tetracycline, doxycycline, and minocycline but NOT to tigecycline/eravacycline/omadacycline (bulky substituents sterically block Tet(M) binding).
-
Enzymatic inactivation - uncommon; plasmid-encoded modification enzyme; can confer resistance to newer agents.
Intrinsic resistance: Pseudomonas aeruginosa and Proteus spp. are intrinsically resistant due to chromosomally encoded multidrug efflux pumps - this includes tigecycline, eravacycline, and omadacycline.
(Katzung 16e; Harrison's Principles of Internal Medicine 22e; Tietz Textbook of Laboratory Medicine)
Adverse Effects
| Category | Effect |
|---|---|
| GI | Nausea, vomiting, epigastric discomfort, diarrhea; esophagitis/ulcers (take with full glass of water, remain upright) |
| Photosensitivity | Especially doxycycline; onycholysis; sunscreen required |
| Teeth/bone | Permanent brown discoloration of teeth in children <8 years; depressed bone growth; deposition in calcifying tissue |
| Hepatotoxicity | High-dose IV in renal failure or pregnancy; fatty liver |
| Renal/antianabolic | Aggravates azotemia in renal failure; avoid (except doxycycline/minocycline) in renal impairment; Fanconi syndrome with outdated tetracycline |
| Vestibular | Dizziness, vertigo, tinnitus - particularly minocycline |
| C. difficile colitis | Class effect; also Candida vaginitis |
| Tigecycline | Increased all-cause mortality (FDA warning from pooled clinical trial data) |
Contraindications & Precautions
- Pregnancy and lactation - dental/bone effects on fetus/infant
- Children <8 years old - tooth discoloration (exception: compelling indications like Rocky Mountain spotted fever)
- Renal failure - use doxycycline/minocycline if tetracycline class required
- Drug interactions:
- Divalent/trivalent cations (food, dairy, antacids, iron, bismuth) - impair absorption
- Phenytoin, carbamazepine, barbiturates, alcohol - increase doxycycline metabolism (reduces serum levels)
- Digoxin, lithium, warfarin - tetracyclines increase serum levels
- Methoxyflurane anesthesia - combined nephrotoxicity
- Oral contraceptives - theoretical decreased efficacy (GI flora alteration)
(Fitzpatrick's Dermatology 2e; Goodman & Gilman's 14e; Goldman-Cecil Medicine)
Newer Tetracycline Derivatives (3rd/4th Generation)
These were engineered specifically to overcome resistance:
- Tigecycline (glycylcycline): IV only; overcomes both efflux and ribosomal protection; very broad spectrum including MRSA, VRE, anaerobes, MDR gram-negatives; FDA warning for increased mortality; not useful for UTIs or bacteremia (poor urinary/serum levels)
- Eravacycline (fluorocycline): IV; twice daily; similar profile to tigecycline; nausea the main side effect
- Omadacycline (aminomethylcycline): Oral AND IV; once daily; requires empty stomach; good for CAP and SSTIs; promising safety profile
All three retain activity against Tet(M)- and efflux pump-resistant organisms but are still ineffective against Pseudomonas and Proteus.
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics; Katzung's Basic & Clinical Pharmacology, 16e; Harrison's Principles of Internal Medicine, 22e (2025); Fitzpatrick's Dermatology; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.